
Abstract
Objective
To describe the post-operative complications reported in patients who had trabeculectomy with and without antimetabolite in UCH, Ibadan between 1999 and 2003 and the success rate achieved in term of the post-operative intraocular pressure (IOP).
Methods
A retrospective study of the records of glaucoma patients who had trabeculectomy between 1999 and 2003 and had follow-up in UCH Ibadan eye clinic for a minimum of 1 year was carried out.
Results
Seventy-six out of 171 eyes that had trabeculectomy during the period were reviewed. Mean age of patients was 49.4 years. The mean preoperative IOP was 31.8 mm Hg. Success rate of 79.4% was achieved in term of IOP control at a year of follow-up. The most frequent early post-operative complication was shallow AC (13 eyes; 17.1%) while late complication was elevated IOP (21 eyes; 27.6%). Others were encapsulated bleb 7.9% and hyphema 3.9%. There was no significant difference in the complication rate in those who had intraoperative antimetabolite (5-fluorouracil) when compared with those operated without antimetabolite.
Conclusion
Guarded filtration surgery is effective in controlling IOP. Most of the complications noted were transient and not visually threatening.
Similar content being viewed by others

Introduction
Trabeculectomy has remained the most effective weapon in the ophthalmologist's armoury with which we can achieve a satisfactorily low intraocular pressure (IOP).1 It continues to outperform both medical and laser treatment in this regard,2, 3 especially in Africans where availability of and compliance with topical therapy are limited.4 Also, trabeculectomy has been reported to be more beneficial in Africans in term of IOP lowering effect and slowing down of field loss.5, 6, 7
The goal of the surgery is to establish a permanent flow of aqueous from the anterior chamber to the subconjuctival space thereby lowering the IOP.
Since the description of the guarded filtering procedure by Cairn8 numerous modifications have been proposed.9, 10, 11 most of which are aimed at reducing the complications and improving the success in term of IOP lowering effect.
Studies have reported various types of complications following trabeculectomy with incidence differing from one study to another4, 12, 13, 14, 15, 16 depending on the duration of follow-up, the study population and the surgical techniques such as the use of antimetabolite and releasable sutures. Some of these complications are self-limiting while some adversely affect the overall success of the procedure.
Few data are currently available in this region on the post-operative complications and outcome of trabeculectomy.12, 13, 14
Aims and objective
To describe the post-operative complications reported among patients who had trabeculectomy in the University College Hospital Ibadan Eye Department between 1999 and 2003 and to evaluate the overall success in term of IOP control after a year of follow-up.
Materials and methods
A retrospective review of the case note of all patients who had trabeculectomy between January 1999 and December 2003 at UCH Ibadan, Nigeria was carried out.
Preoperative data retrieved included age, gender, type of glaucoma, preoperative antiglaucoma medication and their duration of usage and preoperative IOP. The preoperative IOP was taken as the value measured immediately prior to surgery. Intraoperative events recorded include the use of antimetabolite.
Post-operative complications as well as the time of their occurrences were recorded. Also the post-operative IOPs on first post-operative day, 1 week, a month, and at 1-year follow-up.
Hypotony was defined as IOP <5 mm Hg after fifth post-operative day.
A case was deemed to have failed if the IOP increased above 21 mm Hg during the post-operative examination. Early IOP rise was defined as IOP greater than 21 mm Hg before 4 weeks post-operative period.
Post-operative interventions such as reintroduction of antiglaucoma medication, reformation of anterior chamber, and repeat trabeculectomy were also recorded.
Patients included in this review were those who had post-operative follow-up for minimum of 12 months (range 12 months and 23 months). Both eyes of patients undergoing bilateral primary trabeculectomy were included except for the analysis of success rate in which only the first eye of patients who underwent bilateral surgery was used.
Excluded from the analysis were the eyes of patients under 30 years of age at the time of surgery, eyes that had repeat trabeculectomy, secondary glaucoma (traumatic, post-inflammatory, pseudoexfoliative), and patients whose record could not be retrieved.
Surgeries were performed by four senior surgeons. The use of antimetabolite was at the discretion of the surgeon.
Data analysis was performed using the SPSS statistical software.

Results
Seventy-six eyes of 44 patients were reviewed. Twenty-nine (65.9%) were males and 15 (34.1%) were females. The mean age of the patients was 49.4 years (median=47; SD=11.9). Seventy (92.1%) eyes had primary open angle glaucoma and six (7.9%) had chronic angle closure glaucoma (Table 1).
All the patients were on antiglaucoma medication preoperatively. The mean duration of medication was 2.4 years (range 1 month and 15 years; median=0.95; SD=3.9). Twenty-five (32.9%) eyes had intraoperative antimetabolite (5-fluorouracil (5-FU)) while 51 (67.1%) were operated without antimetabolite.
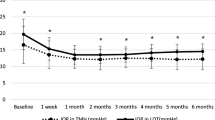
The mean preoperative IOP was 31.8 mm Hg (SD=11.2; median=32.0 and 95% CI, 27.2–36.5) for the 5-FU group and 32.3 mm Hg (SD=11.7; median=30.0 and 95% CI, 29.0–35.6) for the eyes without intraoperative antimetabolite.
The mean IOP for both groups on the first post-operative day was 8.4 mm Hg (95% CI, 6.9–9.9; median=6.0; SD=6.6). At 4 weeks post-operative period the mean IOP has increased to 16.4 mm Hg (95% CI, 14.6–18.2; median=14.5; SD=7.8). The mean reduction in IOP from the preoperative IOP was statistically significant (P⩽0.000). There was no significant difference in the mean IOP at the first post-operative day of the group that had intraoperative antimetabolite (8.2 mm Hg; 95% CI, 5.6–10.9; median=6.0; SD=6.4) and those that were operated without antimetabolite (8.5 mm Hg; 95% CI, 6.6–10.4; median=6.0; SD=6.7; Table 2).
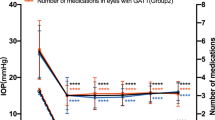
Using the Kaplan–Meier survival curve analysis (Figure 1) the probability of maintaining IOP of 21 mm Hg or less at 1 year of follow-up was 79.4%. (80.6% for the non-5-FU group and 76.7% for the 5-FU group.) Comparison of the curve by the log-rank test showed no significant difference between the two groups (P=0.136).

Kaplan–Meier survival curve.
Early post-operative complications recorded included shallow anterior chamber 13 (17.1%) eyes, IOP rise in 10 (13.2%) eyes, and hyphema 3 (3.9%) eyes. Late rise in IOP was recorded in 21 (27.6%) while bleb encapsulation occurred in 6 (7.9%) of the eyes with progression of cataract in 3 (3.9%) eyes. No case of endophthalmitis was recorded (Table 3).
Antiglaucoma medication was introduced in all the eyes with elevated IOP; however, effective IOP control was achieved in 17 eyes with 2 or more medications mainly β-blocker (Timoptol) and carbonic anhydrase inhibitor (Acetazolamide) and rarely prostaglandin analogue (Latanoprost) while 4 eyes had repeat surgery.
Discussion
Although aggressive antiglaucoma medical therapy has been found to be on par with trabeculectomy in the management of glaucomatous optic neuropathy for visual field preservation,2 the cost of long-term medication, compliance for medical therapy, and the need for regular ophthalmic reviews may hinder effective glaucoma management by medical therapy in a large proportion of patients.17
This study has again demonstrated the efficacy of trabeculectomy in reducing IOP. The mean reduction in IOP from 32.2 mm Hg (median=30.5; SD=11.4) in the preoperative period to 17.8 mm Hg (median=17.0; SD=5.8) at a year follow-up compares with report from other previous studies.4, 17, 18, 19
There was no significant difference between the 5-FU and the non-5-FU groups at a year follow-up in term of their mean IOP (P=0.6). The survival curve between the two groups also failed to demonstrate any added advantage to the use of antimetabolites. The difference was not statistically significant (log rank P=0.136; Breslow P=0.67). There has been conflicting report concerning the complications and long-term outcome of trabeculectomy in term of IOP control and the intraoperative use of antimetabolite (5-FU) Kabiru et al4 and Leyland et al20 found no added advantage in the use of antimetabolite. However, some other studies21, 22 reported a significant benefit with the use of intraoperative use of 5-FU. It may be difficult forming a conclusion based on this review as it is a retrospective study and patients were not randomized hence the problem of selection bias.
Most of these complications reported were transient and self-limiting. There was no significant difference in the complication rate between the group that had intraoperative 5-FU and those that did not, (Table 3) a finding similar to what was reported by Melke et al21 in their review in Southwestern Nigeria. These early complications included shallow anterior chamber, hyphema, hypotony, and hypopyon. Most of the patients with shallow anterior chamber were managed by adequate dilatation and overnight padding. There were two eyes that required surgical intervention in form of reforming the anterior chamber. Three eyes that had leaking bleb with positive Seidel 1 test did well on padding. Shallow anterior chamber ranked highest in the list of early post-operative complications and is similar to what had being reported in some other previous studies.4, 12, 15, 20, 21 There was no clinically documented case of choroidal effusion/detachment, the incidence of which is very low among blacks compared to Caucasians. This study showed no significant correlation between the use of 5-FU and the presence of post-operative shallow anterior chamber. (P=0.75 Fisher's exact test; OR 0.8; 95% CI, 0.4–1.8). The Cochrane review reported no consistently increased risk of shallow anterior chamber in those who received 5-FU.23
There were much fewer cases of hyphema in this review than reported in some other study in Nigeria21 and among Caucasians.15, 16 This may be related to the generous but cautious cauterization of the scleral bed at surgery, a technique well favoured by most of the surgeons in the centre. The higher incidence reported among the white subjects in the CIGTS was partly attributed to the fact that perhaps blood was more visible in the eye of whites, and hence a greater reporting.15 There was no case of endophthalmitis in any of the patients at their last follow-up. The very marginal infective complication reported in this series could be factored to such preoperative measures as ensuring no growth on conjuctival culture with sterilization of the conjuctival fornices using 5% povidone iodine, paying detailed attention to aseptic technique intraoperatively and post-operative use of antibiotics. Furthermore, the incidence of endophthalmitis following trabeculectomy ranged between 0.2 and 1.5% for those without antimetabolites24, 25 and 3.0% in those with 5-FU.26
Six (7.6%) eyes were complicated by encapsulated bleb compared to the one eye reported by Baiyeroju and Ubah.12 The overall incidence is less than encapsulated bleb was reported in some other studies (AGIS 14%;3 CIGTS 12%).15 The low incidence of encapsulated bleb reported may be due to reporting a problem common with retrospective studies as some studies has reported that increased keloid activity in Africans predispose them to increased scarring with resultant bleb encapsulation and resultant bleb failure.27
The success achieved was 79.4% at a year follow-up which compares with findings in some other previous studies in Western Nigeria.13, 21 It may be difficult making a meaningful comparison of these findings with what has been reported in some other studies elsewhere because of the difference in the population group, the follow-up period and the criteria used in defining success. In this review, post-operative IOP 21 mm Hg or less without any medication or with only one medication was regarded a success thus putting together what some studies categorized as qualified success and complete success.
The review showed no strong association between prolonged uses of antiglaucoma medication and surgical failure (P=0.17; OR 1.2; 95% CI, 0.9–1.6). The untoward effect of prolonged antiglaucoma medication on the outcome of filtration surgery has been well documented. Various reasons have been adduced for this. Lavin et al28 found that filtering surgery was more successful in patients who had received an average of only 2 weeks of preoperative medical treatment than in patients who had received at least 1 year of antiglaucoma treatment. Broadway et al29 reported that long-term topical medication caused a decrease in goblet cell density but an increase in fibroblasts, macrophages, and mast cells in the substantia propria and an increase in macrophages and lymphocytes in the epithelium. They also demonstrated that these changes were more significant if more than one drug was administered. The lack of association in this review could be a factor of poor drug compliance, a fairly common problem among glaucoma patients in Africa.
Hypotony complicating trabeculectomy has low incidence among black, hence is not a surprise that no cases of hypotony was recorded. Singh et al30 in a study of 5-FU augmented trabeculectomy in a West African population found no case of hypotony or choroidal detachment. It has been suggested that this could be a factor of the thickness of the sclera.31
Conclusion
Guarded filtration surgery is effective in controlling IOP. Most of the complications noted were transient and not visually threatening. The intraoperative use of antimetabolite did not increase the incidence of post-operative complications.
References
Husain R, Clarke JCK, Seah SLK, Khaw PT . A review of trabeculectomy in East Asian people—the influence of race. Eye 2005; 19: 243–252.
Lichter PR, Musch DC, Gillespie BW, Guirre KE, Janz NK, Wiren PA et al. Interim clinical outcomes in the collaborative initial glaucoma treatment study comparing initial treatment randomized to medication or surgery. Ophthalmology 2001; 108: 1943–1953.
AGIS Investigators . The Advanced Glaucoma Intervention Study (AGIS): 9. Comparison of glaucoma outcomes in black and white patients within treatment group. Am J Ophthalmol 2001; 132: 311–320.
Kabiru J, Bowman R, Wood M, Mafwiri M . Audit of trabeculectomy at a tertiary referral hospital in East Africa. J Glaucoma 2005; 14: 432–434.
David R, Freedman J, Luntz MH . Comparative study of Watsons and Cairns trabeculectomies in a black population with open angle glaucoma. Br J Ophthalmol 1977; 61: 117–119.
Sandford-Smith JH . The surgical treatment of open-angle glaucoma in Nigerians. Br J Ophthalmol 1978; 62: 283–286.
Thommy CP, Bhar IS . Trabeculectomy in Nigerian patients with open-angle glaucoma. Br J Ophthalmol 1979; 63: 636–642.
Cairns JE . Trabeculectomy: preliminary report of a new technique. Am J Ophthalmol 1968; 66: 673–679.
Five year follow up of the fluorouracil filtering surgery study. The fluorouracil filtering surgery study group. Am J Ophthalmol 1996; 121: 349–366.
Ophir A, Ticho U . A randomized study of trabeculectomy and subconjuctival administration of fluorouracil in primary glaucomas. Arch Ophthalmol 1992; 110: 1072–1075.
Bell RW, Habib NE, O'Brien C . Long term result and complications after Trabeculectomy with a single perioperative application of 5-fluorouracil. Eye 1997; 11 (Part 5): 663–671.
Baiyeroju AM, Ubah JN . A review of the effect of 5-fluorouracil on the outcome of Trabeculectomy in Ibadan. Niger J Ophthalmol 2004; 12 (1): 14–18.
Bekibele CO . Evaluation of 56 trabeculectomy operations at ago Iwoye, Ogun State, Nigeria. West Afr J Med 2001; 20 (3): 223.
Anand N, Melke C, Dawda VK . Trabeculectomy outcomes in advanced glaucoma in Nigeria. Eye 2001; 15: 274–278.
Jampel HD, Musch DC, Gillespie PW, Lichter PR, Wright MM, Guire KE et al. Perioperative complications of trabeculectomy in the collaborative initial glaucoma treatment study (CIGTS). Am J Ophthalmol 2005; 140: 16–22.
Edmunds B, Thompson JR, Salmon JF, Wormold RP . The National Survey of Trabeculectomy 111. Early and late complications. Eye 2002; 16: 297–3003.
Sihota R, Grupta V, Agarwal HC . Long term evaluation of trabeculectomy in primary open angle glaucoma and chronic primary angle closure in an Asian population. Clin Exp Ophthalmol 2004; 32: 23–28.
Quigley HA, Buhrmann RR, West SK, Isseme I, Scudder M, Oliva MS . Long term result of glaucoma surgery among participants in an east African population survey. Br J Ophthalmol 2000; 84: 860–864.
Ehrnrooth P, Lehto I, Puska P, Laatikainen L . Long term outcome of trabeculectomy in term of intraocular pressure. Acta Ophthalmol Scand 2002; 80: 267–271.
Leyland M, Bloom P, Zinicola E, McAlister J, Rassam S, Migdal C . Single intraoperative application of 5-fluorouracil vs placebo in low risk Trabeculectomy surgery. A randomized trial. J Glaucoma 2001; 10: 452–457.
Melke C, Dawda VK, Anand N . Intraoperative 5-fluorouracil application during primary trabeculectomy in Nigeria: a comparative study. Eye 2003; 17: 829–834.
Egbert PR, William AS, Singh K . A prospective trial of intraoperative fluorouracil during trabeculectomy in a black population. Am J Ophthalmol 1993; 116: 612–616.
Wormald R, Wilkins WR, Bunce C . Postoperative 5-fluorouracil for glaucoma surgery (review). The Cochrane Library 2006, issue 3.
Azuara-Blanco A, Katz LJ . Dysfunctional filtering bleb. Surv Ophthalmol 1998; 43: 93–126.
Ayyala RS, Bellows AR, Thomas JV, Hutchnson BT . Bleb infections: clinically different courses of ‘blebitis’ and endophalmitis. Opthalmic Surg Lasers 1997; 28: 452–460.
Wolmer B, Liebmann JM, Sassani JW, Ritch R, Speaker M, Marmor M . Late bleb—related endophthalmitis after trabeculectomy with adjunctive 5-fluorouracil. Ophthalmology 1991; 98: 1053–1060.
Merritt JC . Filtering procedures in American Blacks. Ophthalmic Surg 1980; 11: 91–94.
Lavin MJ, Wormald RP, Migdal CS, Hitchings RA . The influence of prior therapy on the success of trabeculectomy. Arch Ophthalmol 1990; 108: 1543–1548.
Broadway DC, Grierson I, O'Brien C, Hitchings RA . Adverse effect of antiglaucoma medication: 11. The outcome of filteration surgery. Arch Ophthalmol 1994; 12: 1446–1454.
Singh K, Byrd S, Egbert PR, Budenz D . Risk of hypotony after primary trabeculectomy with antifibrotic agents in a black African population. J Glaucoma 1998; 7: 82–85.
Stamper RL, Mc Menemy MG, Lieberman MF . Hypotonous maculopathy after trabeculectomy with subconjuctival 5-fluorouracil. Am J Ophthalmol 1992; 114: 544–553.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ashaye, A., Komolafe, O. Post-operative complication of trabeculectomy in Ibadan, Nigeria: outcome of 1-year follow-up. Eye 23, 448–452 (2009). https://doi.org/10.1038/sj.eye.6702979
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702979
Keywords
This article is cited by
-
Phaco-goniosynechialysis versus phaco-trabeculectomy in patients with refractory primary angle-closure glaucoma: a comparative study
BMC Ophthalmology (2023)
-
Randomized Clinical Trial for Early Postoperative Complications of Ex-PRESS Implantation versus Trabeculectomy: Complications Postoperatively of Ex-PRESS versus Trabeculectomy Study (CPETS)
Scientific Reports (2016)
-
Evaluation of recurrent hyphema after trabeculectomy with ultrabiomicroscopy 50-80 MHz: a case report
BMC Research Notes (2012)
