
Abstract
Clinical outcomes for multiple myeloma (MM) are highly heterogeneous and it is now clear that pivotal genetic events are the primary harbingers of such variation. These findings have broad implications for counseling, choice of therapy and the design and interpretation of clinical investigation. Indeed, as in acute leukemias and non-hodgkins lymphoma, we believe it is no longer acceptable to consider MM a single disease entity. As such, the accurate diagnosis of MM subtypes and the adoption of common criteria for the identification and stratification of MM patients has become critical. Herein, we provide a consensus high-risk definition and offer practical guidelines for the adoption of routine diagnostic testing. Although acknowledging that more refined classifications will continue to be developed, we propose that the definition of high-risk disease (any of the t(4;14), t(14;16), t(14;20), deletion 17q13, aneuploidy or deletion chromosome 13 by metaphase cytogenetics, or plasma cell labeling index >3.0) be adopted. This classification will identify most of the 25% of MM patients for whom current therapies are inadequate and for whom investigational regimens should be vigorously pursued. Conversely, the 75% of patients remaining have more favorable outcomes using existing – albeit non-curative – therapeutic options.
Similar content being viewed by others
Introduction
Multiple myeloma (MM) represents the malignant culmination of the clonal expansion of genetically transformed plasma cells. Several pre malignant stages have been described including monoclonal gammopathy of undetermined significance (MGUS) and smoldering myeloma (SMM).1 The differentiation into stages of progression is most important in distinguishing active MM from the preceding stages, as treatment is usually withheld until actual or impending complications from MM are evident.2 Clinical trials have failed to illustrate any advantage for the initiation of early treatment, and, given the lack of a curative therapy, the delay of treatment until symptomatic progression remains a reasonable strategy.3 These are important points as some of the same genetic features of high-risk MM are also found in MGUS and SMM.4, 5, 6 Thus, the use of ‘high risk’ may rightfully be applied to active and symptomatic disease, but should be used with caution in earlier stages where these findings may potentially predict for early progression but where, in fact, hard data are lacking.
Multiple myeloma remains incurable. Nevertheless, with modern treatment approaches up to 70–90% of patients will respond to their initial therapy and as many as 40–50% may achieve a clinical complete remission.2, 7, 8 Despite this high frequency of early treatment responses, relapse is ubiquitous even for those achieving a clinical complete response and most patients will ultimately succumb to disease progression or complications. However, the timing of relapse is widely variable with some patients progressing almost immediately and some remaining in remission for many years.9 Indeed, even with the earliest clinically applied staging systems, the disease is highly heterogenous.9, 10, 11 For example, review of the SEER database from 1998 to 2002 (http://seer.cancer.gov/) demonstrates somewhat surprisingly that 25% of patients lived less than 1 year and 40% of patients lived less than 2 years. Many of these early deaths presumably reflect advanced age, co existent morbidity and treatment-related toxicities as even ‘high risk’ MM will seldom result in such rapid decline, with the possible exception of primary plasma cell leukemia, which occurs in <5% of patients with a median survival of less than a year.12, 13 As an example of the significant impact of co-morbid conditions, or treatment complications, on mortality, we recently recorded a one-year mortality of 30% in patients presenting in acute renal failure even with aggressive management of renal failure and appropriate anti-MM therapy.14 Most of these patients are never captured in clinical trials, which, then by design, inflate the expected survival of MM patients overall. Even on clinical trials, patients treated with high-dose corticosteroids have an early treatment-related mortality of at least 5%.
This issue aside there is now an abundance of evidence demonstrating that some of the early deaths reflect aggressive genetic features of the underlying disease.6, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28 In contrast, the SEER database also demonstrates that 15% of MM patients were alive 10 years after diagnosis. We will show here that the primary determinant of these heterogeneous patient outcomes are the underlying genetics of the malignant plasma cell and propose that this finding is sufficiently important as to warrant a formal definition of ‘high risk disease’. These definitions have broad implications for the counseling of patients, the choice of therapy and the interpretation of clinical investigation. We believe that clinical trials should now adopt these or similar criteria routinely such that outcome results can be interpreted correctly.
Myeloma genetics synopsis
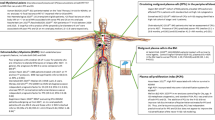
One initial event in the genesis of MM is the translocation of non-random partners that include cyclins D1, D2 and D3, MAF family members (MafA, MafB and c-Maf) and fibroblast growth factor receptor 3 (FGFR3) to the immunoglobulin heavy chain (IgH) switch regions on 14q32.29 These recurrent translocations account for approximately 40% of MM cases. The remaining 60% of MM lack translocations but instead are characterized by chromosomal duplication and a resultant increase in chromosome number – predominantly reflected by trisomies of odd numbered chromosomes – (hyperdiploidy).30, 31, 32 Each of these genetic events (IgH translocation and hyperdiploidy) is then unified by the downstream upregulation of either cyclin D1, D2 or D3.18 This seminal phase of chromosome rearrangement or duplication and disease initiation is followed by further karyotypic instability that often includes deletions/monosomy at chromosome 13q1432, 33, 34 or chromosome 17p13 (p53)26, 28 or amplifications of chromosome 135, 36 or chromosome 8 (MYC).37 Somatic activating mutation in genes such as P53, FGFR3, NRAS and KRAS2 may arise, or secondary translocation may occur by a non-B–cell-mediated mechanisms.32 A common secondary translocation partner is MYC.37 Recently, we have noted mutation of the non-canonical NFkappaB pathway as a common secondary event in up to 40% of patients (PL Bergsagel, unpublished results).
The net effect of these changes and careful examination of their associated gene expression profiles is that MM can be divided into four major transcriptional subgroups (FGFR3/MMSET, MAF, CYCLIN D, HYPERDIPLOID) and for any of these subgroups a dominant proliferation signature may be superimposed.18, 38, 39 In recent analyses the combination of these groupings have variously resulted in seven or eight unique gene expression analyses signatures of newly diagnosed patients with one such signature usually reflecting contaminating non-MM cells.18, 39, 40 Thus, six–seven gene clusters have been defined in the various expression profiling studies.6, 18, 20, 32, 38, 39, 41 In common, however, each of these gene expression-based analyses broadly segregates patients into three highrisk camps – FGFR3/MMSET, MAF and PROLIFERATION.
Genetic features of low-risk disease
t(11;14) and t(6;14) is associated with a neutral prognosis
The t(11;14) and t(6;14) upregulate cyclin D1 and D3, respectively.18, 32, 39, 42, 43 They share a gene expression signature and as such may be considered together, for the purposes of disease biology and clinical outcome.18 Together they represent approximately 20% of all MM patients.18, 39 The presence of the t(11;14) or t(6;14) is associated with an improved or neutral survival in patients treated with conventional or high-dose chemotherapy and stem cell support.23, 28, 39, 44, 45, 46 This good prognosis extends to the most aggressive regimens being employed in MM therapy.39 Arguing against a very favorable prognosis, studies of long-term survivors of MM have not revealed any enrichment for t(11;14) patients.23 There is an association of the t(11;14)(q13;q32) with oligosecretory or light chain only MM, CD20 expression and lymphoplasmacytic morphology.16, 44, 45, 47
Hyperdiploidy is likely to be associated with a favorable prognosis
The presence of hyperdiploidy is generally considered favorable and patients with hyperdiploidy can live for extended periods after high-dose melphalan-based therapies.18, 30, 31, 32, 39, 48, 49 All studies to date have shown superiority in overall survival and progression-free survival for patients with hyperdiploidy, whether this is detected by flow cytometry determination of DNA content, karyotype analysis50, 51, 52 or gene expression profile.6, 39, 53 In a recent publication, we were able to show that this difference in survival was not clearly related to initial responsiveness to treatment (using melphalan based strategies); thus, the difference in outcomes reflects a prolonged remission duration.54 It should be noted that few studies have yet analyzed the impact of hyperdiploidy by multivariant analysis.
Genetic features of high-risk disease
t(4;14) imparts an unfavorable prognosis
Fifteen percent of patients exhibit the t(4;14).21, 22, 24, 28, 39, 44, 55, 56 At least five large studies in over 1500 patients treated with conventional therapy, single or tandem transplant, with or without thalidomide, have demonstrated a uniformly unfavorable prognosis for this group of patients as measured by gene expression, fluorescent in situ hybridization (FISH) or immunohistochemistry.22, 28, 44, 46, 55, 56 This patient population is also present in premalignant MGUS, but is more common in smoldering and active MM. The t(4;14) population is enriched in IgA isotype MM and in cohorts of patients with relapsed disease.28, 39, 57 A large percentage (50–80%) of these patients will have a coexistent deletion of chromosome 13 and are frequently hypodiploid (loss of chromosomes) on conventional cytogenetics.28, 39
t(14;16)and t(14;20) impart an unfavorable prognosis
The t(14;16), t(14;20) and rare t(8;20) are detectable in 6–8% of patients.15, 18, 39, 58, 59, 60, 61 The MAF transcription factor family is transcriptionally upregulated as a result of these translocations. As with the cyclins, the MAF translocation share a gene expression signature and as such may be considered together for the purposes of disease biology and clinical outcome.18, 39 In at least two series of patient this patient cohort was associated with a shorter survival among patients treated with conventional or tandem transplant-based chemotherapy.32, 39, 62, 63 Again this population is enriched for IgA isotype, deletion of chromosome 13 and hypodiploidy.32, 39, 62, 63
Secondary events that alter prognosis
Inactivation of p53(17p13) is associated with a poor prognosis
Deletions of 17p13 are detectable in 10% of patients at diagnosis and are associated with a shorter survival after both conventional and high-dose therapy.25, 26, 28, 46, 63, 64 This deletion is generally considered to be a progression event and is prevalent in plasma cell leukemia and central nervous system MM.25, 32 Again, a number of series have confirmed the very poor prognosis of MM patients with deletion of p53.6, 26, 27, 29, 63 Interestingly, this deletion is not specifically correlated with other high-risk groups particularly t(4;14) that seems almost mutually exclusive.46
Chromosome 13 deletion on metaphase analysis is associated with a poor prognosis
One particularly common genetic marker in MM is deletion of chromosome 13 which is detected in ∼50% of patients with abnormal karyotypes so that it was detectable in 10–20% of all patients overall.32, 34, 65, 66, 67, 68 However, the reported prevalence in MM is 50% when interphase FISH has been applied.54, 55, 56, 65, 66, 67, 68, 69, 70 Independent of the mode of treatment (standard versus high-dose chemotherapy) and the mode of detection (karyotype versus FISH), MM cases with deletion 13 are associated with shorter survival and lower response rate to treatment.32 The net effect of deletion 13 on prognosis is, however, greater when deletion 13 is detected by karyotype than when it is detected by interphase FISH.19 This is owing to the additive effects of the requirement for a proliferative tumor to produce abnormal metaphases. Indeed, when detected by FISH it is only weakly prognostic and is not prognostic at all in some multivariable analysis.46 This later finding reflects the high correlation of chromosome 13 deletion and other high-risk groups – with up to 80% of t(4;14) patients also harboring a deletion 13. Nevertheless, when found during metaphase analysis the prognosis is very poor.
Amplification of chromosome 1
Amplification of chromosome 1 in a region that includes the cks1b gene is common – being found in around 35% of patients – and is considered a progression event.32, 33, 36, 38, 39, 40, 69 CKS1B expression is associated with a proliferation signature in MM patients and by both gene expression profiles and by FISH, it confers a poor prognosis,36, 38, 39, 40 however, this is not significant in multivariate analysis when FISH is employed as the diagnostic criterion. Its prognostic impact seems stronger when gene expression data are employed.
The impact of proliferation and tumor burden
By a variety of different methodologies, the presence of high tumor burden or increased proliferation in MM is generally unfavorable.6, 9, 10, 70, 71, 72, 73, 74, 75, 76, 77 Surrogate markers include the serum LDH71, 78 and beta-2-microglobulin,9, 46, 72, 75, 79 whereas more direct assays include the plasma cell labeling index76, 80, 81 or gene expression-based signatures.39 Indeed, a proliferation signature on gene expression profiling identifies 15% of patients with dismal outcome independent of other risk factors including otherwise favorable genetics.39 Conversely, a low or normal beta-2-microglobulin may identify subsets of FISH-identified high-risk patients (e.g., t(4;14)) in whom prognosis is only marginally worse than for other MM patients.46 The beta-2-microglobulin is commonly employed as a surrogate for tumor burden,9, 76 and likely serves as an adequate, if imperfect, marker of plasma cell number. Indeed, in the recently described international staging system and in a number of other series, the beta-2-microglobulin retains prognostic significance even in multivariate analysis.9, 76
The actual beta-2-microglobulin cutoff used to define high risk has variously been reported as 346 439 or 5.5 mg/l.9 In the absence of other guidance, we have selected >5.5 mg/l as the most conservative interpretation of high-risk disease as fully 34% of MM patients may be found within this group.9 Use of the beta-2-microglobulin alone should then be used cautiously, particularly in the absence of other poor prognostic factors and in the presence of renal failure where poor clearance rather than high tumor burden may be dominant. Although not widely adopted, the plasma cell labeling index76, 80, 81 remains another tool for assessing plasma cell turnover and retains prognostic significance in many models.
The value of routine genetic testing
The summary above has led to our recommended classification of high-risk MM (Table 1). Specifically, independent studies involving over 1500 patients21, 28, 39, 46 have identified a poor prognosis associated with the presence of immunoglobulin heavy chain translocations (t(4;14); t(14;16); t(14;20)), deletion of chromosome 13 by conventional cytogenetics or patients with a clearly proliferative tumor of all genetic stripes. Furthermore, similar large studies have confirmed the favorable prognosis of t(11;14) and t(6;14) or hyperdiploid patients lacking both a proliferation signature and metaphase detected abnormality of chromosome 13 or aneuploidy.
As conventional therapies perform poorly for the 25% of patients (by our definition) with high-risk disease, we now feel confident in endorsing a strong recommendation for the adoption of routine molecular genetic testing in MM patients and a suggested ‘basic’ panel is proposed (Table 2). It is strongly recommended that all newly diagnosed MM patients be tested at a minimum for the t(4;14), t(14;16) and deletion 17p13 by FISH on clonal plasma cells (CD138 selected, cytoplasmic immunoglobulin restricted or morphologically identifiable) to define high-risk disease. Although the t(14;20) and t(8;14) MAF translocations are also likely poor prognosis markers, they are present in a very small fraction of patients (∼2%) and because some of these patients will be picked up by other poor-risk features such as chromosome 13 deletion or aneuploidy, we did not feel it was cost effective to include these diagnostics here. We have retained the deletion of chromosome 13 by metaphase analysis to identify some of this low frequency MAF ‘high risk’ group but also to identify those ‘good risk’ genetic patients who may not fare well owing to acquired secondary genetic events that override the initial genetic insult. Although detection of the presence of the t(11;14) or hyperdiploidy to define low-risk disease is of value, by default in the absence of high–risk genetics, these patients would be considered low-risk and, in the absence of elevated proliferation markers can, for the time being, be lumped together therapeutically. Importantly, the evaluation of low-risk patients should include measurement of the serum beta-2-microglobulin, LDH or PCLI as surrogate markers of tumor burden or proliferation.
The arrival of targeted therapies
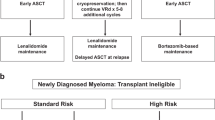
The detection of either t(4;14), t(14;16), deletion of 17p13 (p53) by FISH, deletion of chromosome 13 or aneuploidy on metaphase analysis or PCLI>3 will define a population of ∼25% MM patients who are in a high-risk prognostic group and who do not generally appear to achieve sufficient benefit from conventional autologous stem cell transplant21, 24, 28, 39, 46 to justify the morbidity and cost of the procedure and who should then arguably be steered towards more investigational therapeutic algorithms soon after diagnosis. In particular, the early introduction of bortezomib seems to overcome at least some of the adverse influence of high-risk genetics.82, 83 Alternatively, the 75% of patients under the age of 70 lacking these poor-risk factors are more likely to benefit from a high-dose melphalan-based approach.39, 46 In transplant ineligible patients, a combination of melphalan, prednisone and thalidomide84 is recommended for low-risk patients, but the early introduction of bortezomib82, 83 should be strongly considered for high-risk patients. For some patients, the presence of specific genetic markers may lend themselves to clinical trials of targeted therapies, for example FGFR3 kinase inhibitors.85, 86
Conclusion
We suggest here that a high-risk diagnostic panel should be performed on all newly diagnosed MM patients and the results imparted such that patients may make informed choices regarding therapeutic options. Furthermore, we believe that the collection of this information is imperative in the interpretation of current and future clinical trials and should be immediately adopted in trial design.
References
Kyle RA, Rajkumar SV . Monoclonal gammopathies of undetermined significance. Best Pract Res Clin Haematol 2005; 18: 689–707.
Kyle RA, Rajkumar SV . Multiple myeloma. N Engl J Med 2004; 351: 1860–1873.
Dispenzieri A, Kyle RA . Multiple myeloma: clinical features and indications for therapy. Best Pract Res Clin Haematol 2005; 18: 553–568.
Avet-Loiseau H, Li JY, Morineau N, Facon T, Brigaudeau C, Harousseau JL et al. Monosomy 13 is associated with the transition of monoclonal gammopathy of undetermined significance to multiple myeloma. Intergroupe Francophone du Myelome. Blood 1999; 94: 2583–2589.
Fonseca R, Bailey RJ, Ahmann GJ, Rajkumar SV, Hoyer JD, Lust JA et al. Genomic abnormalities in monoclonal gammopathy of undetermined significance. Blood 2002; 100: 1417–1424.
Zhan F, Hardin J, Kordsmeier B, Bumm K, Zheng M, Tian E et al. Global gene expression profiling of multiple myeloma, monoclonal gammopathy of undetermined significance, and normal bone marrow plasma cells. Blood 2002; 99: 1745–1757.
Barlogie B, Tricot G, Rasmussen E, Anaissie E, van Rhee F, Zangari M et al. Total therapy 2 without thalidomide in comparison with total therapy 1: Role of intensified induction and posttransplantation consolidation therapies. Blood 2006; 107: 2633–2638.
Richardson PG, Mitsiades CS, Hideshima T, Anderson KC . Novel biological therapies for the treatment of multiple myeloma. Best Pract Res Clin Haematol 2005; 18: 619–634.
Greipp PR, San Miguel J, Durie BG, Crowley JJ, Barlogie B, Blade J et al. International staging system for multiple myeloma. J Clin Oncol 2005; 23: 3412–3420.
Jacobson JL, Hussein MA, Barlogie B, Durie BG, Crowley JJ . A new staging system for multiple myeloma patients based on the Southwest Oncology Group (SWOG) experience. Br J Haematol 2003; 122: 441–450.
Ong F, Hermans J, Noordijk EM, Kluin-Nelemans JC . Is the Durie and Salmon diagnostic classification system for plasma cell dyscrasias still the best choice? Application of three classification systems to a large population-based registry of paraproteinemia and multiple myeloma. Ann Hematol 1995; 70: 19–24.
Jimenez-Zepeda VH, Dominguez VJ . Plasma cell leukemia: a rare condition. Ann Hematol 2006; 85: 263–267.
Saccaro S, Fonseca R, Veillon DM, Cotelingam J, Nordberg ML, Bredeson C et al. Primary plasma cell leukemia: report of 17 new cases treated with autologous or allogeneic stem-cell transplantation and review of the literature. Am J Hematol 2005; 78: 288–294.
Clark WF, Stewart AK, Rock GA, Sternbach M, Sutton DM, Barrett BJ et al. Plasma exchange when myeloma presents as acute renal failure: a randomized, controlled trial. Ann Intern Med 2005; 143: 777–784.
Avet-Loiseau H, Li JY, Facon T, Brigaudeau C, Morineau N, Maloisel F et al. High incidence of translocations t(11;14)(q13;q32) and t(4;14)(p16;q32) in patients with plasma cell malignancies. Cancer Res 1998; 58: 5640–5645.
Avet-Loiseau H, Garand R, Lode L, Harousseau JL, Bataille R . Translocation t(11;14)(q13;q32) is the hallmark of IgM, IgE, and nonsecretory multiple myeloma variants. Blood 2003; 101: 1570–1571.
Bergsagel PL, Kuehl WM . Critical roles for immunoglobulin translocations and cyclin D dysregulation in multiple myeloma. Immunol Rev 2003; 194: 96–104.
Bergsagel PL, Kuehl WM, Zhan F, Sawyer J, Barlogie B, Shaughnessy Jr J . Cyclin D dysregulation: an early and unifying pathogenic event in multiple myeloma. Blood 2005; 106: 296–303.
Stewart AK, Fonseca R . Prognostic and therapeutic significance of myeloma genetics and gene expression profiling. J Clin Oncol 2005; 23: 6339–6344.
Shaughnessy Jr J, Zhan F, Barlogie B, Stewart AK . Gene expression profiling and multiple myeloma. Best Pract Res Clin Haematol 2005; 18: 537–552.
Chang H, Sloan S, Li D, Zhuang L, Yi QL, Chen CI et al. The t(4;14) is associated with poor prognosis in myeloma patients undergoing autologous stem cell transplant. Br J Haematol 2004; 125: 64–68.
Chang H, Stewart AK, Qi XY, Li ZH, Yi QL, Trudel S . Immunohistochemistry accurately predicts FGFR3 aberrant expression and t(4;14) in multiple myeloma. Blood 2005; 106: 353–355.
Chang H, Qi XY, Stewart AK . t(11;14) does not predict long-term survival in myeloma. Leukemia 2005; 19: 1078–1079.
Chang H, Qi XY, Samiee S, Yi QL, Chen C, Trudel S et al. Genetic risk identifies multiple myeloma patients who do not benefit from autologous stem cell transplantation. Bone Marrow Transplant 2005; 36: 793–796.
Chang H, Sloan S, Li D, Keith Stewart A . Multiple myeloma involving central nervous system: high frequency of chromosome 17p13.1 (p53) deletions. Br J Haematol 2004; 127: 280–284.
Chang H, Qi C, Yi QL, Reece D, Stewart AK . p53 gene deletion detected by fluorescence in situ hybridization is an adverse prognostic factor for patients with multiple myeloma following autologous stem cell transplantation. Blood 2005; 105: 358–360.
Chang H, Bouman D, Boerkoel CF, Stewart AK, Squire JA . Frequent monoallelic loss of D13S319 in multiple myeloma patients shown by interphase fluorescence in situ hybridization. Leukemia 1999; 13: 105–109.
Gertz MA, Lacy MQ, Dispenzieri A, Greipp PR, Litzow MR, Henderson KJ et al. Clinical implications of t(11;14)(q13;q32), t(4;14)(p16.3;q32), and −17p13 in myeloma patients treated with high-dose therapy. Blood 2005; 106: 2837–2840.
Bergsagel PL, Kuehl WM . Chromosome translocations in multiple myeloma. Oncogene 2001; 20: 5611–5622.
Chng WJ, Van Wier SA, Ahmann GJ, Winkler JM, Jalal SM, Bergsagel PL et al. A validated FISH trisomy index demonstrates the hyperdiploid and non-hyperdiploid dichotomy in MGUS. Blood 2005; 106: 2156–2161.
Chng WJ, Winkler JM, Greipp PR, Jalal SM, Bergsagel PL, Chesi M et al. Ploidy status rarely changes in myeloma patients at disease progression. Leuk Res 2006; 30: 266–271.
Fonseca R, Barlogie B, Bataille R, Bastard C, Bergsagel PL, Chesi M et al. Genetics and cytogenetics of multiple myeloma: a workshop report. Cancer Res 2004; 64: 1546–1558.
Shaughnessy J, Jacobson J, Sawyer J, McCoy J, Fassas A, Zhan F et al. Continuous absence of metaphase-defined cytogenetic abnormalities, especially of chromosome 13 and hypodiploidy, ensures long-term survival in multiple myeloma treated with Total Therapy I: interpretation in the context of global gene expression. Blood 2003; 101: 3849–3856.
Shaughnessy J, Barlogie B . Chromosome 13 deletion in myeloma. Curr Top Microbiol Immunol 1999; 246: 199–203.
Hanamura I, Stewart JP, Huang Y, Zhan F, Santra M, Sawyer JR et al. Frequent gain of chromosome band 1q21 in plasma-cell dyscrasias detected by fluorescence in situ hybridization: incidence increases from MGUS to relapsed myeloma and is related to prognosis and disease progression following tandem stem-cell transplantation. Blood 2006; 108: 1724–1732.
Shaughnessy J . Amplification and overexpression of CKS1B at chromosome band 1q21 is associated with reduced levels of p27Kip1 and an aggressive clinical course in multiple myeloma. Hematology 2005; 10 (Suppl 1): 117–126.
Kuehl WM, Brents LA, Chesi M, Huppi K, Bergsagel PL . Dysregulation of c-myc in multiple myeloma. Curr Top Microbiol Immunol 1997; 224: 277–282.
Shaughnessy Jr JD, Barlogie B . Using genomics to identify high-risk myeloma after autologous stem cell transplantation. Biol Blood Marrow Transplant 2006; 12 (Suppl 1): 77–80.
Zhan F, Huang Y, Colla S, Stewart JP, Hanamura I, Gupta S et al. The molecular classification of multiple myeloma. Blood 2006; 108: 2020–2028.
Agnelli L, Bicciato S, Mattioli M, Fabris S, Intini D, Verdelli D et al. Molecular classification of multiple myeloma: a distinct transcriptional profile characterizes patients expressing CCND1 and negative for 14q32 translocations. J Clin Oncol 2005; 23: 7296–7306.
Carrasco DR, Tonon G, Huang Y, Zhang Y, Sinha R, Feng B et al. High-resolution genomic profiles define distinct clinico-pathogenetic subgroups of multiple myeloma patients. Cancer Cell 2006; 9: 313–325.
Chesi M, Bergsagel PL, Brents LA, Smith CM, Gerhard DS, Kuehl WM . Dysregulation of cyclin D1 by translocation into an IgH gamma switch region in two multiple myeloma cell lines. Blood 1996; 88: 674–681.
Shaughnessy Jr J, Gabrea A, Qi Y, Brents L, Zhan F, Tian E et al. Cyclin D3 at 6p21 is dysregulated by recurrent chromosomal translocations to immunoglobulin loci in multiple myeloma. Blood 2001; 98: 217–223.
Fonseca R, Blood EA, Oken MM, Kyle RA, Dewald GW, Bailey RJ et al. Myeloma and the t(11;14)(q13;q32); evidence for a biologically defined unique subset of patients. Blood 2002; 99: 3735–3741.
Hoyer JD, Hanson CA, Fonseca R, Greipp PR, Dewald GW, Kurtin PJ . The (11;14)(q13;q32) translocation in multiple myeloma. A morphologic and immunohistochemical study. Am J Clin Pathol 2000; 113: 831–837.
Avet-Loiseau H, Attal M, Moreau P, Charbonnel C, Garban F, Harousseau J et al. A comprehensive analysis of cytogenetic abnormalities in myeloma: results of the FISH analysis of 1000 patients enrolled in the IFM99 trials. session type: oral session. Blood 2005; 106: 622.
Fonseca R, Hoyer JD, Aguayo P, Jalal SM, Ahmann GJ, Rajkumar SV et al. Clinical significance of the translocation (11;14)(q13;q32) in multiple myeloma. Leuk Lymphoma 1999; 35: 599–605.
Wuilleme S, Robillard N, Lode L, Magrangeas F, Beris H, Harousseau JL et al. Ploidy, as detected by fluorescence in situ hybridization, defines different subgroups in multiple myeloma. Leukemia 2005; 19: 275–278.
Chng WJ, Van Wier SA, Ahmann GJ, Winkler JM, Jalal SM, Bergsagel PL et al. A validated FISH trisomy index demonstrates the hyperdiploid and nonhyperdiploid dichotomy in MGUS. Blood 2005; 106: 2156–2161.
Debes-Marun CS, Dewald GW, Bryant S, Picken E, Santana-Davila R, Gonzalez-Paz N et al. Chromosome abnormalities clustering and its implications for pathogenesis and prognosis in myeloma. Leukemia 2003; 17: 427–436.
Smadja NV, Bastard C, Brigaudeau C, Leroux D, Fruchart C . Hypodiploidy is a major prognostic factor in multiple myeloma. Blood 2001; 98: 2229–2238.
Garcia-Sanz R, Orfao A, Gonzalez M, Moro MJ, Hernandez JM, Ortega F et al. Prognostic implications of DNA aneuploidy in 156 untreated multiple myeloma patients. Castelano-Leones (Spain) cooperative group for the study of monoclonal gammopathies. Br J Haematol 1995; 90: 106–112.
Zhan F, Tian E, Bumm K, Smith R, Barlogie B, Shaughnessy Jr J . Gene expression profiling of human plasma cell differentiation and classification of multiple myeloma based on similarities to distinct stages of late-stage B-cell development. Blood 2003; 101: 1128–1140.
Chng WJ, Santana-Davila R, Van Wier SA, Ahmann GJ, Jalal SM, Bergsagel PL et al. Prognostic factors for hyperdiploid-myeloma: effects of chromosome 13 deletions and IgH translocations. Leukemia 2006; 20: 807–813.
Fonseca R, Oken MM, Greipp PR . The t(4;14)(p16.3;q32) is strongly associated with chromosome 13 abnormalities in both multiple myeloma and monoclonal gammopathy of undetermined significance. Blood 2001; 98: 1271–1272.
Fonseca R, Oken MM, Harrington D, Bailey RJ, Van Wier SA, Henderson KJ et al. Deletions of chromosome 13 in multiple myeloma identified by interphase FISH usually denote large deletions of the q arm or monosomy. Leukemia 2001; 15: 981–986.
Jaksic W, Trudel S, Chang H, Trieu Y, Qi X, Mikhael J et al. Clinical outcomes in t(4;14) multiple myeloma: a chemotherapy-sensitive disease characterized by rapid relapse and alkylating agent resistance. J Clin Oncol 2005; 23: 7069–7073.
Hurt EM, Wiestner A, Rosenwald A, Shaffer AL, Campo E, Grogan T et al. Overexpression of c-maf is a frequent oncogenic event in multiple myeloma that promotes proliferation and pathological interactions with bone marrow stroma. Cancer Cell 2004; 5: 191–199.
Chesi M, Kuehl WM, Bergsagel PL . Recurrent immunoglobulin gene translocations identify distinct molecular subtypes of myeloma. Ann Oncol 2000; 11 (Suppl 1): 131–135.
Chesi M, Bergsagel PL, Shonukan OO, Martelli ML, Brents LA, Chen T et al. Frequent dysregulation of the c-maf proto-oncogene at 16q23 by translocation to an Ig locus in multiple myeloma. Blood 1998; 91: 4457–4463.
Rasmussen T, Knudsen LM, Dahl IM, Johnsen HE . C-MAF oncogene dysregulation in multiple myeloma: frequency and biological relevance. Leuk Lymphoma 2003; 44: 1761–1766.
Fonseca R, Debes-Marun CS, Picken EB, Dewald GW, Bryant SC, Winkler JM et al. The recurrent IgH translocations are highly associated with nonhyperdiploid variant multiple myeloma. Blood 2003; 102: 2562–2567.
Fonseca R, Blood E, Rue M, Harrington D, Oken MM, Kyle RA et al. Clinical and biologic implications of recurrent genomic aberrations in myeloma. Blood 2003; 101: 4569–4575.
Chang H, Qi XY, Samiee S, Yi QL, Chen C, Trudel S et al. Genetic risk identifies multiple myeloma patients who do not benefit from autologous stem cell transplantation. Bone Marrow Transplant 2005; 36: 793–796.
Shaughnessy Jr J, Tian E, Sawyer J, McCoy J, Tricot G, Jacobson J et al. Prognostic impact of cytogenetic and interphase fluorescence in situ hybridization-defined chromosome 13 deletion in multiple myeloma: early results of total therapy II. Br J Haematol 2003; 120: 44–52.
Fassas AB, Spencer T, Sawyer J, Zangari M, Lee CK, Anaissie E et al. Both hypodiploidy and deletion of chromosome 13 independently confer poor prognosis in multiple myeloma. Br J Haematol 2002; 118: 1041–1047.
Sawyer JR, Waldron JA, Jagannath S, Barlogie B . Cytogenetic findings in 200 patients with multiple myeloma. Cancer Genet Cytogenet 1995; 82: 41–49.
Tricot G, Sawyer JR, Jagannath S, Desikan KR, Siegel D, Naucke S et al. Unique role of cytogenetics in the prognosis of patients with myeloma receiving high-dose therapy and autotransplants. J Clin Oncol 1997; 15: 2659–2666.
Sawyer JR, Tricot G, Lukacs JL, Binz RL, Tian E, Barlogie B et al. Genomic instability in multiple myeloma: evidence for jumping segmental duplications of chromosome arm 1q. Genes Chromosomes Cancer 2005; 42: 95–106.
Desikan KR, Tricot G, Munshi NC, Anaissie E, Spoon D, Fassas A et al. Preceding chemotherapy, tumour load and age influence engraftment in multiple myeloma patients mobilized with granulocyte colony-stimulating factor alone. Br J Haematol 2001; 112: 242–247.
Barlogie B, Smallwood L, Smith T, Alexanian R . High serum levels of lactic dehydrogenase identify a high-grade lymphoma-like myeloma. Ann Intern Med 1989; 110: 521–525.
Alexanian R, Barlogie B, Fritsche H . Beta 2 microglobulin in multiple myeloma. Am J Hematol 1985; 20: 345–351.
Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, Dispenzieri A et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc 2003; 78: 21–33.
Pardanani A, Witzig TE, Schroeder G, McElroy EA, Fonseca R, Dispenzieri A et al. Circulating peripheral blood plasma cells as a prognostic indicator in patients with primary systemic amyloidosis. Blood 2003; 101: 827–830.
Rajkumar SV, Fonseca R, Lacy MQ, Witzig TE, Lust JA, Greipp PR et al. Beta2-microglobulin and bone marrow plasma cell involvement predict complete responders among patients undergoing blood cell transplantation for myeloma. Bone Marrow Transplant 1999; 23: 1261–1266.
Greipp PR, Lust JA, O'Fallon WM, Katzmann JA, Witzig TE, Kyle RA . Plasma cell labeling index and beta 2-microglobulin predict survival independent of thymidine kinase and C-reactive protein in multiple myeloma. Blood 1993; 81: 3382–3387.
Gertz MA, Kyle RA, Greipp PR, Katzmann JA, O'Fallon WM . Beta 2-microglobulin predicts survival in primary systemic amyloidosis. Am J Med 1990; 89: 609–614.
Dimopoulos MA, Barlogie B, Smith TL, Alexanian R . High serum lactate dehydrogenase level as a marker for drug resistance and short survival in multiple myeloma. Ann Intern Med 1991; 115: 931–935.
Tricot G, Spencer T, Sawyer J, Spoon D, Desikan R, Fassas A et al. Predicting long-term (> or =5 years) event-free survival in multiple myeloma patients following planned tandem autotransplants. Br J Haematol 2002; 116: 211–217.
Rajkumar SV, Fonseca R, Dewald GW, Therneau TM, Lacy MQ, Kyle RA et al. Cytogenetic abnormalities correlate with the plasma cell labeling index and extent of bone marrow involvement in myeloma. Cancer Genet Cytogenet 1999; 113: 73–77.
Steensma DP, Gertz MA, Greipp PR, Kyle RA, Lacy MQ, Lust JA et al. A high bone marrow plasma cell labeling index in stable plateau-phase multiple myeloma is a marker for early disease progression and death. Blood 2001; 97: 2522–2523.
Mateos MV, Hernandez JM, Hernandez MT, Gutierrez NC, Palomera L, Fuertes M et al. Bortezomib plus melphalan and prednisone in elderly untreated patients with multiple myeloma: results of a multicenter phase I/II study. Blood 2006; 108: 2165–2172.
Richardson PG, Barlogie B, Berenson J, Singhal S, Jagannath S, Irwin D et al. Clinical factors predictive of outcome with bortezomib in patients with relapsed, refractory multiple myeloma. Blood 2005; 106: 2977–2981.
Palumbo A, Bertola A, Musto P, Caravita T, Callea V, Nunzi M et al. Oral melphalan, prednisone, and thalidomide for newly diagnosed patients with myeloma. Cancer 2005; 104: 1428–1433.
Trudel S, Stewart AK, Rom E, Wei E, Li ZH, Kotzer S et al. The inhibitory anti-FGFR3 antibody, PRO-001 is cytotoxic to t(4;14) multiple myeloma cells. Blood 2006; 107: 4039–4046.
Trudel S, Li ZH, Wei E, Wiesmann M, Chang H, Chen C et al. CHIR-258, a novel, multitargeted tyrosine kinase inhibitor for the potential treatment of t(4;14) multiple myeloma. Blood 2005; 105: 2941–2948.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Stewart, A., Bergsagel, P., Greipp, P. et al. A practical guide to defining high-risk myeloma for clinical trials, patient counseling and choice of therapy. Leukemia 21, 529–534 (2007). https://doi.org/10.1038/sj.leu.2404516
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.leu.2404516
