
Abstract
Objectives:
To determine the natural course of spinal cord injury (SCI) after aortic aneurysm surgery.
Setting:
Acute care and semi-acute wards in Osaka Rosai Hospital, Japan.
Methods:
From 1998 to 2003, 12 patients with thoracic SCI (eight men and four women; mean age: 69 years) were enrolled and evaluated by the American Spinal Injury Association (ASIA) impairment scale and Functional Independence Measure (FIM), and the results were analyzed.
Results:
The level of SCI was distributed from T5 to L1. The ASIA impairment scale was A in four patients, B in four, C in three and D in one. Finally, six patients were discharged to home, and two patients died during hospitalization. Excluding the value of the deceased patients, the mean motor FIM was initially 32±15.6 (13–59) points and became 61±21.4 (29–88) points at discharge. Referencing the databases of SCI in Japan and USA revealed that the complication rates of pneumonia and aspiration were higher in our cases. The motor FIM before rehabilitation and at discharge were relatively lower than in the databases, but the gain and the rate of gain were similar to the Japanese database.
Conclusion:
SCI associated with aortic aneurysm surgery was noticed especially in the elderly patients using airways (for example, tracheostomy). The higher age and recurrent nerve palsy were associated with deconditioning state to develop aspiration pneumonia. This state impaired the general condition, and such vicious cycle led to poor prognosis and functional outcome.
Similar content being viewed by others


Introduction
Aortic aneurysm sometimes causes thoracic spinal cord infarction with thoracic spinal artery occlusion.1, 2, 3 Renal and respiratory failures also sometimes occur. The incidence of left recurrent nerve palsy (RNP) was 8.6% in a study on 500 patients4 and 5% in another study on 168 cases.5 Most of the patients with the above-mentioned syndrome were elderly. Therefore, the rehabilitation is difficult in contrast to that for the young patients with traumatic spinal cord injury (SCI).6, 7 We rehabilitated several patients with thoracic SCI after aortic aneurysm operation. The results and problems are discussed herein.
Patients and methods
From 1998 to 2003, we treated 12 patients with medical rehabilitation in our hospital. There were eight men and four women, and their mean age was 69 years (range: 55–80 years). They were diagnosed as having thoracic aortic aneurysm (TAA; eight cases) and dissecting aneurysm (DA; four cases). The patients' details are shown in Table 1. The Functional Independence Measure (FIM)8, 9 and American Spinal Injury Association (ASIA)10, 11 impairment scale (AIS) were used for clinical evaluation.
Results
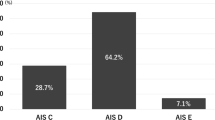
The level of SCI was distributed from T5 to L1 as shown in Table 1. Six patients were injured at T5 and T6 levels, and were classified as the upper thoracic group, while the other six had injury at T8–L1 levels and were classified as the lower thoracic group. Their impairments were classified into A, four cases; B, four cases; C, three cases; and D, one case, according to AIS. Regarding the final results, six patients were discharged, four were referred to another hospital, while two died.
Two elderly patients (78 and 80 years old) died during hospitalization. Both of them had TAA complicated with aspiration pneumonia. One of them had intubation and the other underwent mini-tracheostomy. One of them had RNP that was diagnosed postoperatively with laryngoscope. Both of them had a long smoking history. One of them had a history of bronchial asthma. They also had renal failure, and one of them was under hemodialysis (HD). Their poor general condition led to delay of rehabilitation start. Only range of motion exercises were performed in the intensive care unit. They also had sacral decubitus due to deterioration of their general condition and long bed rest. The clinical course in both cases was 5 months, one died of tracheal bleeding and the other died of hypotension during HD.
Postoperatively, rehabilitation was started within 1 month. The patients, transferred to our hospital after operation, had delay in the start of rehabilitation because the rehabilitation beds for the patients with SCI are limited. The ASIA motor score at the beginning of rehabilitation was 62.2±15.0 (39–83) points, improved by 8.2±10.2 (3–32) points and became 70.0±16.3 (50–94) points at discharge. The AIS score of the patients did not change during the hospital rehabilitation. The motor FIM at the beginning of rehabilitation was 31.9±15.4 (13–59) points, improved by 28.6±13.1 (1–46) points, and became 60.5±21.4 (29–88) points at discharge. Four patients were referred to another hospital. In one patient, dehiscence of the surgical wound started, and he was sent back to the original hospital where operation was performed. The other three were transferred to a long-term care hospital like nursing home.
Complications
Renal failure and RNP occurred in four and seven cases, respectively, before rehabilitation. In five out of the latter seven cases, RNP probably developed perioperatively. Postoperatively, five patients had respiratory failure that was managed with intubation, tracheostomy or mini-tracheostomy. Sacral decubitus developed in eight patients. Most of them had slightly reddish skin on the sacral region without ulcer formation.
Factors influencing outcome
Statistical analysis was not conducted because of small number of cases. However, to find out the factors influencing the patient's function at discharge and the place to discharge, we selected some factors; namely, gender, diagnosis (TAA or DA), preoperative lung disease, smoking history, hypertension, HD, airway (tracheostomy, intubation, mini-tracheostomy), RNP, dysphagia, pneumonia, level of SCI (upper and lower thoracic groups), decubitus and chronic pain. The scores of the two deceased patients were excluded from the analysis. As shown in Table 2, we compared the gain of the motor FIM (during hospitalization) and the rate of this gain. The gain of the motor FIM seemed to be lower with airway intervention, dysphagia and pneumonia. The independent patients at home had a mean gain of motor FIM of 39 points, and their rate of improvement was also very high when compared to the other patients. The good and fast functional improvement allowed them to return to their home enjoying independent living.
Discussion
Referencing the databases of SCI in Japan6, 7 and USA12, 13, 14, 15, 16, 17 revealed that the complication rates of pneumonia and aspiration were higher in our cases. The motor FIM before rehabilitation and that at discharge were relatively lower than in the databases (Table 3). The gain and the rate of gain during hospitalization were also less than those in the databases. Finally, SCI associated with aortic aneurysm operation was especially noticed in the elderly persons using airways such as intubation, tracheostomy or mini-tracheostomy. Because of the long operation time, the tracheal secretion increased, resulting in longer stay in the intensive care unit and worse deconditioning state. Deterioration of the swallowing activity in the elderly patients18 and impairment of expectoration due to paraplegia resulted in aspiration pneumonia. The above-mentioned state easily worsened the general condition, and such vicious cycle led to a poor prognosis.
The anatomy of the left recurrent nerve makes it vulnerable to injury as it courses around the aortic arch.4, 5 RNP was reported by Ortner 100 years ago.19, 20 Aspiration caused by RNP was also reported.21, 22 In the patients with SCI, coughing, which prevents aspiration pneumonia, is impaired. We thought that the upper thoracic SCI patients would have lower ability of coughing and breathing, but there were no differences in the outcomes between the upper thoracic palsy and lower thoracic palsy groups. This means that the devastating disease, that is, paraplegia, severely influenced all patients especially the elderly who died during hospitalization.
The incidence of pressure sores was very high in our series. In the Japanese database, this incidence is 45.4% in the complete SCI patients aged 30 years or higher, and 17.3% in those aged below 30 years. However, the United States database showed no difference in the age, and the rate was 23.7%. These results may be attributed to the smaller nursing facilities in Japan.
The final outcome in our series was poor. Only one-third of the patients were independent in their homes. One of the reasons is that the caregiver was old, too. This poor care potential led to a long-term care in hospitals.
In conclusion, SCI associated with aortic aneurysm surgery was noticed especially in the elderly patients, who likely tend to have respiratory dependency or application of airways (for example, tracheostomy). The higher age and RNP were associated with deconditioning state resulting in aspiration pneumonia. This state impaired the general condition, and such vicious cycle led to poor prognosis and functional outcome.
References
Crawford ES, Fenstermacher JM, Richardson W, Sandiford F . Reappraisal of adjuncts to avoid ischemia in the treatment of thoracic aortic aneurysms. Surgery 1970; 67: 182–196.
Grace RR, Mattox KL . Anterior spinal artery syndrome following abdominal aortic aneurysmectomy. Case report and review of the literature. Arch Surg 1977; 112: 813–815.
Sliwa JA, Maclean IC . Ischemic myelopathy: a review of spinal vasculature and related clinical syndrome. Arch Phys Med Rehabil 1992; 73: 365–372.
De Bakey ME, McCollum CH, Graham JM . Surgical treatment of aneurysms of the descending thoracic aorta. Long-term results in 500 patients. J Cardiovas Surg 1978; 19: 571–576.
Teixido MT, Leonetti JP . Recurrent laryngeal nerve paralysis associated with thoracic aortic aneurysm. Otolaryngol Head Neck Surg 1990; 102: 140–144.
Sumida M, Fujimoto M, Tokuhiro A, Tominaga T, Magara A, Uchida R . Early rehabilitation effect for traumatic spinal cord injury. Arch Phys Med Rehabil 2001; 82: 391–395.
Sumida M, Tokuhiro A, Magara A, Toyonaga T, Uchida R . Clinical Outcome of Spinal Cord Injury. Ishiyaku Publishers: Tokyo, 2001.
Granger CV, Hamilton BB, Keith RA, Zielezny M, Sherwin FS . Advances in functional assessment for medical rehabilitation. Top Geriatr Rehabil 1986; 1: 59–74.
Ottenbacher KJ, Hsu Y, Granger CV, Fiedler RC . The reliability of the functional independence measure: a quantitative review. Arch Phys Med Rehabil 1996; 77: 1226–1232.
Ditunno Jr JF, Young W, Donovan WH, Creasey G . The international standards booklet for neurological and functional classification of spinal cord injury. Paraplegia 1994; 32: 70–80.
Maynard Jr FM, Bracken MB, Creasey G, Ditunno Jr JF, Donovan WH, Ducker TB . et al. International standards for neurological and functional classification of spinal cord injury. Spinal Cord 1997; 35: 266–274.
Eastwood EA, Hagglund KJ, Ragnarsson KT, Gordon WA, Marino RJ . Medical rehabilitation length of stay and outcomes for persons with traumatic spinal cord injury – 1990–1997. Arch Phys Med Rehabil 1999; 80: 1457–1463.
Hall KM, Cohen ME, Wright J, Call M, Werner P . Characteristics of the functional independence measure in traumatic spinal cord injury. Arch Phys Med Rehabil 1999; 80: 1471–1476.
Chen D, Apple DF, Hudson LM, Bode R . Medical complications during acute rehabilitation following spinal cord injury – current experience of the model systems. Arch Phys Med Rehabil 1999; 80: 1397–1401.
Graves DE, Frankiewicz RG, Carter RE . Gain in functional ability during medical rehabilitation as related to rehabilitation process indices and neurologic measures. Arch Phys Med Rehabil 1999; 80: 1464–1470.
Marino RJ, Ditunno Jr JF, Donovan WH, Maynard Jr F . Neurologic recovery after traumatic spinal cord injury: data from the model spinal cord injury systems. Arch Phys Med Rehabil 1999; 80: 1391–1396.
DeVivo MJ, Stuart Krause J, Lammertse DP . Recent trends in mortality and causes of death among persons with spinal cord injury. Arch Phys Med Rehabil 1999; 80: 1411–1419.
Robbins J, Hamilton JW, Lof GL, Kempster GB . Oropharyngeal swallowing in normal adults of different ages. Gastroenterology 1992; 103: 823–829.
Ortner N . Recurrenslaehmung bei Mitralstenose. Wei Klin Woch 1897; 33: 753–755.
Thirlwall AS . Ortner's syndrome: a centenary review of unilateral recurrent laryngeal nerve palsy secondary to cardiothoracic disease. J Laryngol Otol 1997; 111: 869–871.
Heitmiller RF, Tseng E, Jones B . Prevalence of aspiration and laryngeal penetration in patients with unilateral vocal fold motion impairment. Dysphagia 2000; 15: 181–187.
Périé S, Laccourreye O, Bou-Malhab F, Brasnu D . Aspiration in unilateral recurrent laryngeal nerve paralysis after surgery. Am J Otolaryngol 1998; 19: 18–23.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ohsawa, S., Tamaki, M. & Hirabayashi, S. Medical rehabilitation of the patients with spinal cord injury caused by aortic aneurysm and its operation. Spinal Cord 46, 150–153 (2008). https://doi.org/10.1038/sj.sc.3102075
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3102075
