
Abstract
Design
Cluster-randomised controlled trial, in Belgian nursing homes.
Intervention
Supervised implementation of the ‘Oral health care Guideline for Older people in Long-term care Institutes’ (OGOLI) and the daily oral healthcare protocol derived from the guideline. This included appointing project supervisors and oral healthcare teams responsible for the implementation process, a three stage educational programme and oral healthcare records for each resident.
Outcome measure
The primary outcome variables were the knowledge and attitudes of nurses and nurses' aides towards oral health and oral hygiene. This was collected through a 15-item self-reported knowledge questionnaire and a four item attitude survey administered both at baseline and six months after the start of the study.
Results
Of the 651 participants who completed the initial survey 259 had complete data at six months. There were no significant differences between the control and intervention groups at baseline or follow up for baseline characteristics, knowledge or attitudes (p=0.42, p=0.37). At six months the intervention group showed higher knowledge scores (p<0.0001) but no difference in attitude scores (p=0.78).
Conclusions
Significant improvements in knowledge followed an educational programme where participants' initial knowledge was low and no improvement in knowledge was found in the intervention group. Educational activities alone had no impact on attitudes and further research on how to improve attitudes is required.
Similar content being viewed by others

Commentary
It is well documented that the population is ageing, and the number of those aged 75 and over in the UK are expected to double in the next 30 years.1 Modern medicine is allowing people to live to what can be called the ‘very old’ (80+),2 but often at the cost of living with disability or impairment. This frequently removes the possibility of living independently and necessitates habitation within a residential or nursing home environment, often relying on others for personal care procedures.
Existing studies have shown that oral health declines once resident in such an institution and as a result quality of life suffers.3,4,5,6,7 It is therefore no surprise that there has been global commitment to reduce such oral health inequality8 evidenced through intervention programmes aimed at this vulnerable subgroup.9,10,11
Interventions often focus on improving upon one or more of the perceived barriers to providing oral healthcare to care home users. Willumsen et al. divide these into three factors; firstly, those within the patients such as cognitive impairment, resistant behaviour and consent, secondly, carers' knowledge and attitudes, and finally the organisation of oral care in nursing homes.12
Awareness of the importance of carer knowledge is not novel. In 1988 Vigild suggested education on oral hygiene procedures should be given to carers who do not have sufficient knowledge,13 and within the UK in 2001 a trial assessed whether oral healthcare instruction for carers within nursing homes would result in improved oral health for the residents.14 Studies, including two systematic reviews,15,16 have generally shown that providing oral hygiene education to carers is effective in improving the oral hygiene of residents, presenting the evidence necessary on which to base guidelines for residential and nursing homes to follow.
This paper exhibits findings from the ABRIM (Actief Begeleide Richtlijn Implementatie Mondzorg) study in Belgium, conducted to assess the impact of recommendations from the guideline ‘Oral healthcare Guideline for Older people in Long-term care Institutions’ (OGOLI). Specifically it aimed to explore the impact of a supervised implementation of an oral healthcare protocol derived from the OGOLI guideline, in addition to education on nurses' and nurses' aides' oral health-related knowledge and attitude.
The design was a multi-centre cluster-randomised controlled trial, using the care home as the unit of randomisation, as randomising within a care home would have resulted in contamination of control staff by secondary learning from watching colleagues or talking to residents. Concealment of allocation was impossible as provision of ‘placebo’ knowledge is not conceivable.
A random sample of 12 nursing homes was achieved using computer aided tools to gain stratified (by geographical distribution) cluster sampling with replacement, to make up those that declined participation. The sampling could have also benefited from being stratified by size as well as location.
The study was approved by the Ethical Committee at Ghent University, and consent was gained from all the nursing homes prior to the study and from the nurses and nurses' aides individually. The intervention was applied to control homes following the study to fulfill ethical obligations.
A comprehensive explanation of the intervention is provided. Data were gathered before the educational sessions using a 34-item validated questionnaire and then six months after the start of the study with the same questionnaire. Fifteen questions looked at personal items, 15 looked at knowledge about oral pathology and oral hygiene but only four questions assessed attitude. However this section of the study was tested for reliability through a test-retest procedure in a comparable nursing home that was not participating in the study. Despite this, the authors conclude that the limited number may have led to poor discriminant validity.
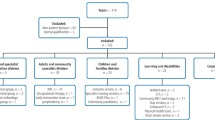
A flow diagram is provided, giving account of all nurses and nurses' aides that entered the trial, and the number of questionnaires filled out at each stage, with those completing the final ‘post’ questionnaire but not the original ‘pre’ questionnaire being removed through matching using a unique, anonymous code.
The full questionnaire is not provided but response options and scoring method are explained for each section.
As data were collected on personal items, the differences between control and intervention group were analysed at baseline and there was found to be none. Linear mixed-model analyses were also performed to assess differences in knowledge and attitude at six months owing to intervention and the predictive value or other explanatory factors. Intention to treat analysis was carried out; however it is not clear whether stratification was taken into account during analysis. It is also unclear whether the analysis was carried out blind, without which bias could be introduced due to the fact this is a secondary analysis of previously collected data.
At baseline 404 questionnaires were completed in the intervention group compared to 247 in the control group, creating an information bias. Following matching at six months 165 questionnaires from the intervention group could be compared against 94 from the control group. The high rate of loss and difficulty matching has been explained by the authors as that the participants were to remember the original, unique code, but many forgot so were noted as non-responders.
Unfortunately the results indicated that 52% of the participants in the intervention group did not participate in the educational part of the intervention. This clearly introduces difficulties in drawing firm conclusions based on the intervention, as knowledge may be improved from secondary sources, ie watching and talking to other staff who did attend the educational events and also those who attend the events are clearly motivated and already prioritise oral health.
However the primary variables were reported on, there was a statistically significant (p<0.0001) improvement between intervention group and control group for the variable knowledge at six months. The variable attitude however showed no significant difference (p=0.78) between control group and intervention group at six months. Unsurprisingly, as no differences were found at baseline, a significant difference (p<0.0001) was found comparing knowledge at baseline and at six months in the intervention group.
The control group also appeared to gain in knowledge and attitude although a p value is not provided. This is likely due to the provision of the questionnaire, which it itself may prompt knowledge-seeking behaviour.
Authors also found age and ward type had a significant impact on attitude and educational level a significant impact on knowledge at six months.
The main issue with this paper lies in the use of a questionnaire to measure outcomes. As a research instrument a questionnaire is imprecise and reflects subjective responses. Optional completion of the questionnaire also gives potential bias to those open to learning and with time (important as lack of time in care homes is often given as a reason for lack of oral hygiene procedures).12 The repeated use of the same questionnaire could also cause bias.
In conclusion this is a good study, using the most of data collected previously in an area that has a dearth of comparable studies. Particularly appreciated is the limitations section in which the authors detail the improvements they would like to achieve. As negative attitude of carers towards oral care has been reported previously as a barrier to providing oral hygiene procedures12 it is important to gain further information on this area. It is agreed that interventions to improve oral health in this group must be developed and this paper will aid that goal, relevant for all countries facing this demographic transition.
References
National Population Projections, 2012-based. Office for National Statistics. 2013.
Forman DE, Berman AD, McCabe CH, Baim DS, Wei JY . PTCA in the elderly: the “young-old” versus the “old-old”. J Am Geriatr Soc 1992; 40: 19–22.
Manderson RD, Ettinger RL . Dental status of the institutionalized elderly population of Edinburgh. Community Dent Oral Epidemiol 1975; 3: 100–107.
Wirz J, Brunner T, Egloff J . Dental care of the elderly. An inquiry on the status of dental welfare in the old age and nursing homes as well as in the geriatric medical clinics of Basel-Stadt and Basel-Land cantons. Schweiz Monatsschr Zahnmed 1989; 99: 1267–1272.
Weyant RJ, Jones JA, Hobbins M, Niessen LC, Adelson R, Rhyne RR . Oral health status of a long-term-care, veteran population. Community Dent Oral Epidemiol 1993; 21: 227–233.
Sweeney MP, Williams C, Kennedy C, Macpherson LM, Turner S, Bagg J . Oral health care and status of elderly care home residents in Glasgow. Community Dent Health 2007; 24: 37–42.
Johnson IG, Morgan MZ, Monaghan NP, Karki AJ . Does dental disease presence equate to treatment need among care home residents? J Dent 2014; 42: 929–237. doi:10.1016/j.jdent.2014.05.010.
WHO, 2010. World Health Organization Social and Gender inequalities in environment and health. http://www.euro.who.int/__data/assets/pdf_file/0010/76519/Parma_EH_Conf_pb1.pdf?ua=1
NHS Education for Scotland. Caring for Smiles. http://www.nes.scot.nhs.uk/education-and-training/by-discipline/dentistry/areas-of-education/oral-health-improvement-caring-for-smiles.aspx [Accessed 16 June 2015]
National Institute for Health and Care Excellence. Oral health: promoting and protecting oral health and ensuring access to dental treatment for adults in nursing and residential care homes.
NHS Fife. NHS Fife Home Care Awards. 12 Nov 2009. http://www.nhsfifehomecareawards.scot.nhs.uk/about.html.
Willumsen T, Karlsen L . Naess R Bjorntvedt . Are the barriers to good oral hygiene in nursing homes within the nurses or the patients? Gerondontology 2012. 29: e748–755
Vigild M . Oral hygiene and periodontal conditions among 201 dentate institutionalised elderly. Gerodontics 1988; 4: 140–145.
Frenkel HF, Harvey I, Newcombe RG . Improving oral health in institutionalised elderly people by educating care givers: a randomised controlled trial. Community Dent Oral Epidemiol 2001; 29: 289–297.
Weening-Verbree L, Huisman-de WG, van Dusseldorp L . Oral health care in older people in long term care facilities:a systematic review of implementation strategies. Int J Nurs Stud 2013; 50: 569–582.
de Lugt-Lustig KH, Vanobbergen JN, van de Putten GJ . Effect of oral healthcare education on knowledge, attitude and skills of care home nurses: a systematic literature review. Community Dent Oral Epidemiol 2014; 42: 88–96.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Barbara Janssens, UZ Ghent, P8, De Pintelaan 185, 9000 Ghent, Belgium. E-mail: barbarae.janssens@ugent.be
Janssens B, DeVisschere L, van der Putten GJ, de Lugt-Lustig K, Schols JM, Vanobbergen J. Effect of an oral healthcare protocol in nursing homes on care staffs' knowledge and attitude towards oral health care: a cluster-randomised controlled trial. Gerodontology 2014. doi: 10.1111/ger.12164 [Epub ahead of print]
Rights and permissions
About this article

Cite this article
Hollands, K., Burns, J. Oral healthcare protocols in a nursing home. Evid Based Dent 16, 93–94 (2015). https://doi.org/10.1038/sj.ebd.6401123
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401123
