
Abstract
The purpose of this study is to report two patients with retained rigid gas-permeable contact lenses (RCLs) that had become integrated into the upper eyelid tissues, to provide a brief literature review and to discuss possible aetiologies. The methods used in this study are as follows: retrospective review of clinical records and review of the literature. Two contact lens wearers presented with an upper eyelid mass, one after previous loss of a lens and the other 40 years after a failed trial of RCL wear; this latter case appears to be the longest delay in diagnosis reported in the ophthalmic literature. Although extremely rare, the presence of an upper tarsal lump in a RCL wearer should raise possibility of an embedded contact lens, particularly where the contour is suggestive in size or shape. Ultrasonography or magnetic resonance imaging may show characteristic changes. It is probable that RCL migration into periocular tissues occurs by entrapment above the upper tarsal border and integration, by local tissue necrosis, into the tarsus or pretarsal space.
Similar content being viewed by others


Introduction
Integration of a rigid contact lens (RCL) into the upper eyelid is an uncommon cause of an eyelid lump or ptosis,1, 2, 3, 4, 5, 6, 7, 8, 9, 10 and may present late after loss of a lens. But for the presence of an eyelid swelling, almost half of all reported cases remained clinically silent.
We present two cases of lost contact lenses presenting as eyelid masses, one being a lens that had been placed 40 years before presentation.
Case reports
Case 1
An 81-year-old aphakic man presented with 6 months of progressive left upper eyelid swelling, associated with mild inflammation. A 1 cm diameter firm mass was palpable within the upper eyelid and eversion of the lid showed a normal tarsal conjunctiva (Figure 1a). Exploration through an upper eyelid skin incision revealed a fibrous capsule tightly adherent to the pretarsal surface which, when opened, released a mucoid substance surrounding a RCL (Figure 1b). The lens was removed intact (Figure 1c) and the cavity had a smooth lining with no evidence of inflammation (Figure 1d). Although usage of a contact lens was initially denied, the patient eventually recalled a trial of fitting for aphakic contact lenses soon after cataract surgery 40 years before presentation.

Case 1. (a) Normal tarsus on eversion, (b) mucoid debris within the pretarsal fibrous capsule, and (c) rigid contact lens removed from within the cavity. (d) Uninflamed smooth lining to the fibrous capsule.
Case 2
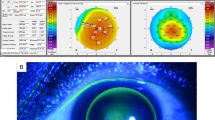
A 50-year-old myopic male who had used RCLs for some decades, developed a left upper lid mass over 6–8 months. A prominent firm mass was visible on the anterior surface of the eyelid (Figure 2a) and a raised mass was present on the tarsal conjunctival surface, with prominent abnormal overlying blood vessels (Figure 2b) and mild inflammation. Due to suspected meibomian cell carcinoma an incisional biopsy was performed; however on infiltrating the tissue with local anaesthetic a firm mass was felt against the needle. The pre-tarsal space was opened through a conjunctival incision just above the tarsus and a RCL was found within the cavity of a fibrous capsule (Figure 2c). The patient could not recall an episode of contact lens loss.

Case 2. (a) Prominent mass visible on the anterior surface of the left upper eyelid and (b) tarsal examination revealing an elevated ring of tissue surrounding a central crater (the ‘O’ sign), with some prominent overlying blood vessels. (c) Rigid contact lens removed from cavity of a fibrous capsule, using a supratarsal conjunctival incision.
Discussion
Migration of a RCL into the periocular tissues has been reported fairly often,3, 4, 5, 6, 7, 8, 9, 10 with the time between loss of a RCL and retrieval being reported as between 2 and 84 months. The exceptionally long period of one of our patients (40 years; case 1) appears to be unique.
Eversion of the eyelid should be performed in all patients with a tarsal mass or who have ‘lost’ a RCL4, 5 and the presence of a conjunctival ‘O’ sign, an elevated ring of tissue surrounding a central crater (Figure 3b) may be suggestive of retained RCL.6 Two-thirds of reported cases presented with an upper eyelid mass and about half had only painless swelling. Contact lenses have been found in various locations, including the anterior lamella,4, 5 within tarsus,9 subconjunctivally,2, 3, 6 between the anterior and posterior lamellae,2, 8 and in the anterior orbit.7, 10 One author (GER) recalls discovering three RCLs sequestered in the capacious upper fornix of an aphakic patient who had been experiencing vague discomfort; the lower border of the lenses had lodged onto the upper border of the tarsus.

Bock's ‘upper fornix trap’.12 (reproduced, with permission, from the British Journal of Ophthalmology) (license number: 2693240483181). Inverted contact lens in the upper fornix with its lower border wedged into the upper tarsal edge.
Magnetic resonance imaging can show a curvilinear signal in the tissues8 and B-mode ultrasonography, an acoustically void oval mass.3
The release of serous3, 8 or mucopurulent4, 5, 6 fluid from the surgical site has been noted and the tissues around the lens variously reported as nonspecific granulation tissue,2, 5, 7, 9, 10 fibrous tissue capsule,3, 5, 7, 8, 9, 10 or a cavity lined with conjunctival epithelium.2, 4, 7 The histological spectrum is likely to reflect the tissue response according to the duration of RCL retention.11
Bock12 has described the ‘upper fornix trap’ (Figure 3), a mechanism also suggested by the anecdotal patient with three retained contact lenses. Once displaced into the upper fornix, the RCL engages the upper border of the tarsal plate and slowly erodes through to the subconjunctival space encouraged by eyelid movement combined with inflammatory pressure necrosis. Such a mechanism is more likely when the RCL has flipped ‘upside down’ (concave anteriorly). Resolution of the acute inflammatory response is followed by the appearance of granulation tissue and ultimately the formation of a fibrous capsule.11 Sequestration of conjunctival epithelium within the RCL cavity appears rare,4 but the presence of milky fluid around the lens might suggest its presence and was seen in case 1. The absence of granulation tissue on histological examination would suggest resolution of the subacute inflammatory response.
Conclusion
In a RCL wearer, the presence of a persistent lump or ptosis should raise the suspicion of a retained lens, even if the lens wear was discontinued many years before presentation.

References
Shenken E . Traumatic dislocation of a contact lens into the eyelid. Can Med Assoc J 1969; 101: 295–296.
Older JJ . Encysted corneal contact lens presenting as an eyelid mass. Ann Ophthalmol 1979; 11: 1393–1394.
Beyer-Machule CK, Shapiro A . Eyelid penetration of a hard contact lens, simulating a neoplasm. Ophthalmic Surg 1986; 17: 101–102.
Jones D, Livesey S, Wilkins P . Hard contact lens migration into the upper lid: an unexpected lid lump. Br J Ophthalmol 1987; 71: 368–370.
Hornblass A, Kass LG . Contact lenses in the upper eyelid masquerading as lid masses. Ophthalmic Surg 1987; 18: 438–440.
Bellan L, Buffam F . The ‘O’ sign—clue to a lost lens. Can J Ophthalmol 1990; 25: 348–350.
Roberts-Harry TJ, Davey CC, Jagger JD . Periocular migration of hard contact lenses. Br J Ophthalmol 1992; 76: 95–97.
Hammons M, Gayre G, Hammons D, Dutton J . Intrapalpebral migration of a rigid gas-permeable contact lens resulting in an eyelid mass. Ophthalmology 2003; 110: 1781–1783.
Hayasaka Y, Hayasaka S, Nagaki Y, Endo Y . An eyelid mass caused by a migrated hard contact lens. Eye Contact Lens 2003; 29: 250–251.
Nicolitz E, Flanagan JC . Orbital mass as a complication of contact lens wear. Arch Ophthalmol 1978; 96: 2238–2239.
Anderson JM, Rodriguez A, Chang DT . Foreign body reaction to biomaterials. Semin Immunol 2008; 20: 86–100.
Bock RH . The upper fornix trap. Br J Ophthalmol 1971; 55: 784–785.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
This case series was presented at the British Oculoplastic Surgeons Society Meeting in Newcastle in 2008.
The images belong to the authors and therefore permission was not required.
Rights and permissions
About this article
Cite this article
Shams, P., Beckingsale, A., Sheldrick, J. et al. An unusual eyelid lump: unsuspected embedded contact lens for up to 40 years. Two cases and literature review. Eye 25, 1371–1373 (2011). https://doi.org/10.1038/eye.2011.136
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2011.136
Keywords
This article is cited by
-
Folded bandage contact lens retention in a patient with bilateral dry eye symptoms: a case report
BMC Ophthalmology (2017)
