
Key Points
-
'Occlusal sketch' is a simple and inexpensive technique for recording oclusal contacts.
-
The 'occlusal sketch' shows a high degree of inter- and intra-operator reliability.
-
This technique could be useful for researchers who wish to quantify occlusal changes during different treatment modalities.
-
'Occlusal sketch' can be used, by practising dentists, as a permanent record of the patient's occlusion.
Abstract
Objectives To develop a simple way of recording occlusal contacts with proven inter- and intra-operator reliability.
Setting Clinical skills laboratory in the University Dental Hospital of Manchester.
Materials and methods The marked static occlusal contacts of 20 sets of models were recorded in a pseudo-clinical situation, by three dentists and in addition by one dentist on two occasions using a schematic representation of the dental arch – the 'occlusal sketch'.
Results The median of Kappa agreement for inter- and intra-operator reliability was almost perfect.
Conclusions The occlusal sketch is a simple, inexpensive and easy way of recording the results of an occlusal examination using marking papers.
Similar content being viewed by others

Main
A simple and reliable means of recording the results of an occlusal examination is important not only in relation to clinical dentistry but is also a consideration in dental research.1,2,3,4 Unless an occlusal record is accurate any change in occlusion cannot be evaluated.5
There is confusion surrounding the use of the terms 'examination', 'record' and 'registration'. For the purposes of this paper the following definitions will be used:
Occlusal examination: An investigation of the occlusal contacts by inspection.
Occlusal record: Preservation of the results of an occlusal exami-nation; this may be two dimensional (eg written record, photo-graph, computer representation drawing or sketch).
Occlusal registration: A physical record which by determining the jaw relationships (existing or desired) allows for the transfer of upper and lower models to an articulator in that jaw relationship.
All bite registration materials have drawbacks.6 Even if a registration is accurate there remains the problem of storage and easy retrieval. Alternative means of recording occlusions include photosensitive films and pressure sensitive wafers.7
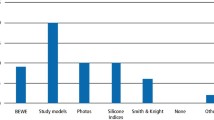
Examination of occlusal contacts is often made using marking papers and ribbons, but this does not constitute a record that can be stored for future reference. Some method is required to transfer the results of this examination to a permanent record and a review of the literature indicates the variety of techniques that have been employed (Table 1).
The aims of the study
The principal aim of this study was to test whether an acetate sheet 'occlusal sketch' could be used as an accurate and reproducible means of recording occlusal contacts, previously marked by articulating paper.
The trial was divided into two tests:
1. Inter-operator reliability:
Do different operators place marks onto a schematic representation of teeth, 'the occlusal sketch', in the same places when viewing occlusal marks?
2. Intra-operator reliability:
Does the same operator similarly place the same marks on the sketch when viewing an unchanged occlusal scheme at different times?
Materials and methods
The occlusal sketch (Fig. 1) is an acetate sheet on which is drawn a schematic representation of the teeth (the occlusal surfaces of the posterior teeth, the palatal surfaces of the upper anterior teeth and the labial surfaces of the lower anterior teeth). It is configured so that the lower arch is viewed as if from above by direct vision and the upper arch is a mirror image. This is the same view as experienced in a clinical examination of a supine patient.

The occlusal sketch acetate sheet marked on a 1mm2 grid
The 'occlusal sketch' is made from transparent acetate rather than paper because the technique has been used, for a number of years, by one of the authors in restorative dentistry as a clinical procedure to facilitate the transmission of occlusal information between dentist and dental technician. In this application it is important that the sketch can be viewed from both sides.19
Inter-operator reliability
Twenty sets of upper and lower plaster models were mounted in centric occlusion in a Denar articulator after facebow record. These models were mounted in centric occlusion. The contacts of the static occlusion were marked using thin articulating paper (Bausch occlusion paper 40 μ, blue) because thicker paper would lead to inaccuracy. The paper was supported by a paper holder (Fig. 2) during manipulation of the articulator.

Marking the occlusal contacts during manipulation of the articulator.
This simulates the most common clinical technique for examining occlusion and as an examination technique has been shown to have good inter- and intra-operator reliability.20
Once the occlusal contacts had been marked, the models were transferred to phantom heads in the clinical skills laboratory in order to simulate the examination of a supine patient. These models were not further articulated in the phantom heads and the original occlusal marks remained constant. Three operators independently examined these 20 occlusal schemes. As in a supine patient in a dental chair, the lower model was examined by direct vision and the upper by mirror. The schematic arches on the occlusal sketch were arranged in such a manner as to facilitate the record of the occlusal contacts from this perspective.
For the purpose of this trial the acetate sketch sheets were overlaid by a 1 mm2 grid. This enabled comparison between operators by comparing the X and Y co-ordinate for each occlusal contact on the sheet (Fig. 3).

This illustration for example represents among the others an occlusal contact on the mesio-lingual cusp of the lower right second molar with the co-ordinates X 46 : Y 16
Intra-operator reliability
One of the operators re-examined the same 20 sets of models on a further occasion at an interval of 3 months. The 'occlusal sketches' obtained at this examination were re-analysed in the same manner as previously.
Results
Inter-operator reliability
The 60 occlusal sketches generated by three examiners recording the occlusal marks on 20 sets of models were analysed by comparing the grid references of operator A versus B, B versus C, and A versus C. The results were analysed for Kappa agreement. The Kappa statistic reflects the degree of agreement among examiners, corrected for chance.
The coefficients of Kappa agreement allows for assessment of random agreement and the strength of agreement is displayed in Table 2. Kappa values for agreement between pairs of examiners were 0.90, 0.86, and 0.85 respectively, all indicating 'almost perfect' agreement (Table 3).
Intra-operator reliability
The range of Kappa agreement gave a median of 0.94 (almost perfect strength of agreement). This means that a high degree of agreement has been achieved when viewing an unchanged occlusal scheme at different times by the same operator.
Discussion
There is general agreement that the ability to examine and record occlusions accurately is essential in both research protocols and in clinical dentistry. It is surprising, therefore, that there does not appear to be any simple means of doing this with a proven level of inter- and intra-operator reliability. The problems raised in the introduction and the literature review are primarily related to poor study design, poor standardisation of technique and a lack of assessment of inter- and intra-operator reliability.
In the present study the median Kappa agreement readings showed strong correlation. This means that the methodology described permits different operators to reliably and consistently take occlusal records. The intra-operator reliability was also very strong with an even higher median. This means that the same operator can accurately record the same occlusion at different intervals in time with a very high degree of reproducibility.
This paper suggests that an 'occlusal sketch' is a system that is quick, easy, inexpensive and reliable in recording the results of an occlusal examination using articulating paper. It is hoped that it will have the following uses:
Clinically
A simple record of occlusion with a proven reliability could be of value in clinical dentistry as it offers the clinician and the dental laboratory technician a means of validating the accuracy of an occlusal registration during a restorative procedure.
In research
If it is suspected that occlusion may be an aetiological factor in dental disease or that certain procedures or conditions may cause a change in occlusion then further investigation is dependent upon an accurate means of recording the patient's occlusion at various times and by different operators in order that change may be quantified.
It may appear to be a limitation of this study that it was carried out using occlusal marks on models mounted in phantom heads (in vitro). However, in order to test whether occlusal sketching was reliably accurate, it was essential that the examinations were attempting to recording an unchanged occlusion. This is why the pseudo-clinical examination of a phantom head was used. It is our contention that an 'in vitro' application could only be tested by stimulating a clinical situation rather than using a patient where occlusion may vary. Dynamic occlusion was not tested because a small static occlusal mark is a greater challenge to record than a dynamic occlusal trace.
Conclusion
Three dentists when viewing the same occlusal contacts in a pseudo-clinical situation have made marks on a schematic representation of teeth in almost exactly the same places. This suggests that this simple means of recording an occlusion has a high degree of interoperator reliability. Similarly, a single dentist when examining the same occlusal marks in a pseudo-clinical situation at different times has recorded the same marks onto a schematic representation of the dental arches. These findings suggest a high degree of inter- and intra-operator reliability. Occlusal sketching offers the clinician a simple, inexpensive method of reliably recording and retaining a record of occlusal contacts.
Further research is at present being undertaken to confirm these parameters in clinical studies which use occlusal sketching as a means of determining whether occlusion changes during some dental procedures and to investigate the reliability of occlusal sketching as a means of communication between clinician and the dental technician.
References
Celenza FV, Nasedkin JN Occlusion. The state of the art. pp 31–41 Chicago: Quintessence Publishing Co. Inc 1978.
Gross MD, Mathews JD Occlusion in restorative dentistry. pp 36–50 Edinburgh: Churchill Livingstone 1982.
Pameijer JHN Periodontal and occlusion factors in crown and bridge procedures. pp 41–45 Amesterdam: PBC, Dental center for postgraduate courses 1985.
Dawson PE Evaluation diagnosis and treatment of occlusal problems. 2nd ed pp 436 Missouri: The C.V. Mosby Company 1989.
Millstein PL A permanent method of recording occlusal contacts. J Prosthet Dent 1985; 53: 748–749.
Fattore L-D, Malone WF, Sandrick JL et al. Clinical evaluation of the accuracy of interocclusal recording materials. J Prosthod Dent 1984; 51: 7.
Gazit E, Lieberman MA Occlusal contacts following orthodontic treatment. Measured by a Photocclusion technique. Angle Orthod 1985; 55: 316–320.
Ziebert GJ, Donegan SJ Tooth contacts and stability before and after occlusal adjustment. J Prosthet Dent 1979; 42: 276–281.
Ehrlich J, Taicher S Intercuspal contacts of the natural dentition in centric occlusion.. J Prosthet Dent 1981; 45: 419–421.
Millstein PL An evaluation of occlusal contact marking indicators: A Descriptive, Qualitative Method. Quintessence Int 1983; 8: 813–818.
Berry DC, Singh BP Daily variations in occlusal contacts. J Prosthet Dent 1983; 50: 286–391.
Berry DC, Singh BP Effect of electromyographic biofeedback therapy on occlusal contacts. J Prosthet Dent 1984; 51: 379–403.
Gazit E, Fitzig S, Lieberman MA Reproducibility of occlusal marking technique. J Prosthet Dent 1986; 55: 505–509.
Durbin DS, Sadowsky C Changes in tooth contacts following orthodontic treatment. Am J Orthod Dentofac Orthop 1986; 90: 375–382.
Razodolsky Y, Sadowsky C, BeGole EA Occlusal contacts following orthodontic treatment: a follow-up study. Angle Orthod 1989; 59: 181–186.
Haydar B, Ciõer S, Saatçi P Occlusal contact changes after the active phase of orthodontic treatment. Am J Orthod Dentofac Orthop 1992; 102: 22–28.
Maness WL, Benjamin M, Podoloff R, Bobic A, Golden RF Computerized occlusal analysis: a new technology. Quintessence Intl 1987; 18: 287–292.
Hsu M, Palla S, Gallo LM Sensitivity and reliability of the T-scan system for occlusal analysis. J Craniomandib Disord Facial Oral Pain 1992; 6: 17–23.
Davies SJ, Gray RJM, Smith PW Good occlusal practice in simple restorative dentistry. Br Dent J 2001; 191: 365–381.
Anderson G, Schulte JK, Aeppli DM Reliability of the evaluation of occlusal contacts in intercuspal position. J Prost Dent 1993; 70: 320–323.
Landis JR, Koch GC The measurement of observer agreement for categorical data. Biometrics 1977; 33: 159–74.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Davies, S., Gray, R., Al-Ani, M. et al. Inter- and intra-operator reliability of the recording of occlusal contacts using 'occlusal sketch' acetate technique. Br Dent J 193, 397–400 (2002). https://doi.org/10.1038/sj.bdj.4801575
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4801575
This article is cited by
-
Over-the-counter (OTC) bruxism splints available on the Internet
British Dental Journal (2014)
-
Risk management in clinical practice. Part 8. Temporomandibular disorders
British Dental Journal (2010)
-
Reproducibility and reliability of the occlusal sketch
British Dental Journal (2002)
