
Abstract
Hypertensive crisis (HC) stands out as one type of acute elevation in blood pressure (BP) and can manifest as hypertensive emergency (HE—with target-organ damage (TOD)) or hypertensive urgency (HU—without TOD), usually accompanied by levels of diastolic BP ⩾120 mm Hg. The aim of this study was to characterize the clinical–epidemiological profile of HC over the course of 1 year in a university reference hospital and perform a review of the literature. The study was a cross-sectional study, conducted over a period of 1 year (2006) in 362 patients who presented for treatment at the emergency hospital with HC, as described above. Among all patients examined, 231 individuals met the criteria for HE and 131 met the criteria for HU. Patients with HE were older (P<0.001) and more sedentary (P=0.026) than those with HU. Furthermore, fewer HE patients than HU patients had previously undergone antihypertensive treatment (P=0.006). The groups did not differ regarding BP levels, gender, smoking or body mass index. Dyspnea (41.1%), thoracic pain (37.2%) and neurological deficit (27.2%) were common signs/symptoms in those with HE. Meanwhile, in the group with HU, we most frequently found headache (42.0%), thoracic pain (41.2%) and dyspnea (34.3%). Among the forms of HE, we most frequently observed acute lung edema (30.7%), myocardial infarction/unstable angina (25.1%), and ischemic (22.9%) and hemorrhagic (14.8%) stroke. HC is a clinical entity associated with high morbidity in the emergency room. Individuals with HE are older and sedentary and have lower rates of antihypertensive treatment. Adequate control of BP should be pursued as a way to avoid this severe complication of hypertension.
Similar content being viewed by others


Introduction
Hypertension is a worldwide health problem that increases the costs to public health systems and, as such, merits special emphasis. One presentation or even consequence of inadequate blood pressure (BP) control is hypertensive crisis (HC), a condition defined as a fast, inappropriate, intense and symptomatic increase in BP (diastolic BP generally ⩾120 mm Hg). HC may manifest as either a hypertensive emergency (HE) or an urgency (HU); HE is characterized by rapid deterioration of target organs (heart, brain, kidneys and arteries), and poses an immediate threat to life, a situation not found in HU.1 An important differential diagnosis for HC, mainly with HU, is the pseudocrisis phenomenon.1 Certain patients, independent of BP levels, present neither evidence of acute target-organ damage (TOD) nor an immediate threat to life, which obviates the need for antihypertensive therapy in the emergency room. This condition occurs usually in oligosymptomatic or asymptomatic hypertensive patients, whose BPs, although under treatment, are not controlled and are typically elevated. Another group of hypertensive patients may have a transient BP elevation caused by any emotional, painful or uncomfortable event, such as migraine, vertigo or headache of muscle-skeletal origin, and manifestations of panic disorder. Such symptoms characterize hypertensive pseudocrisis.2, 3
Although these conditions are well described, few studies compare the characteristics of individuals with HU and HE.2, 4, 5, 6, 7, 8, 9, 10, 11 This study aimed to analyze the clinical–epidemiological profile of HC over the course of 1 year in a university reference hospital and to perform a review of the literature.
Methods
A total of 362 individuals aged ⩾18 years presenting HC and having been admitted to the Clinical Emergency Department at the university hospital during 2006 were evaluated in this study. The criteria proposed by the Seventh Joint National Committee were used for the definition of HC.1 HEs are characterized by severe elevations in BP complicated by evidence of impending or progressive TOD (hypertensive encephalopathy, hemorrhagic and ischemic strokes, acute myocardial infarction, acute left ventricular failure with pulmonary edema, unstable angina pectoris, dissecting aortic aneurysm and acute/progressive renal insufficiency). HUs are those situations associated with severe elevations in BP without TOD.1
All patients underwent physical examination and diagnostic tests after signing an informed consent previously approved by the ethics research committee. In the absence of conditions that allowed for signing, participation was authorized by the parents or guardians.
This study excluded female patients presenting with preeclampsia and eclampsia, hypertensive patients with pseudocrisis and those with diastolic BP <120 mm Hg. BP was measured by the standard technique recommended,12 using the average of three BP measurements obtained with a mercury sphygmomanometer.
Previous diagnosis of hypertension was identified through examination of the medical history or use of antihypertensive drugs. Previous diabetes mellitus was recognized by medical history or use of hypoglycemic drugs. Patients were considered smokers when they had active smoking habits or a previous history of smoking. Sedentary lifestyle was recognized as those who reported participating in physical activity for a period <20 min per day and less frequently than three times a week. Electrocardiograms and measurements of creatine kinase M-band (CK-MB) and troponin were performed when coronary ischemia was suspected, and computed tomography was used for the evaluation of brain damage, for example, during the suspicion of stroke and hypertensive encephalopathy. Renal function was assessed by serum creatinine at hospital admission, clinical history of changes in urinary volume and clinical outcome (indication for dialysis in the emergency room). The literature review was based on articles published and available in PubMed and Google Scholar databases.
Descriptive analysis was performed for qualitative variables and quantitative results are presented as means and standard deviation. To compare patient characteristics, Student's t-test or the Mann–Whitney test was used for quantitative variables and χ2 or Fisher's exact test was used for qualitative variables. All analysis was carried out using Minitab 15.0 (Minitab Inc., State College, PA, USA), allowing an α error of 5%, with a significance level of P<0.05.
Results
In 2006, 79 463 patients ⩾18 years of age were treated in the emergency department. The prevalence of HC corresponded to 0.45% of all emergencies and 2.0% of clinical emergencies. In all, 362 cases met the inclusion criteria of HC, with 231 cases of HE (63.8%) and 131 (36.2%) of HU. Patients with HE had a higher mean age (63.4±13.4 vs. 57.1±15.6 years, P<0.001), a higher frequency of sedentary lifestyle (87.7 vs. 78.1%, P=0.026) and a lower rate of previous antihypertensive treatment (71.0 vs. 83.9%, P=0.006) than those with HU. The groups did not differ (P>0.05) with regard to gender, systolic and diastolic BP, body mass index, waist circumference, history of smoking, known history of diabetes or hypertension (Table 1).
Signs and symptoms most commonly found in the study group as a whole, in descending order, were chest pain, dyspnea, headache, neurological deficit, dizziness and paresthesia (Table 2). In HU patients, headache (42.0%) and chest pain (41.2%) were the most common, whereas in HE, the most frequent were dyspnea (41.1%), chest pain (37.2%) and neurological deficit (27.3%). These findings are compatible with the TOD observed in this study.
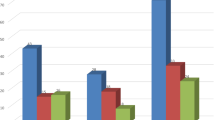
Of the 231 patients who presented HE during the analyzed period (Figure 1), 137 had cardio-related events (71 patients presented acute pulmonary edema, 30 had acute myocardial infarction, 28 had unstable angina and 8 presented with acute aortic dissection); 94 experienced brain-related events (53 patients with ischemic stroke, 26 with hemorrhagic stroke, 8 with subarachnoid hemorrhage and 6 with hypertensive encephalopathy) and 1 patient experienced a kidney-related event (acute and progressive renal insufficiency).

Distribution of acute TOD in patients who presented with HE, according to organ involvement (a) and etiology (b).
Discussion
In this study, we analyzed the clinical–epidemiological profile of HC in individuals admitted to the emergency department. Subjects with HE were older, more sedentary and more frequently Caucasian than those with HU. Unlike the findings of Zampaglione et al.,4 Martin et al.2 and Cerrilo et al.,6 we found no significant difference in the values of systolic and diastolic BP between the two groups. These studies also demonstrate that individuals with HE were older than those with HU.2, 4, 6
In contrast to our findings, other investigators 2, 4, 5, 6, 7, 8, 9, 10, 11 (Table 3) found a greater prevalence of HU in their HC samples. Despite the fact that most studies have been conducted in tertiary hospitals, there is a tendency for less severe conditions to be treated in primary care,8 which prevents overloading the tertiary service centers. In addition, our hospital serves as a referral service for many cities, attending primarily to seriously ill patients that require complex and specialized care.
As previously discussed by Martin et al.,2 the high prevalence rate of hypertensive crises reported by Zampaglione et al.4 may have resulted from the inclusion of cases of hypertensive pseudocrisis, which may imitate HU. The presence of pseudocrisis is often confused with HC and inadequately treated.2, 3 Monteiro, Jr. et al.13 found that only 16% of patients treated in an emergency room with presumed HC met the diagnostic criteria. Sobrinho et al.3 demonstrated a 48% prevalence of pseudocrisis, and 94% of these patients received inappropriate treatment (antihypertensive drugs), as they were patients with HC.
Another aspect that we want to highlight is a discrepancy related to the gender distribution of patients who presented with HC (Table 3). Although world data estimates suggest that there is no difference in hypertension prevalence between genders,1 most previously published studies found a higher prevalence of HC among women.2, 4, 5, 6 This statistic could mean that women are more aware of their condition and more frequently seek primary care,14 despite the fact that males tend to have more serious complications related to hypertension, as evidenced by the higher rate of HE presentation found among males.2, 6, 15 Despite the slightly higher prevalence of HC in women, our results suggest that this prevalence represents an underestimation. Although most patients with eclampsia or preeclampsia have clinical symptoms, they are treated as emergency cases in the obstetrics department when they arrive at our hospital. Therefore, such patients were excluded from our analysis.
As can be seen in Table 3, less than a quarter of the population had no previous knowledge of their disease in all studies, suggesting that something was amiss with the treatment of these hypertensive patients. One of the possible factors involved in the genesis of HC may have been the mismanagement of or non-compliance with antihypertensive treatment.16, 17, 18 In our study, significantly more patients with HU compared with HE had previously received antihypertensive treatment, which reinforces this hypothesis.
Dosse et al.19 showed in a series of hypertensive patients that 61.76% of those surveyed attended the medical consultations, 86.76% did not comply with the medication regimen and 85.29% did not comply with the non-medication regimen, as represented by reporting at least one non-healthy lifestyle habit. Another important factor involved in the occurrence of HC is the rate of hypertensive control. In a study of a Brazilian population, Moreira et al.14 showed that the percentage of BP control among all hypertensive individuals was 38.6%. Among treated hypertensive patients, this percentage was 52.9% and was even higher in the population with more years of schooling, which also was of a higher socioeconomic class. There was no significant difference associated with age group or gender. These rates are between 15.2 and 47.7% in Europe,20, 21, 22, 23 19.6% in Brazil,24 3.9 and 30.6% in China25, 26, 27 and 50.1% in the United States, as determined by the National Health and Nutrition Examination Survey 2007–2008.28
The signs and symptoms presented on admission to the hospital vary according to the clinical presentation of HC, depending on which target organs are affected most severely. In our sample, because of the higher frequency of strokes, acute pulmonary edema and acute coronary syndromes, the most common signs/symptoms were dyspnea, chest pain, headaches and neurological deficit. Such findings are in accordance with the majority of previous studies.2, 4, 5, 6, 7, 8, 9, 10, 11 The HE presentation was also similar to those found in other samples (Table 3).
Recently, Saguner et al.18 described several potential risk factors for HC in a sample of 85 hypertensive patients followed-up for 1.6±0.3 years. The main risk factors were female gender, high degree of obesity, presence of hypertensive or coronary heart disease, somatoform disorder, higher number of antihypertensive drugs and non-adherence to treatment regimens. Despite being one of the first prospective studies to assess risk factors for HC, the findings are worthy of careful consideration. First, to classify all events as HC, the investigators may have included patients with hypertensive pseudocrisis in this series, a fact that leads to misclassification of cases of HC, which could be confirmed by the inclusion of individuals with somatoform disorders. Moreover, both the sample size and the relatively short follow-up duration, as highlighted by the investigators, may have contributed to some of these findings.
Finally, one limitation that should be mentioned is the miscegenation of the Brazilian population. Despite the well-established higher incidence of HC in black individuals,29 the color of the skin is a weak predictor of the ethnic background of individuals in our region,30 which led us to disregard this variable in our analysis. The dynamics of the hospital, which dictated that pregnant patients were treated as special emergency cases, also precluded the inclusion of patients admitted with eclampsia and preeclampsia in our analysis. Another limitation that must be highlighted is the lack of standardization in the definition of HC, which prevented the comparison of our results to those obtained in other studies.
In conclusion, this study highlights the importance of knowing the clinical presentation of HC in the emergency room and of describing the symptoms, clinical profile and TOD in individuals who present with HC. Appropriate measures of BP control should be pursued as a way to avoid this severe complication of hypertension.
References
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Jr JL, Jones DW, Materson BJ, Oparil S, Wright Jr JT, Roccella EJ, Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003; 42: 1206–1252.
Martin JF, Higashiama E, Garcia E, Luizon MR, Cipullo JP . Hypertensive crisis profile. Prevalence and clinical presentation. Arq Bras Cardiol 2004; 83: 125–130.
Sobrinho S, Correia LC, Cruz C, Santiago M, Paim AC, Meireles B, Andrade M, Kerner M, Amoedo P, de Souza CM . Occurence rate and clinical predictors of hypertensive pseudocrisis in emergency room care. Arq Bras Cardiol 2007; 88: 579–584.
Zampaglione B, Pascale C, Marchisio M, Cavallo-Perin P . Hypertensive urgencies and emergencies. Prevalence and clinical presentation. Hypertension 1996; 27: 144–147.
Tomero EP, Alonso SJ, Laguna P . Hypertensive crises at the hospital emergency services. The SUHCRIHTA study. Emergencias 2001; 13: 82–88.
Cerrilo MR, Hernández PM, Pinilla CF, Claros NM, Otero ML . Hypertensive crises: prevalence and clinical aspects. Rev Clin Esp 2002; 202: 255–258.
Piedra-León M, García-Gómez MC, Mendoza NV, Fernández-Fresnedo G, Arias M . Análisis clínico de las crisis hipertensivas tratadas en el servicio de urgências de un hospital de tercer nível. Hipertensión 2007; 24: 185–186.
Capdevila CG, Blanco CA, García JAM, Jordana NM . Comparación entre La actuación hospitalaria y La de Atención Primaria ante las crisis hipertensivas. Hipertensión (Madr) 2008; 25: 126–128.
Lanthier L, Malenfant L, Lacelle M-J . Characteristics of hypertensive emergencies and urgencies at Sherbrooke between 1998 and 2006. Can J Gen Intern Med 2008; 3: 38–40.
Serrano VC, Freites GQ, Delgado LL, García BMF . Behavior of the hypertensive crisis present in patients from NA integral diagnosis medical center. Rev Cubana Med Gen Integr 2009; 25: 129–135.
Al-Bannay R, Husain AA . Hypertensive crisis. Clinical presentation, comorbidities, and target organ involvement. Saudi Med J 2010; 30: 916–920.
O’Brien E, Asmar R, Beilin L, Imai Y, Mancia G, Mengden T, Myers M, Padfield P, Palatini P, Parati G, Pickering T, Redon J, Staessen J, Stergiou G, Verdecchia P, European Society of Hypertension Working Group on Blood Pressure Monitoring. Practice guidelines of the European Society of Hypertension for clinic, ambulatory and self blood pressure measurement. J Hypertens 2005; 23: 697–701.
Monteiro Jr FC, Anunciação FA, Salgado Filho N, da Silva GM, Barbosa JB, Ferreira PA, Lages J, Mandarino NR, da Silva Júnior WS, Monteiro CC . Prevalence of true hypertensive crises and appropriateness of the medical management in patients with high blood pressure seen in a general emergency room. Arq Bras Cardiol 2008; 90: 247–251.
Moreira GC, Cipullo JP, Martin JF, Ciorlia LA, Godoy MR, Cesarino CB, Cordeiro JA, Lupino PL, Ciorlia G, Burdmann EA . Evaluation of the awareness, control and cost-effectiveness of hypertension treatment in a Brazilian city: populational study. J Hypertens 2009; 27: 1900–1907.
Bennett NM, Shea S . Hypertensive emergency: case criteria, sociodemographic profile, and previous care of 100 cases. Am J Public Health 1988; 78: 636–640.
Shea S, Misra D, Ehrlich MH, Field L, Francis CK . Predisposing factors for severe, uncontrolled hypertension in an inner-city minority population. N Engl J Med 1992; 327: 776–781.
Tisdale JE, Huang MB, Borzak S . Risk factors for hypertensive crisis: importance of out-patient blood pressure control. Fam Pract 2004; 21: 420–424.
Saguner AM, Dür S, Perrig M, Schiemann U, Stuck AE, Bürgi U, Erne P, Schoenenberger AW . Risk factors promoting hypertensive crises: evidence from a longitudinal study. Am J Hypertens 2010; 23: 775–780.
Dosse C, Cesarino CB, Martin JF, Castedo MC . Factors associated to patients’ noncompliance with hypertension treatment. Rev Lat Am Enfermagem 2009; 17: 201–206.
Psaltopoulou T, Orfanos P, Naska A, Lenas D, Trichopoulos D, Trichopoulou A . Prevalence, awareness, treatment and control of hypertension in a general population sample of 26,913 adults in the Greek EPIC study. Int J Epidemiol 2004; 33: 1345–1352.
Scheltens T, Bots ML, Numans ME, Grobbee DE, Hoes AW . Awareness, treatment and control of hypertension: the ‘rule of halves’ in an era of risk-based treatment of hypertension. J Hum Hypertens 2007; 21: 99–106.
Aguado A, López F, Mirayet S, Oriol P, Fuentes MI, Henares B, Badia T, Esteve L, Peligro J . Hypertension in the very old; prevalence, awareness, treatment and control: a cross-sectional population-based study in a Spanish municipality. BMC Geriatr 2009; 9: 16.
Costanzo S, Di Castelnuovo A, Zito F, Krogh V, Siani A, Arnout J, Cappuccio FP, Miller MA, van Dongen M, de Lorgeril M, de Gaetano G, Donati MB, Iacoviello L, European Collaborative Group of the IMMIDIET project. Prevalence, awareness, treatment and control of hypertension in healthy unrelated male-female pairs of European regions: the dietary habit profile in European communities with different risk of myocardial infarction–the impact of migration as a model of gene-environment interaction project. J Hypertens 2008; 26: 2303–2311.
Sociedade Brasileira de Cardiologia/Sociedade Brasileira de Hipertensão/Sociedade Brasileira de Nefrologia. VI Diretrizes Brasileiras de Hipertensão. Arq Bras Cardiol 2010; 95 (Suppl 1): 1–51.
Wu Y, Hyxley R, Li L, Anna V, Xie G, Yao C, Woodward M, Li X, Chalmers J, Gao R, Kong L, Yang X, China NNHS Steering Committee; China NNHS Working Group. Prevalence, awareness, treatment, and control of hypertension in China: data from the China National Nutrition and Health Survey 2002. Circulation 2008; 118: 2679–2686.
Hu DY, Liu LS, Yu JM, Yao CH, China STATUS Study Group. National survey of blood pressure control rate in Chinese hypertensive outpatients-China STATUS. Zhonghua Xin Xue Guan Bing Za Zhi 2010; 38: 230–238.
Li H, Meng Q, Sun X, Salter A, Briggs NE, Hiller JE . Prevalence, awareness, treatment, and control of hypertension in rural China: results from Shandong Province. J Hypertens 2010; 28: 432–438.
Egan BM, Zhao Y, Axon RN . US trends in prevalence, awareness, treatment, and control of hypertension, 1988-2008. JAMA 2010; 303: 2043–2050.
van den Born BJ, Koopmans RP, Groeneveld JO, van Montfrans GA . Ethnic disparities in the incidence, presentation and complications of malignant hypertension. J Hypertens 2006; 24: 2299–2304.
Parra FC, Amado RC, Lambertucci JR, Rocha J, Antunes CM, Pena SD . Color and genomic ancestry in Brazilians. Proc Natl Acad Sci USA 2003; 100: 177–182.
Acknowledgements
This study was supported by grants from the Faculdade de Medicina de São José do Rio Preto (FAMERP) and Conselho Nacional de Pesquisa (CNPq).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Vilela-Martin, J., Vaz-de-Melo, R., Kuniyoshi, C. et al. Hypertensive crisis: clinical–epidemiological profile. Hypertens Res 34, 367–371 (2011). https://doi.org/10.1038/hr.2010.245
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2010.245
Keywords
This article is cited by
-
Determinants of hypertensive crisis among hypertensive patients at adult emergency departments of public hospitals in Addis Ababa, Ethiopia, 2021: a case–control study
International Journal of Emergency Medicine (2023)
-
Hypertensive emergencies and urgencies: a preliminary report of the ongoing Italian multicentric study ERIDANO
Hypertension Research (2023)
-
Clinico-epidemiological profile and risk factors of hypertensive crisis among patients attended at a tertiary care hospital in Somalia
Scientific Reports (2023)
-
A Systematic Review and Meta-analysis of the Clinical and Epidemiological Characteristics of Patients with Hypertensive Emergencies: Implication for Risk Stratification
High Blood Pressure & Cardiovascular Prevention (2023)
-
Is headache at admission associated with higher rate of recent brain MRI injury during malignant hypertension crisis?
Journal of Human Hypertension (2022)
