
Abstract
Particulate air pollution has been related with cardiopulmonary morbidity and mortality. Recent studies have shown that an increase in particulate matter (PM)2.5 ambient concentrations was associated with a decrease in heart rate variability (HRV) in the elderly with cardiovascular conditions, which could increase the risk of death. In order to assess if this association could also be observed in young adults, we studied 40 young healthy residents of the Mexico City Metropolitan Area (MCMA) who underwent 13 h Holter electrocardiographic and PM2.5 personal monitoring. HRV was evaluated in time domain: the standard deviation of normal RR intervals (SDNN) and the percentage of differences between adjacent normal RR intervals larger than 50 ms (pNN50). In multivariate analysis with mixed effects models, a significant negative association of pNN50 with PM2.5 accumulative exposure was found. An increase in 30 μg/m3 of the average PM2.5 personal exposure in the previous 2 h decreased the pNN50 in 0.08% (P=0.01). This observation revealed an acute effect related to environmental exposure to PM2.5 with regard to HRV in normal youngsters. The long-term health consequences of this association in young healthy adults remain to be clarified.
Similar content being viewed by others

Introduction
Air pollution is a major public health problem, which has been associated with an increase in cardiopulmonary morbidity and mortality in many cities around the world after short-term exposures (Dockery and Pope, 1994; Katsouyanni et al., 1995; Wong et al., 2001). Acute as well as chronic exposure to suspended particulate matter (PM) has been linked to a rise in hospital admissions (Zanobetti et al., 2000) and emergency room visits due to respiratory and cardiovascular causes, especially in children under 5 years of age with asthma (Schwartz et al., 1994) and elderly people with known cardiac or pulmonary disease (Linn et al., 2000). Moreover, cohort epidemiological studies have linked long-term exposure to particulate air pollution to a reduction of life expectancy due to cardiovascular mortality (Pope et al., 2004a). Although the underlying biological mechanism of these associations remains limited, several hypotheses have been postulated, from inflammation, accelerated atherosclerosis and altered cardiac autonomic function.
Since the 1980s, heart rate variability (HRV) has been widely used in clinical fields to stratify the risk of arrhythmic death of the patients with ischemic heart disease in whom a low HRV could be a negative predictor (Lombardi et al., 1996). Alterations of the autonomic nervous system accompanying the early stages of essential hypertension have also studied using HRV and it was found that sympathetic activity increases while parasympathetic decreases. Patients with congestive heart failure had clinical signs of enhanced sympathetic activity and progressive decrease in RR variance (Musialik-Lydka et al., 2003). A low HRV has been associated to an increased mortality rate in people with heart disease (Bigger et al., 1993; Fauchier et al., 2004).
Recent studies that included elderly individuals with heart diseases in Baltimore, Boston and Mexico City suggest that PM2.5 air pollution measured with ambient monitors was associated with a reduced HRV (Liao et al., 1999; Gold et al., 2000; Holguín et al., 2003; Park et al., 2005). The aim of this study was to test whether this association could also be observed in young healthy adults, using personal exposure monitors, at ambient levels currently observed in the Mexico City metropolitan area (MCMA).
Materials and methods
Protocol and Population
Between April and August 2002, 44 volunteers with a mean age of 27 years were recruited. All participants lived within the MCMA, which is located in a geographical basin at 2240 meters above the sea level and surrounded by mountains with an average height of 1000 m above the ground level, which prevent air pollution dissemination. The following inclusion criteria were fulfilled: no-smokers, not taking any medication and without a personal history of cardiovascular, pulmonary, neurological or endocrine disease. All subjects underwent 13 h Holter electrocardiographic (ECG) and personal PM monitoring during their daily activities from 0900 to 2200 hours.
The Institutional Ethics and Research Committees approved this study and all subjects signed an informed consent.
Holter ECG Monitoring and HRV
Holter monitoring was performed with a digital three-channel personal recorder (model 92,513, Burdik-Spacelabs, Dreefield, WI, USA), with a sampling speed of 200 Hz and 8-bit resolution. The skin was carefully prepared and electrodes were connected using modified V1 and V5 leads.
Data were processed using the software, Vision Premier™ System (version 2.0). Only segments without noise were analyzed. All ectopic beats were identified both automatically and manually and excluded from the analysis. All subjects had sinus heart rhythm. Only time domain indexes were utilized because no stationary recording periods were available; however, both type of indexes (time and frequency domain) are highly correlated (Task Force, 1996). These indexes are the standard deviation of all NN intervals (SDNN) and percentage of differences between adjacent normal RR intervals that are larger than 50 ms (pNN50), both calculated for 30-min periods.
PM Measurement
To assess exposure, participants received and carried a personal PM2.5 monitor. PM2.5 concentrations were measured using the pDR nephelometric method (personal DataRAM, pDR1200 (MIE Inc., Bedford, MA, USA), 2000). It consisted of a real-time active system, which was connected to a pump with suction flux set at 4 l/min. The equipment was calibrated previously according to the manufacturer's instructions. The sensitivity of this technique allows one to detect concentrations up to 0.001 mg/m3. Each minute concentration was averaged in 30 min periods to relate it to the preset time periods of the written diary. As pDR measurements can be biased if relative humidity (RH) is more than 70% (Liu et al., 2002), data were obtained from the environmental monitor network for each specific day in which PM2.5 measurements were performed. Average daily RH was below 70% the days in which all the measurements were made. No data about daily temperature or other pollutants concentrations were used because they were not always available from net monitors. Details of personal exposure data were published elsewhere (Vallejo et al., 2004).
Each individual completed a written diary, which classified their daily activities in indoor and outdoor microenvironments in a preset time period resolution of 30 min. Indoor situations included activities at home, at work, at school or in public places such as theaters, stores, restaurants, coffee shop and subway transportation. If participants were walking, standing or sitting in an open space, or if they were driving a car or using public transportation (bus or taxi), activities were classified as outdoor. The written diary considered separately the periods when participants were cooking or near a smoker. These measurements were excluded from the analysis since they only represented 3.2% of the total amount of measurements (33 samples). Participants were instructed to classify periods as indoor and outdoor exposure according to the microenvironment where they spent most of the time of each 30 min period. Microenvironments were not preassigned, since each individual was instructed to perform their usual activities. No measurements were made during weekends. The study was carried out during the rainy season (April–August 2002).
Other Variables
A questionnaire was administered regarding sociodemographic information (age, gender, and home and work addresses), and regular physical activity was defined as exercise that produces cardiovascular overload, increasing the ejection volume and heart rate, like running or swimming, at least 20 min, three times a week for the last 3 months (McArdle et al., 1991). Body mass index (BMI) was calculated as weight in kilograms divided by height in squared meters.
Statistical Analysis
Summary and dispersion estimates were used to describe the distribution of data that did not fit a normal pattern (Shapiro Wilk's test P=0.000). In order to achieve a normal distribution of the response variable, HRV indexes, SDNN and pNN50 were transformed into logarithmic scale (lnSDNN and lnpNN50). The HRV indexes autocorrelation was tested using partial and crossed correlation, and a first-order autoregressive correlation structure was identified.
Suspended particle matter data were classified as indoor and outdoor measurements according to the microenvironment indicated by participants in the diary of activities. Measurements were also classified according to the geographical location (northwest, northeast, center, southwest and southeast).
Multivariable analysis was carried out using linear mixed effects models that accounts for correlation within individuals. A first-order autoregressive correlation structure was used (Diggle et al., 1996) and each measurement Yij was modeled as

where Tij is the exposure variable for the individual i on the j time, Gi are the explanatory variables in the i subject fixed during all study, Zij are the explanatory variables that could change during the study, like microenvironment, for the individual i on the j time, β0, β1, β2 and β3 are the fix effect coefficients, ν is the random coefficient vector and ɛ is the random error term that follows the AR1 structure with the following distribution:

where  . Multivariate models were tested using different cumulative PM2.5 exposure periods previous to the 30 min of the HRV, the concurrent measurement of the 30 min and subsequent periods at 60, 90, 120, 150, 180 and 210 min in order to explore critical time exposure windows.
. Multivariate models were tested using different cumulative PM2.5 exposure periods previous to the 30 min of the HRV, the concurrent measurement of the 30 min and subsequent periods at 60, 90, 120, 150, 180 and 210 min in order to explore critical time exposure windows.
Model testing included fixed and variable factors over the monitoring period. Physical training, gender, BMI and age (both were introduced in the model as numerical kg/m2 and year of age, respectively) were fixed variables. Time of the day, included as 30 min preset periods, indoor and outdoor microenvironments, geographical location and PM2.5 (μg/m3) 30 min average concentration changed over the monitoring period. No random term for PM2.5 was included in the models.
Gender, BMI, physical training, indoor/outdoor microenvironments, geographical location and hours of the day were evaluated as effect modifiers and tested as interaction terms, but all P-values were in all cases >0.20; therefore, no interaction term was considered in the final models.
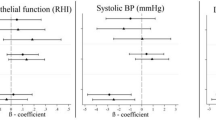
Final estimates are presented as the percent change in HRV per 30 μg/m3 of PM2.5 concentration, which is the interquartile range of the average personal exposure measurements in order to provide more meaningful figures (Figure 1).

Estimated pNN50 and its confidence intervals after 30 μg/m3 incremente in PM2.5 ambient concentrations.
Results
All 44 subjects had Holter ECG and PM2.5 personal exposure monitoring; four were eliminated, and the participation rate was of 91%. The losses were attributable to: PM2.5 personal monitors malfunction in two subjects, the presences of multiple premature ventricular beats in a young male and a 40-year-old woman decided to withdraw from the study because she was uncomfortable with the Holter ECG electrodes. The mean age of the participants was 27 years, range 21–35 years, and 29 were women. Average BMI was 24 kg/m2 and eighth of the participants exercised regularly. The median (25–75 percentiles) PM2.5 personal concentration exposure was 74 μg/m3 (49–111 μg/m3), the median (25–75 percentiles) SDNN was 74 ms (59–92 ms) and the pNN50 was 8.9% (4–19%). A description of HRV indexes behavior in relation to study covariables is shown in Table 1.
In Tables 2 and 3 estimated coefficients for accumulative exposure periods for both HRV indexes are shown. For lnpNN50, estimated association with PM2.5 increased significantly with each additional half hour until 1.5 and 2 h of prior exposure when the largest reduction in lnpNN50 was observed; after these periods, a lost statistical significance was found and precision became weaker due to the sample size reduction with each accumulative period. An interquartile increase in PM2.5 (30 μg/m3) in the previous 1.5 h was associated with a reduction in the pNN50 of 0.072%, with its maximum peak at 2 h, that is 0.08%, which are the same periods with the largest decrease in the pNN50 with a statistical significance.
Even though both indexes had a similar behavior, statistically significant association was only observed in lnpNN50 at 1.5 and 2 h, with negative coefficients. lnSDNN showed a decrease of the β-coefficient after three periods of accumulative exposure, the largest reduction started after 120 min; however, associations seen in this index were weaker than between PM2.5 and lnpNN50 (Table 3).
Discussion
This study is consistent with previous evidence that ambient PM2.5 air pollution is associated with decreased HRV, particularly for parasympathetic (vagal) modulation of cardiac autonomic function. This association was stronger at 1.5 and 2 h of accumulative personal exposure when adjusted for gender, age, physical training and BMI.
In order to compare these findings with previous studies, it is necessary to take into account different methods to evaluate HRV and methods to estimate exposure. The evaluation of the cardiac autonomic control through HRV requires certain conditions. While time domain indexes are statistical estimates of the variability of RR intervals, frequency domain indexes are the power spectral densities estimated through mathematical algorithms, usually the fast Fourier transformation; the first require long Holter monitoring periods to ensure a fairly large RR interval sample size and the second can be obtained from periods of 3–5 min of stationary recordings. Many frequency and time domain variables measured over the entire 24 h are strongly correlated with each other, that is the case of the SDNN, which correlates with the total power or the pNN50, which correlates with the high frequencies (HF) (Task Force, 1996). Some studies have used time domain indexes with 24 h ambulatory ECG. One included seven participants and involved monitoring only PM10 (Pope et al., 1999). Another study estimated the effect of average levels of PM2.5 and ozone over the previous 4 h on SDNN and rMSSD (Gold et al., 2000), and a study in Utah that included 88 participants examined PM's influence on cardiac autonomic function as measured by HRV (SDNN and rMSSD) and blood markers of inflammation (Pope et al., 2004b). All of them found that an increase in PM2.5 or in PM10, alone or combined with other pollutants like ozone, were associated with a reduction of the SDNN and of the rMSSD, only one study informed an increase of this last index (Gold et al., 2000). Studies in which frequency domain indexes were used also found this association, particularly of the HF of a parasympathetic-related index (Liao et al., 1999; Holguín et al., 2003; Park et al., 2005).
These studies have found that the elderly with or without cardiovascular conditions, hypertension or diabetes may be more responsive to airborne particle exposure and have a larger reduction of the HRV in relation to an increase in PM2.5 ambient concentrations (Liao et al., 1999; Pope et al., 1999, 2004b; Gold et al., 2000; Holguín et al., 2003). Our findings are consistent with those even though we studied young healthy adults; as expected, the magnitude of association was larger in those studies where susceptible individuals were included than in ours.
These researches in susceptible groups have helped to explain the short-term effects of PM2.5 air pollution and possible mechanisms of mortality displacement after pollution episodes as the 1952 “4 days fog” event in London with an increase in morbidity and mortality related to respiratory or cardiovascular disease (Logan et al., 1953; Bell and Davis, 2001). The possible mechanisms for the acute cardiovascular effects may include endothelial cell, platelet and leukocyte activation as part of inflammatory response, along with increased blood viscosity (Pope et al., 1999, 2004a) and physiological changes such as acute arterial constriction responses (Brook et al., 2002) that may trigger acute cardiovascular events.
We found stronger effects of PM2.5 in 1.5 and 2 h of accumulative exposure than in the concurrent 30 min. As air pollution concentration from 30 min were available, it was possible to evaluate several lagged models with end times matched to each participant's ECG recordings; however, no significant association was observed.
A potential limitation of this study is that PM2.5 concentrations were measured only during 13 consecutive hours in each participant; therefore, we were not able to evaluate the effect of air pollution on one or several subsequent days. However, Brook et al. (2002) found in healthy adults a significant vasoconstriction after 2 h inhalation of ≈150 μg/m3 of concentrated ambient fine particles plus ozone (120 ppb). With this study approach, cardiac autonomic control effects related PM2.5 air pollution, resulting in a decreased vagal tone with a predominance of the sympathetic activity, may be better understood in relation to short-term pollution episodes.
Most air pollution research has measured the exposure with fix monitors, in some cases data were taken from the environmental monitor network, which is known to be a good estimate but may be altered by weather conditions such as wind, rain or RH (Pope et al., 1999, Gold et al., 2000, Park et al., 2005). Other studies have used fixed indoor monitors (Liao et al., 1999; Holguín et al., 2003). Outdoor concentrations of PM2.5 are well correlated with ambient measurements; however, indoor pollutant levels are weekly correlated to outdoor ones. Since the use of ambient fixed monitors could not reflect personal exposure, we used personal monitors with continuous measurements that allowed one to assess the effects in shorter periods and different time windows.
The public health consequences of the effects found in a young healthy population in our study could be different from those informed in previous studies. A decrease of HRV is a common finding in the elderly and in patients with heart disease, which has been demonstrated to be a predictor of an increased mortality in both populations (Odemuyiwa et al., 1991; Tsuji et al., 1996). However, in the long term cardiac autonomic imbalance may play a role in the development of cardiovascular diseases. A reduction in the pNN50 suggesting a decreased parasympathetic cardiac autonomic control with sympathetic nervous system overactivity has been associated with the development of hypertension among previously normotensive men (Singh et al., 1998). Brook et al. (2002) reported preliminary results explaining how sympathetic stimulation through peripheral acute arterial constriction was related to PM as well as other pollutants exposure (Brook et al., 2002).
However, the significance of a decreased parasympathetic activity in the young healthy adults over a lifetime exposure in urban areas as Mexico City needs to be clarified. Further studies are needed to assess if these cardiac autonomic changes could be related to the association between PM2.5 air pollution and the increase in cardiovascular morbidity and mortality.
Individuals included in this study are representative of a population with exposure patterns mainly in in-door microenvironments, characterized by a sedentary lifestyle. Therefore, conclusions are limited to these types of subjects. Studies with a larger sample size that include individuals with different exposure patterns should be carried out in order to corroborate the results of this study. Additionally, no other copollutants such as O3, SO2 or PM10 were included because corresponding measurements were not always available in the city environmental monitor net.
References
Bell M.L., and Davis D.L. Reassessment of the lethal London fog of 1952: novel indicators of acute and chronic consequences of acute exposure to air pollution. Environ Health Perspect 2001: 109 (Suppl. 3): 389–394.
Bigger Jr J.T., Fleiss J.L., Fleiss J.L., Rolnitzky L.M., and Steinman R.C. Frequency domain measures of heart period variability to assess risk late after myocardial infarction. J Am Coll Cardiol 1993: 21: 729–736.
Brook R.D., Brook J.R., Bruce U., Urch B., Vincent R., Rajagopalan S., and Silverman F. Inhalation of fine particle air pollution and ozone causes acute arterial vasoconstriction in healthy adults. Circulation 2002: 105: 1534–1536.
Diggle P.J., Liang K.Y., and Zeger S.L. Analysis of Longitudinal Data. Clarendon Press, Oxford, UK, 1996.
Dockery D.W., and Pope III C.A. Acute respiratory effects of particulate air pollution. Ann Rev Public Health 1994: 15: 107–132.
Fauchier L., Babuty D., Melin A., Bonnet P., Cosnay P., and Fauchier J.P. Heart rate variability in severe right or left heart failure: the role of pulmonary hypertension and resistances. Eur J Heart Fail 2004: 1 (6): 181–185.
Gold D.R., Litonjua A., Shwartz J., Lovett E., Larson A., Nearing B., Allen G., Verriei M., Cherry R., and Verrier R. Ambient pollution and heart rate variability. Circulation 2000: 101: 1267–1273.
Holguín F., Téllez-Rojo M.M., Hernández M., Cortez M., Chow J.C., Watson J.G., Mannino D., and Romieu I. Air pollution and heart rate variability among the elderly in Mexico City. Epidemiology 2003: 5: 514–520.
Katsouyanni K., Zmirou D., Spix C., Sunyer J., Schouten J.P., Ponka A., Andreso H.R., Le Moullec Y., Wojtyniak B., Vigotti M.A., et al. Short-term effects of air pollution on health: a European approach using epidemiological time-series data. The APHEA project: Background, objectives, design. Eur Respr J 1995: 8: 1030–1038.
Liao D., Creason J., Shy C., Williams R., Watts R., and Zweidinger R. Daily variation of particulate air pollution and poor cardiac autonomic control in the elderly. Environ Health Perspect 1999: 107: 521–525.
Linn W.S., Szlachcic Y., Gong H., Kinney P.L., and Berhane K.T. Air pollution and daily hospital admissions in metropolitan of Los Angeles. Environ Health Perspect 2000: 108: 427–434.
Liu L.J., Slaughter J.C., and Larson T.V. Comparison of light scattering devices and impactors for particulate measurements in indoor, outdoor and personal environments. Environ Sci Technol 2002: 36: 2977–2986.
Logan W.P.D., Glag M.D., and Lond D. Mortality in the London fog incident, 1952. Lancet 1953: 14: 336–338.
Lombardi F., Malliani A., Pagani M., and Cerutti S. Heart rate variability and its sympatho-vagal modulation. Cardiovasc Res 1996: 32: 208–216.
McArdle W.D., Katch F.I., and Katch V.L. Training for anaerobic and aerobic power. In: McArdle W.D., Katch F.I., Katch V.L. (Eds.). Exercise Physiology, Energy and Nutrition and Humans Performance, 3rd edn. Lea and Febiger, Philadelphia, 1991, p 423–451.
Musialik-Lydka A., Sredniawa B., and Pasyk S. Heart rate variability in heart failure. Kardiol Pol 2003: 58 (1): 10–16.
Odemuyiwa O., Malik M., Farrell T., Bashir Y., Poloniecki J., and Camm J. Comparison of the predictive characteristics of heart rate variability index and left ventricular ejection fraction for all-cause mortality arrhythmic events and sudden death after acute myocardial infarction. Am J Cardiol 1991: 68: 434–439.
Park S.K., O’Neil M.S., Vokonas P.S., Sparrow D., and Schwartz J. Effects of air pollution on heart rate variability: the VA Normative Aging Study. Environ Health Perspect 2005: 113: 304–309.
Pope III A.C., Verrier R.L., Lovett E.G., Larson A.C., Raizenne M.E., Kanner R.E., Schwartz J., Villegas M., Gold D., and Dockery D. Heart rate variability associated with particulate air pollution. Am Heart J 1999: 138: 890–899.
Pope III C.A., Burnett R.T., Thurston G.D., Thun M.J., Calle E.E., Krewski D., and Godleski J.J. Cardiovascular mortality and long term exposure to particulate air pollution. Epidemiological evidence of general pathophysiological pathways of disease. Circulation 2004a: 109: 71–77.
Pope III C.A., Hansen M.L., Long R.W., Nielsen K.R., Eatough N.L., Wilson W.E., and Eatough J.D. Ambient particulate air pollution, heart rate variability and blood markers of inflammation in panel of elderly subjects. Environ Health Perspect 2004b: 112: 339–345.
Schwartz J., Dockery D.W., Neas L.M., Wypij D., Ware J.H., Spengler J.D., Koutrakis P., Speizer F.E., and Ferris B.G. Acute effects of summer air pollution on respiratory symptom reporting a children. Am J Respir Crit Care Med 1994: 150: 1234–1242.
Singh J.P., Larson M.G., Tsuji H., Evans J.C., O’Donnell C.J., and Levy D. Reduce heart rate variability and new-onset hypertension: insights into pathogenesis of hypertension, the Framingham Heart Study. Hypertension 1998: 32: 293–297.
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation and clinical use. Circulation 1996: 93: 1043–1065.
Tsuji H., Larson M.G., Venditti F.J., Manders E.S., Evans J.C., Feldman C.L., and Levy D. Impact of reduced heart rate variability on risk for cardiac events. Framingham Heart Study. Circulation 1996: 94: 2850–2855.
Vallejo M., Lerma C., Infante O., G-Hermosillo A., Riojas-Rodriguez H., and Cárdenas M. Personal exposure to particulate matter less than 2.5 μm in Mexico City: a pilot study. J Exp Anal Environ Epidemiol 2004: 14: 323–329.
Wong C.M., Ma S., Hedley A.J., and Lam T.H. Effect of air pollution on daily mortality in Hong Kong. Environ Health Perspect 2001: 109: 335–340.
Zanobetti A., Shwartz J., and Dockery D.W. Airborne particles are a risk factor for hospital admissions for heart and lung disease. Environ Health Perspect 2000: 108: 1071–1077.
Acknowledgements
We express our deepest gratitude to the individuals who participated voluntarily in this study and thank Ms Betty Lou Chin R.N. for her support in the preparation of the manuscript, and Dr Manlio F Marquez for interpreting Holter data. Financial support for this study was provided by Sectorial Fund CONACyT/Semarnat No. 047.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vallejo, M., Ruiz, S., Hermosillo, A. et al. Ambient fine particles modify heart rate variability in young healthy adults. J Expo Sci Environ Epidemiol 16, 125–130 (2006). https://doi.org/10.1038/sj.jea.7500447
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jea.7500447
Keywords
This article is cited by
-
Effect of L-Ascorbic Acid on Nickel-Induced Alteration of Cardiovascular Pathophysiology in Wistar Rats
Biological Trace Element Research (2020)
-
Heavy metals in the gold mine soil of the upstream area of a metropolitan drinking water source
Environmental Science and Pollution Research (2016)
-
Cardiac effects of seasonal ambient particulate matter and ozone co-exposure in rats
Particle and Fibre Toxicology (2015)
-
Elevated particle number concentrations induce immediate changes in heart rate variability: a panel study in individuals with impaired glucose metabolism or diabetes
Particle and Fibre Toxicology (2015)
-
Noninvasive effects measurements for air pollution human studies: methods, analysis, and implications
Journal of Exposure Science & Environmental Epidemiology (2015)
