
Abstract
Aim
To correlate the microaneurysmal closure rate measured on fundus fluorescein angiography (FFA) with reduction in macular thickness observed on optical coherence tomography (OCT) following laser photocoagulation of diabetic macular edema.
Materials and methods
A prospective observational case series. Fifty patients (50 eyes) of type II diabetes mellitus with clinically significant macular oedema (CSME) underwent focal/grid laser photocoagulation. OCT and FFA were performed at baseline and at 2 and 12 weeks following laser photocoagulation to measure the change in macular thickness and the number of leaking microaneurysms respectively. Statistical analysis was performed using paired-ttest and Pearson's correlation test.
Results
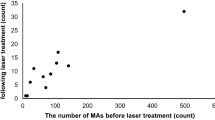
A significant reduction in macular thickness was seen at both 2 (P=0.02) and 12 weeks (P<0.0001), most remarkably in the central 1 mm quadrant. However, microaneurysm closure was only 0.67% at 2 weeks, which increased to 89.6% by 12 weeks. The change in retinal thickness correlated significantly with the decrease in the number of leaking microaneurysms at 12 weeks (r=0.597, P<0.0001), but not at 2 weeks (r=−0.228, P=0.112). On OCT, the final reduction in retinal thickness achieved at 12 weeks from baseline correlated significantly with the initial decrease in retinal thickness at 2 weeks (r=0.66, P<0.0001). However, on FFA, the final closure rate of leaking microaneurysms at 12 weeks from baseline did not correlate with the initial closure rate at 2 weeks (r=−0.039, P=0.413).
Conclusion
Following laser photocoagulation for CSME, an OCT at 2 weeks is more informative and better correlates with the final outcome than an FFA at 2 weeks.
Similar content being viewed by others

Introduction
The standard of care for treatment of clinically significant macular oedema (CSME) is focal laser photocoagulation.1 The response of CSME to laser treatment is characterized by closure of leaking microaneurysms, best visualized on fundus fluorescein angiogram (FFA),2 and reduction in macular thickness, best measured on optical coherence tomography (OCT).3 It seems obvious that as the microaneurysms close after the effect of laser photocoagulation, there will be cessation of leakage and hence a reduction in macular thickness will occur. However, correlation between the above two entities, that is the extent of microaneurysmal closure achieved and the resultant reduction in macular thickness, has not been studied before.
Materials and methods
This prospective study, approved by the ethics committee of our institute, included 50 patients (50 eyes) of type II diabetes mellitus having non-proliferative diabetic retinopathy with CSME in at least one eye. Baseline retinal thickness (mean of two readings) was measured in posterior central 6 mm of retina in nine predetermined quadrants using a fast macular thickness scan on STRATUS OCT. An angiogram was also performed and the dye transit phase picture was modified using the Adobe Photoshop software® and Coral graphics® to superimpose an OCT-like grid, created by assuming that the approximate distance between the major vascular arcades in the centre of posterior pole is around 6 mm. The grid was centred on the foveal centre and the number of leaking microaneurysms (those which became fuzzy in the late phase of angiogram) was counted.
Subsequently, the patients underwent standard focal or grid photocoagulation as described by ETDRS1using frequency-doubled Nd:YAG 532 nm laser. Repeat OCT and FFA were performed at 2 and 12 weeks following laser photocoagulation to measure the change in retinal thickness and the number of leaking microaneurysms with respect to the baseline. All microaneurysm counts were performed by two investigators separately, who were blinded to the patient protocol, and a mean of the two readings was taken. Statistical analysis was performed using paired-t test and Pearson's correlation test.
Results
OCT at 2 weeks, showed a significant reduction in retinal thickness in the central 1 mm quadrant (P=0.0004), whereas at 12 weeks the reduction was significant in all the nine quadrants (P<0.0001) (Table 1). However, the average retinal thickness in the posterior 6 mm retina showed a significant reduction at both 2 (P=0.02) and 12 weeks (P<0.0001). On FFA, the closure rate of pre-existing leaking microaneurysms at 2 weeks was only 0.67%. However, a majority of these microaneurysms (89.1%) were observed to close by 12 weeks (Table 1). The change in retinal thickness correlated significantly with the decrease in the number of leaking microaneurysms at 12 weeks (r=0.597, P<0.0001), but not at 2 weeks (r=−0.228, P=0.112).
On OCT, the final reduction in retinal thickness achieved at 12 weeks from baseline significantly correlated with the initial decrease in retinal thickness at 2 weeks (r=0.66, P<0.0001). This correlation was even better observed for the central 1 mm quadrant (r=0.72, P<0.0001) (Table 2). However, on FFA, the final closure rate of leaking microaneurysms at 12 weeks from baseline did not correlate with the initial closure rate at 2 weeks (r=0.039, P=0.413).
Discussion
We observed a significant reduction in retinal thickness at both 2 and 12 weeks following laser photocoagulation, whereas majority of microaneurysms were observed to close by 12 weeks only. How, can reduction in thickness be achieved without microaneurysm closure, remains the question. This probably could be explained by the fact, that after laser photocoagulation, individual microaneurysms may show some reduction in leakage at an earlier stage, a fact that may be very difficult to appreciate even on FFA, whereas their complete closure takes a longer time.2 This delayed closure of microaneurysms is possibly mediated by proliferation of new and functionally better pigmented epithelial cells and endothelial cells leading to a more efficient blood retinal barrier.2 Hence, expectedly, a significant correlation between the above two entities was seen only at 12 weeks and not at 2 weeks.
A significantly positive correlation between final reduction in retinal thickness on OCT at 12 weeks with initial improvement at 2 weeks, especially in the central 1 mm quadrant, suggest that the eyes which show a good initial response on OCT at 2 weeks continue to do better even at 12 weeks compared to those eyes with comparatively poorer initial response. However, similar interpretation could not be obtained from FFA. Hence we suggest that since an OCT at 2 weeks is more informative than FFA at 2 weeks, it should be regularly performed after laser photocoagulation.
References
Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Arch Ophthalmol 1985; 103: 1796–1806.
Gogi D, Gupta A, Gupta V, Pandav SS, Dogra MR . Retinal microaneurysmal closure following focal laser photocoagulation in diabetic macular edema. Ophthalmic Surg Lasers 2002; 33: 362–367.
Rivellese M, George A, Sulkes D, Reichel E, Puliafito C . Optical coherence tomography after laser photocoagulation for clinically significant macular edema. Ophthalmic Surg Lasers 2000; 31: 192–197.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary Information accompanies the paper on Eye website (http://www.nature.com/eye).
Supplementary information
Rights and permissions
About this article
Cite this article
Sachdev, N., Gupta, V., Abhiramamurthy, V. et al. Correlation between microaneurysm closure rate and reduction in macular thickness following laser photocoagulation of diabetic macular edema. Eye 22, 975–977 (2008). https://doi.org/10.1038/sj.eye.6702801
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702801
