
Abstract
Aims:
To study the efficacy of verteporfin photodynamic therapy (VPDT) retrospectively in the treatment of idiopathic subfoveal choroidal neovascularization (ICNV) in an Asian population in correlation with number of treatments and age at treatment. This is the first report to compare the efficacy between single and multiple treatments.
Methods:
VPDT was administered according to protocol to 45 eyes in 45 patients aged 18–55 years diagnosed with active subfoveal ICNV between September 2003 and December 2005. In total 28 patients received a single VPDT treatment and the remaining 17 received multiple treatments. Collected measurements of visual acuity (VA) were plotted on a time-course model, and later dichotomized by age (18–45 vs46–55 years).
Results:
The 28 patients receiving a single VPDT treatment showed significant improvement in VA at 3-month follow-up. The 17 patients, who did not show improvement after the first treatment, received multiple VPDT treatments. Those patients showed an even clearer trend in VA improvement although significance was detected only at the 24th month. All patients showed a significant improvement in mean VA of 0.46 logMAR (P<0.01 compared to baseline) by the end of the 24-month observation period, although VPDT treatment for subfoveal ICNV appears to stabilize vision more rapidly in younger patients.
Conclusions:
ICNV patients who did not benefit from single VPDT treatments could receive multiple treatments, and showed a more significant improvement in visual acuity. These results are the first of their kind in ICNV treatment.
Similar content being viewed by others


Introduction
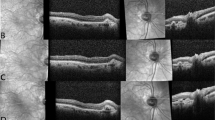
Choroidal neovascularization (CNV) is a significant cause of blindness in patients in developed countries. In patients younger than 55 years of age, CNV is commonly secondary to diseases and disorders such as ocular histoplasmosis syndrome (OHS), pathologic myopia, traumatic rupture of the choroid, Bruch membrane, or retinal pigment epithelium (RPE), or angioid streaks. However, a small subset of younger or middle-aged adults develops CNV in the absence of pathologic myopia, inflammatory disease, degeneration of the Bruch membrane, or post-traumatic findings. These patients are classified as having idiopathic CNV (ICNV). ICNV is essentially a diagnosis of exclusion. The diagnostic criteria are age at presentation <55 years and absence of other diseases or conditions associated with CNV. Fukuchi et al1 have classified ICNV according to three stages—active, intermediate, and cicatricial—on the basis of the patient's history, findings on fundal examination, extent of leakage in fluorescein angiography, and images obtained by optical coherence tomography. ICNV has been estimated to represent about 17% of cases of CNV in patients <50 years, with 67% of cases occurring in women.2
Patients with subfoveal ICNV are considered to have a more favourable long-term prognosis than patients with subfoveal CNV secondary either to OHS or AMD.3 Patients with subfoveal ICNV are also less likely to have profound visual loss, but with significant variation between individuals, the natural course of subfoveal ICNV is difficult to predict.4 Information on subfoveal ICNV is limited by the relatively small number of patients who fall into this subgroup. The present study reports on the results of single vs multiple VPDT treatments in adult patients with subfoveal ICNV.
VPDT is regarded as a safe and minimally invasive form of treatment for macular disorders in general.5 It is used to treat subfoveal CNV associated with pathologic myopia and CNV secondary to AMD as well as subfoveal ICNV. VPDT is preferable to thermal laser photocoagulation for treating subfoveal ICNV, as the latter damages overlying retinal photoreceptors and risks causing immediate loss of central vision.6 The verteporfin roundtable participants published updated guidelines in 2005 recommending VPDT for patients diagnosed with subfoveal ICNV or CNV located so close to the foveal centre that conventional laser photocoagulation treatment would extend beneath the centre.7 Several case series reports of VPDT in patients with subfoveal ICNV have found it a safe treatment option preferable to either observation or submacular surgery.3, 8, 9, 10, 11
Photodynamic therapy is a two-stage treatment designed to occlude the abnormal blood vessels found in CNV while sparing overlying retinal tissue. Verteporfin (Visudyne), a photosensitizing agent, is administered intravenously and activated 15 min later by application of non-thermal red or near-infrared light at a wavelength of 689 nm. Activation of verteporfin results in the formation of singlet oxygen, hydroxyl radicals, and peroxides, leading to occlusion of the blood vessels through thrombus formation, platelet adhesion, and damage to epithelial cells. VPDT is repeated every 3 months as long as leakage appears on fluorescein angiography (FA).
Although several case series of VPDT treatment of patients with subfoveal ICNV have been reported in the literature, and some authors report different prognoses for patients in different age groups,11 none to our knowledge, have reported differences in outcome between single and multiple VPDT treatments or compared results of verteporfin treatment by age.
Materials and methods
Subjects
Patients 18–55 years old attending the ophthalmology clinics of Cathay General Hospital in Hsih-Chu City and Taipei, Taiwan, during the period from September 2003 to December 2005 were included for the study. Inclusion criteria were (1) symptoms of visual disturbance within 6 months of the clinical visit; (2) diagnosis by FA of active subfoveal ICNV without refractive error >−6.00 D (myopia+½ D of astigmatism) by a senior staff ophthalmologist; and (3) a best-corrected visual acuity (BCVA) of at least 20/400. Exclusion criteria were (1) clinical features suggesting that CNV was secondary to pathologic myopia or other conditions; (2) presence of systemic disease, including diabetes mellitus and hypertension; (3) previous diagnosis of ophthalmic disease (glaucoma, diplopia, cataract, retinal detachment, concurrent ocular or macular diseases, and ocular trauma); and (4) contraindications to the use of verteporfin or other angiographic dyes, including indocyanine green. Informed consent was obtained from each patient before treatment.
Intervention
Eligible patients were treated with VPDT using verteporfin (Visudyne; Novartis AG, Bulach, Switzerland) according to the protocol established by the verteporfin photodynamic therapy (VPDT) study group.12 A dose of 6 mg/m2 of body surface area was infused intravenously over a 10-min period followed by a 5-min pause. At 15 min after initiation of infusion, the drug was activated by a 689-nm laser light (Coherent Opal Photoactivator; Lumenis, Santa Clara, CA, USA). Light was delivered to the lesions at an intensity of 600 mW/cm2 over 83 s.2 The spot laser diameter was determined by measurements obtained by digital angiography (Imagenet, Paramus, NJ, USA) and the addition of 1000 μm to the greatest linear dimension (GLD) of the lesion.
The VA of each patient was routinely measured at intervals of 1, 3, 6, 12, 15, 18, and 24 months after the initial treatment by a technician uninvolved in therapy, using the standard Snellen E-chart. Fluorescein angiograms were taken at follow-up visits. Retreatment was considered if fluorescein leakage was noted during the follow-up but was discontinued in the absence of leakage.
Statistical analysis
To adhere to the assumption of independence for each outcome, only data from the eyes with the worse baseline VA for patients with bilateral subfoveal ICNV were used in statistical analysis, for a conservative assessment of the effects of VPDT. A paired t-test comparison of measurements from each follow-up visit and analyses stratified by single or multiple treatments were then conducted. The time course of VA measurements was plotted according to a model that accounted for single vs multiple treatments. Later, another model was constructed based on age (18–45 vs 46–55 years). For both models, a P-value less than 0.05 was considered statistically significant. Statistical analyses were performed by SPSS 13.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
Forty-five eligible patients were included in the study, 25 men and 20 women. Their mean baseline visual acuity (VA) was poor, at 0.80 logarithm of the minimum angle of resolution (logMAR). Although subfoveal ICNV is predominantly a unilateral disorder,11 four of our patients were diagnosed with bilateral subfoveal ICNV. Data were collected only for the weaker eye in these patients. The patients ranged in age from 18 to 55 years, with a mean of 43.42 years (SD=9.55) and a median of 46 years. Since this was a retrospective study, we did not randomize the patients into two groups. The patients received the first treatment at beginning. Among them, 28 patients showed significant improvement in VA at 3-month follow-up. The rest of the 17 patients, who did not show any improvement after the first treatment, received 2–4 VPDT treatments, with an average of 2.29 treatments. Table 1 shows the baseline characteristics and clinical features of subjects who received single and multiple treatments for subfoveal ICNV.
Only consecutive treatments within intervals shorter than 6 months were considered in follow-up analyses. Figure 1 shows that patients treated with VPDT indicated significant improvement in VA of 0.25 logMAR by paired t-tests compared to baseline VA on the logMAR scale (P<0.05) at the 2-month follow-up. Over the next 22 months of period, patients' BCVA changed to 0.47, 0.48, 0.48, 0.39, and 0.34 logMAR in the following 6th, 12th, 15th, 18th, and 24th month (P<0.01 compared to baseline) (Figure 1).

Visual acuity improvement after VPDT (n=45), values are represented as mean±SE. *Paired t-tests compared to baseline visual acuity on logMAR scale, P<0.05. **Paired t-tests compared to baseline visual acuity on logMAR scale, P<0.01.
Figure 2a and b represent analyses stratified according to number of VPDT treatments. Figure 2a documents the improvement in VA for the 28 patients with subfoveal ICNV who received only a single VPDT treatment. These patients showed significant improvement in VA after the 3-month follow-up through the end of the 2-year observation period. Figure 2b identifies an even clearer trend in VA improvement for the 17 patients who received multiple VPDT treatments, although significance was detected only at the 24th month because of limited sample size.

(a) Visual acuity improvement after single VPDT treatment (n=28), values are represented as mean±SE. *Paired t-tests compared to baseline visual acuity on logMAR scale, P<0.05. **Paired t-tests compared to baseline visual acuity on logMAR scale, P<0.01. (b) Visual acuity improvement after first VPDT treatment in patients receiving multiple treatments (n=17), values are represented as mean±SE. *Paired t-tests compared to baseline visual acuity on logMAR scale, P<0.05.
Regardless of the number of treatments, data were analysed retrospectively according to patients' age with the cutoff point being the median age of 46 years. Results are shown in Figure 3. We found that the time course of VA measurements plotted according to age exhibited no statistical difference in baseline VA. The mean logMAR at baseline was 0.77 for younger and 0.82 for older patients. The P-value of the independent t-test was 0.82. The lack of a statistically significant difference between the two age groups persisted until the end of the observation period. The dramatic increase in logMAR in the older group after 6 months may have resulted from a diminished sample size. At the end of the observation period, the mean logMAR was 0.22 for the younger group and 0.44 for the older (Figure 3). The younger adults exhibited statistically significantly greater improvement in follow-up visits: 0.51, 0.44, 0.41, 0.32, 0.31, 0.22, and 0.22. These findings point to more rapid effects of treatment in younger adults (P<0.05).

Visual acuity improvement by age group after first photodynamic therapy, values are represented as mean±SE. No significant difference was detected by independent t-tests between age groups on each follow-up visit for visual acuity on logMAR scale. *Paired t-tests compared to baseline visual acuity on logMAR scale, P<0.05. **Paired t-tests compared to baseline visual acuity on logMAR scale, P<0.01.
Discussion
Verteporfin photodynamic therapy treatment results in short-term restoration of VA in patients with subfoveal ICNV younger than 50 years of age.9, 11, 13 Ruiz-Moreno et al9 found that the mean BCVA in 16 patients with sub- and juxta-foveal ICNV changed from 0.63 logMAR before treatment to 0.82 logMAR after VPDT treatment Lam et al13 reported that eight eyes with subfoveal ICNV changed from a mean VA of 20/200 before VPDT to a mean of 20/125 after treatment. A review of the use of verteporfin in photodynamic therapy recommends it as first-line treatment in patients with subfoveal CNV lesions, whether idiopathic or secondary to AMD.14 Chan et al15 reported a case series of 17 Chinese patients with subfoveal ICNV in which 94% of the subjects had stable or improved VA at 12-month follow-up, a rate comparable to those reported in Caucasian subjects. Our findings support the efficacy of VPDT in treating subfoveal ICNV in Asian eyes, which may differ from those of other races (especially in western populations), although our subject group did not have the female predominance noted in other studies.
Concerning stratification by single vs multiple treatments, the 28 patients who received a single VPDT treatment showed significant improvement in VA from the 3-month follow-up through the end of the 24-month observation period. The other 17 patients who received multiple treatments also showed a significant improvement in VA from 0.74 at baseline to 0.18 at 24 months after treatment. This outcome is comparable to the findings of Maár et al16 regarding the treatment frequency and VA in patients with subfoveal CNV secondary to pathologic myopia. In contrast, in a previous study, we found that VPDT treatment for CNV in patients with pathological myopia receiving single treatments had significantly improved VA over a 2-year period. Improvement was not as distinctive for patients receiving multiple treatments.17
While incidence and gender ratio of subfoveal ICNV are thought to vary somewhat across racial and ethnic groups,18 further study is warranted by certain newer treatment modalities that make PDT newly relevant. Most practitioners of VPDT prefer a combination therapy, such as PDT+anti-vascular endothelial growth factor (anti-VEGF), IVI.19 First, practitioners apply PDT treatment, and then follow patients to ensure a good follow-up. Should further treatment be warranted, they will try one of the two methods. First, they may try multiple PDT treatments. Result of the present study suggests that this may produce acceptable results. Or they may shift to another therapy (eg, single treatment+other therapy). This may be more feasible for older patients.
There is some disagreement in the literature whether age is a significant factor in visual outcome in general. Ergun et al20 reported that younger age is a significant prognostic factor of a better outcome in patients with pathologic myopia treated with VPDT, a finding corroborated by Axer-Siegel et al.21 Ho et al22 had earlier stated, however, that age is not predictive of either final VA or a significant change in vision in patients with subfoveal ICNV. Our study suggests that younger adults with subfoveal ICNV respond more rapidly to VPDT, while older patients demonstrate longer lasting effects of treatment. The group of younger patients in our study experienced an early and noticeable change in VA from a mean logMAR of 0.46 at 1-month follow-up to a mean logMAR of 0.31 at 3-month follow-up. This trend indicates a more rapid effect of treatment in younger patients, similar to that observed by Rogers et al23 in their case series of 19 eyes with subfoveal idiopathic and inflammatory CNV.
This study was limited by its relatively small sample size and data collection retrospectively. Also, 24-months follow-up may not be enough to see the long-term effect of the treatment. In addition, measurements of maximum and minimum retinal thickness over the course of VPDT treatment were not recorded. Significantly, though, the present report included more ICNV patients than any previous single study. In addition, this is the first report in the literature to compare the efficacy of single vs multiple ICNV treatment. VPDT treatment for subfoveal ICNV appears to improve the VA in both single and multiple treatments group. We also found that, while both young and older adults benefited from the treatment, VA stabilized more rapidly in younger adults.
References
Fukuchi T, Takahashi K, Ida H, Sho K, Matsumura M . Staging of idiopathic choroidal neovascularization by optical coherence tomography. Graefes Arch Clin Exp Ophthalmol 2001; 239: 424–429.
Cohen SY, Laroche A, Leguen Y, Soubrane G, Coscas GJ . Etiology of choroidal neovascularization in young patients. Ophthalmology 1996; 103: 1241–1244.
Giansanti F, Virgili G, Varano M, Tedeschi M, Rapizzi E, Giacomelli G et al. Photodynamic therapy for choroidal neovascularization in pediatric patients. Retina 2005; 25: 590–596.
Chan WM, Lam DS, Wong TH, Lai TY, Kwok AK, Tam BS et al. Photodynamic therapy with verteporfin for subfoveal idiopathic choroidal neovascularization: one-year results from a prospective case series. Ophthalmology 2003; 110: 2395–2402.
Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin. Arch Ophthalmol 1999; 117: 1329–1345.
Macular Photocoagulation Study Group. Laser photocoagulation of subfoveal neovascular lesions of age-related macular degeneration. Updated findings from two clinical trials. Arch Ophthalmol 1993; 111: 1200–1209.
Verteporfin Roundtable Participants. Guidelines for using verteporfin (Visudyne) in photodynamic therapy for choroidal neovascularization due to age-related macular degeneration and other causes: update. Retina 2005; 25: 119–134.
Stone TW, Sternberg Jr P . Submacular surgery trials update. Ophthalmol Clin North Am 2002; 15: 479–488.
Ruiz-Moreno JM, Montero JA, Arias L, Sanabria MR, Coco R, Silva R et al. Photodynamic therapy in subfoveal and juxtafoveal idiopathic and postinflammatory choroidal neovascularization. Acta Ophthalmol Scand 2006; 84: 743–748.
Kumar A, Prakas G, Singh RP . Transpupillary thermotherapy for idiopathic subfoveal choroidal neovascularization. Acta Ophthalmol Scand 2004; 82: 205–208.
Yoo MH, Boo HD, Kim HK . Result of photodynamic therapy for idiopathic subfoveal choroidal neovascularization. Korean J Ophthalmol 2005; 19: 264–268.
TAP Study Group. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: 2-year results of 2 randomized clinical trials—TAP report 2. Arch Ophthalmol 2001; 119: 198–207.
Lam A, Lee HC, Ho AC, Regillo CD, McNamara JA, Fineman MD . Photodynamic therapy in young patients. Ophthalmic Surg Lasers Imaging 2006; 37: 182–189.
Fenton C, Perry CM . Verteporfin: a review of its use in the management of subfoveal choroidal neovascularisation. Drugs Aging 2006; 23: 421–445.
Chan WM, Lai TY, Tano Y, Liu DT, Li KK, Lam DS . Photodynamic therapy of macular diseases of Asian populations: when East meets West. Jpn J Ophthalmol 2006; 50: 161–169.
Maár N, Ergun E, Luksch A, Stur M . Treatment frequency and visual outcome in subfoveal choroidal neovascularization related to pathologic myopia treated with photodynamic therapy. Graefes Arch Clin Exp Ophthalmol 2006; 244: 1262–1266.
Chen YS, Lin JY, Tseng SY, Yow SG, Hsu WJ, Tsai SC . Photodynamic therapy for Taiwanese patients with pathologic myopia: a 2-year follow-up. Retina 2007; 27 (7): 839–845.
Capone Jr A, Wallace RT, Meredith TA . Symptomatic choroidal neovascularization in blacks. Arch Ophthalmol 1994; 112: 1091–1097.
Eyetech Study Group. Anti-vascular endothelial growth factor therapy for subfoveal choroidal neovascularization secondary to age-related macular degeneration: phase II study results. Ophthalmology 2003; 110 (5): 979–986.
Ergun E, Heinzl H, Stur M . Prognostic factors influencing visual outcome of photodynamic therapy for subfoveal choroidal neovascularization in pathologic myopia. Am J Ophthalmol 2004; 138: 434–438.
Axer-Siegel R, Ehrlich R, Weinberger D, Rosenblatt I, Shani L, Yassur Y et al. Photodynamic therapy of subfoveal choroidal neovascularization in high myopia in a clinical setting: visual outcome in relation to age at treatment. Am J Ophthalmol 2004; 138: 602–607.
Ho AC, Yannuzzi LA, Pisicano K, DeRosa J . The natural history of idiopathic subfoveal choroidal neovascularization. Ophthalmology 1995; 102: 782–789.
Rogers AH, Duker JS, Nichols N, Baker BJ . Photodynamic therapy of idiopathic and inflammatory choroidal neovascularization in young adults. Ophthalmology 2003; 110: 1315–1320.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chen, YS., Lin, JS., Tseng, SY. et al. Photodynamic therapy of idiopathic subfoveal choroidal neovascularization in Taiwanese patients: a 2-year follow-up. Eye 23, 314–319 (2009). https://doi.org/10.1038/sj.eye.6703073
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6703073
