
Abstract
Because subclinical alterations in cardiovascular structure reflect cumulative damage induced by risk factors and represent an intermediate stage between risk factor exposure and cardiovascular events, this damage is regarded as a marker of increased cardiovascular risk in different clinical settings, including the general population. The Pressioni Monitorate e Loro Associazioni (PAMELA) is an originally designed research study aimed at assessing the normal values and prognostic significance of ambulatory and home blood pressure in a representative sample of the Northern Italian general population. Because the study protocol included the collection of electrocardiographic (ECG) and echocardiographic (ECHO) data, the prevalence and clinical correlates, as well as the prognostic value of subclinical cardiac alterations, have been extensively investigated. This article is a review of the findings of the PAMELA study regarding the clinical aspects and prognostic significance of cardiac abnormal phenotypes such as left ventricular hypertrophy, left atrial dilatation and aortic root dilation.
Similar content being viewed by others

Introduction
Hypertensive subclinical organ damage is an intermediate step in the progression of cardiovascular disease and is a powerful predictor of cardiovascular outcomes. Reversal of target organ damage is regarded to be a reliable intermediate end point of an effective antihypertensive treatment. Among the markers of subclinical organ damage, cardiac alterations, as assessed by ECG or echocardiography (ECHO), play a key role in the clinical work-up of hypertensive patients owing to the wide availability, acceptable costs and undisputed value of both techniques in predicting cardiovascular events.
The PAMELA Study (Pressioni Arteriose Monitorate E Loro Associazioni) is an epidemiologic study designed to determine the normal values and prognostic significance of ambulatory and home blood pressure (BP) in the population. Because the study protocol included the collection of ECG and ECHO data, we were able to examine the presence of subclinical cardiac alterations at the community level.
The main features of this research project can be briefly summarized as follows. The PAMELA Study started in 1990–1991 and included 3200 individuals aged 25–74 years who were randomly selected from among the residents in Monza (Italy). The participation rate was 64%; thus, complete baseline data were collected in 2051 subjects (Table 1).
After their informed consent had been obtained during the initial visit, all subjects underwent the following procedures: medical history and physical examination, three sphygmomanometric BP measurements in the sitting position, blood and urine sampling and standard 12-lead ECG and ECHO. On the same day, all subjects were fitted with an ambulatory BP monitoring device. In addition, each subject was given a validated semi-automatic device for BP measuring at home.
Of the subjects enrolled in the original study, 70% consented to have the same measurements repeated 10 years later. Moreover, the numbers of fatal and nonfatal cardiovascular events (stroke, myocardial infarction and heart failure) were recorded during an average follow-up of 148 months.
This article is a review of the findings of the PAMELA Study on the clinical and prognostic significance of cardiac abnormalities such as left ventricular hypertrophy (LVH), left atrial dilatation (LA) and aortic root (AR) dilatation. These results will be discussed in detail in separate subsections.
Left ventricular hypertrophy
In the past several decades, observational and interventional studies have consistently demonstrated that LVH, assessed either by standard 12-lead ECG or ECHO, is a strong predictor of cardiovascular morbidity and mortality as well as of all-cause death in the general population and in specific settings, such as in patients with systemic hypertension, coronary heart disease, congestive heart failure and chronic renal failure.1, 2, 3, 4
Epidemiological and clinical evidence suggests that arterial hypertension is the major determinant of LVH. Hypertensive LVH is the result of interactions between BP and volume overload with genetic, ethnic, humoral and hormonal factors,5, 6, 7 thus leading to cardiomyocyte hypertrophy and interstitial fibrosis. Experimental studies have provided evidence that these alterations result from an imbalance between stimulatory (that is, angiotensin II, endothelin-1, catecholamines, aldosterone, basic fibroblast growth factor, insulin-like growth factor) and inhibitory factors (prostaglandins, nitric oxide, natriuretic peptides) regulating cardiomyocyte growth and myocardial collagen expression.8, 9 LVH development is a compensatory response to pressure overload and is aimed at counterbalancing heart wall stress in the early phases of essential hypertension. In the subsequent phases, experimental and human studies have indicated that this condition is related to unfavorable cardiac effects such as increased myocardial stiffness leading to diastolic dysfunction, reduced coronary reserve, atrial/ventricular arrhythmias and ultimately systolic dysfunction, the pathophysiologic substrate carrying a high risk for cardiovascular events.10
Detection of LVH can be performed by several diagnostic methods characterized by different sensitivity and specificity, namely, ECG, chest X-ray, ECHO or MRI. Standard ECG at rest is a simple, low-cost technique that is widely available in clinical practice. ECHO is the most widely used noninvasive imaging procedure for evaluation of cardiac anatomy and function in hypertensive patients. The ECG and ECHO findings provided by the PAMELA studies will be discussed separately.
ECG-LVH
During the past half-century, substantial data have accumulated supporting the prognostic value of ECG criteria for LVH in population-based samples. These findings primarily have come from populations at high cardiovascular risk characterized by an elevated prevalence of ECG alterations (LVH and strain), cardiovascular disease or multiple risk factors. The role of ECG-LVH in predicting cardiovascular prognosis in populations at lower cardiovascular risk than those included in the previous studies are poorly defined. Therefore, we evaluated the values of three established ECG voltage criteria (Sokolow-Lyon index: ⩾3.5 mV, Cornell voltage: aVL >2.0 mV in women and >2.8 mV in men and RaVL voltage: >0.7 mV) to detect anatomical LVH, by using echocardiographic LV mass (LVM) index as reference, and to predict incident cardiovascular events and all-cause mortality in 1549 PAMELA participants.11 The prevalence of ECG-LVH was lowest (0.9%) in the Sokolow-Lyon index, intermediate (7.7%) in the Cornell voltage and highest (12.7%) in the RaVL wave voltage. The Cornell voltage showed the best diagnostic performance for the detection of ECHO-LVH and was the only ECG criterion associated with an increased risk of cardiovascular events and all-cause mortality after adjustment for age, sex and average 24-h ambulatory BP. In a practical perspective, our observations indicate that (1) the three examined ECG-LVH criteria have a different power in cardiovascular risk stratification and (2) the Cornell voltage index is more effective than the time-honored Sokolow-Lyon in improving cardiovascular risk stratification.
The diagnostic sensitivity of old and newer ECG-LVH criteria is limited, as documented by studies simultaneously estimating LVM by ECHO and, less frequently, by computerized tomography or magnetic resonance. In particular, obesity markedly impairs the accuracy of ECG-LVH criteria because of the attenuating effects of chest wall and epicardial fat on QRS amplitudes; normalization of ECG criteria to body mass index (BMI) has been proposed to increase the diagnostic sensitivity of LVH. Thus, in the PAMELA population, we tested whether adjusting ECG-LVH criteria to BMI improved the accuracy in detecting anatomical ECHO-LVH and, more importantly, in predicting incident cardiovascular events.12 Our results showed that correction for BMI ameliorated the diagnostic accuracy of the Cornell voltage criterion in detecting ECHO-LVH. In particular, the adjusted risk of cardiovascular events related to a 1s.d. increment of the BMI-corrected Cornell voltage significantly outperformed in the obese participants; however, this was not the case in the total population, in which the performance of the corrected and uncorrected criterion was similar. Thus, normalization of ECG criteria to BMI has a relevant value in obese individuals; this value remains to be evaluated in populations with a higher prevalence of obesity than that in the PAMELA population.
ECHO- LVH
The PAMELA Study provided a number of relevant findings concerning the prevalence, clinical correlates, diagnostic criteria and prognostic value of LVH. In this section, we will focus on the following issues: (1) LVH diagnostic criteria, (2) the relationship between in- and out-of-office BPs with LVH and (3) the prognostic value of LVH and abnormal LV geometric patterns. Normal values of LVM in our study were defined in a selected sample of healthy true normotensive individuals. After excluding conditions known to affect LVM, such as obesity and type 2 diabetes mellitus, normotension was defined not only by clinical BP measurement but also by home and ambulatory BP criteria. Thus, in this study, in contrast to previous studies, subjects with masked hypertension were not included in the normal BP fraction of the population.13 The upper limits of LVM in our study sample were similar (114 g m−2 in men and 99 g m−2 in women) to those subsequently adopted by 2013 ESH/ESC (European Society of Hypertension/European Society of Cardiology) guidelines on hypertension (115/95 g m−2) that have replaced the 2007 criteria (125/110 g m−2; Table 2).
The prevalence and clinical significance of isolated office-measured (or white coat) hypertension and the opposite condition (that is, masked hypertension) is controversial. We studied the prevalence of both conditions and their association with LVH in the untreated fraction of the PAMELA population.14 In subjects with isolated office hypertension (∼10% of the sample), the LVM index and LV heart wall thickness were, on average, lower than those in subjects with both office and ambulatory or home hypertension but greater than those in subjects with true normotension. This finding was also the case when data were separately analyzed by sex and adjusted for age. Of note, the extent of subclinical cardiac damage (average LVM index, LV heart wall thickness and prevalence of LVH) in subjects with masked hypertension (10%) was similar to those of subjects with isolated hypertension and was greater than those in normotensive participants. Overall, these findings indicate that masked and isolated hypertension involving a consistent fraction of the general population represent a considerable risk factor for LVH.
The relationship between circadian BP variations and night-time BP levels with LVH has been investigated by cross-sectional studies in different settings, including population-based samples. Our study was, to our knowledge, the first to prospectively examine the value of such ambulatory BP parameters in predicting new-onset LVH in a population study.15 A total of 243 subjects with a baseline normal LVM index developed LVH 10 years later; these subjects were older and more obese and had higher office and ambulatory BP values than those of subjects with persistently normal LVM. After adjustment for age, sex and baseline LVM, the mean BP and the lowest systolic BP value at night were identified as independent risk factors for LVH development; this finding was not the case for absolute and percent nocturnal BP fall. Thus, night-time BP levels, rather than the magnitude of nocturnal BP decline, may be regarded as a reliable ambulatory BP parameter for predicting the progression to LVH.
In the PAMELA population, the value of LVH in stratifying the risk of cardiovascular morbidity and mortality, as well as the risk of all-cause death, was assessed during a long-term follow-up (average 148 months).16 The risk of cardiovascular events and total mortality was significantly greater in patients with LVH than in their counterparts (hazard ratio (HR) 1.65, 95% confidence interval (CI) 1.10–2.49, P=0.02; HR 1.49, 95% CI 1.02–2.18, P=0.04, respectively). In LVH participants, the increased risk remained significant even after the data were adjusted for several confounding factors, including home BP, 24 h mean BP and office BP. A 10% increase in LVM index was associated with a clearly increased risk in cardiovascular morbidity/mortality or all-cause deaths. In multivariate analysis, LVMI was an independent predictor of cardiovascular events and death for any cause. This study provides the first demonstration that LVH also remains a major risk factor when the contribution of different BPs (office, home and ambulatory) is fully taken into account. This result was independent of methods used to normalize LVM to body size (that is, body surface area (BSA) or height).
In this respect, the most reliable method for scaling LVM to body size remains a matter of debate. Indexation to BSA is more commonly applied in clinical practice; this approach, however, has been questioned because (1) the three-dimensional variable LVM is divided by the two-dimensional variable BSA and (2) indexation to BSA tends to underestimate the LVH prevalence in the obese population. Alternatively, LVM normalization to body height or to height to the power of different allometric exponents (that is, 2.7–1.9–1.7) has been proposed. In 1716 PAMELA participants, we estimated the risk of cardiovascular and all-cause mortality associated with LVH, as assessed by LVM normalized to different indexes (BSA, height, height2.7, height1.7).17 We found that LVH, as defined according to four sex-specific criteria derived from the healthy fraction of the PAMELA population, entailed an increased risk of cardiovascular mortality and all-cause death independently of the indexation method regarding body size. Similar results have been obtained when the LVM index was treated as a continuous instead of a dichotomous variable. Together, our results indicate that indexation of LVM to BSA, in line with recommendations provided by the 2013 ESH/ESC guidelines, may reliably estimate cardiovascular risk related to LVH in populations with characteristics similar to those of the PAMELA cohort.
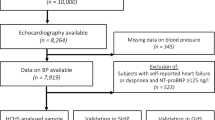
A further relevant issue addressed by the PAMELA Study relies on the prognostic significance of LVH subtypes (Figure 1). Whether abnormal LV geometric patterns (that is, LV concentric remodeling, eccentric and concentric LVH) provide different prognostic information is uncertain.18 Recently, investigators in the Dallas Heart Study have suggested a new LVH classification based on the following four subtypes: eccentric nondilated and dilated LVH, and concentric nondilated and dilated LVH.19 In the PAMELA population, we evaluated the risk of cardiovascular and all-cause mortality associated with abnormal LV geometric patterns, as defined by this new classification.20

Cardiovascular mortality survival rates in the population study, divided according to echocardiographic geometric patterns of the left ventricle (LV). LVH, left ventricular hypertrophy. A full color version of this figure is available at the Hypertension Research journal online.
Compared with normal LV geometry, concentric LVH (represented by nondilated LVH), eccentric dilated LVH and eccentric nondilated LVH, in that order, predicted the risk of cardiovascular mortality after adjustment for baseline covariates, including ambulatory BP. Similar findings were observed for all-cause mortality. Only concentric LVH, maintained a significant prognostic value for both outcomes after adjustment for baseline values of the LVM index. Thus, the new classification of LV geometric patterns tends to improve the risk stratification for all-cause and cardiovascular mortality; graduation of risk, however, is strongly dependent on LVM levels, and only concentric LVH provides prognostic information beyond the estimated cardiac mass.
Left atrial enlargement
LAE is an established marker of LV pressure and/or volume overload.21, 22 LA size, routinely assessed by echocardiography, is increased in several cardiac diseases such as coronary artery disease, dilated and hypertrophic cardiomyopathies, mitral or aortic valve diseases as well as systemic hypertension; all these conditions are associated with alterations in LV structure and function of various degrees.
Hypertensive heart disease is characterized by chronically elevated LV filling pressure and diastolic dysfunction; in this condition, the increase in LA size is the response to impaired LV compliance and LV diastolic dysfunction in the hypertrophic ventricle.23 It has been reported that LAE may already be present before LVH is manifested. Tsioufis et al.24 have shown that in newly diagnosed essential hypertensive subjects without LVH, LA volume is directly related to office and ambulatory BP and to brain natriuretic peptide and LV mass index. The association between circulating levels of brain natriuretic peptide, an index of myocardial stress/dysfunction, and LA size has also been documented in patients with heart failure of different etiologies with and without preserved LV systolic function.25 Despite growing evidence that LA size is a relevant cardiac phenotype for cardiovascular risk stratification, a limited number of studies have analyzed LAE prevalence and its demographic and clinical correlates in large population-based studies. In a random-sample of 2042 residents of Olmsted County, Minnesota, USA, who were aged ⩾45 years, the LAE prevalence, identified according to the partition values of LA volume indexed to BSA derived from a healthy reference group, was 16%.26 In the MONIKA/KORA study, a population-based survey including 1212 individuals aged 25-74 years, LAE diagnosed according to criteria based on LA volume indexed to height was found to be enlarged in 9.6% of men and 10% of women.27
In small-scale cross-sectional investigations, a higher risk of LAE has been associated with type 2 diabetes, obesity, metabolic syndrome, sleep apnea, hypertension, aging, chronic kidney disease, ECG- and ECHO-LVH and LV systolic and diastolic dysfunction.28, 29
The prognostic significance of LA size has been investigated in longitudinal studies in both Caucasian and ethnically mixed populations. These reports have shown that LAE is among the strongest risk factors for atrial fibrillation30 and ischemic stroke, independently of concomitant LVH.31, 32 Moreover, LA size has been found to be a strong predictor of death and heart failure hospitalization in patients with myocardial infarction and reduced LV ejection fraction.33, 34 Whether abnormalities in LA structure may revert and lead to an improvement in cardiovascular prognosis, as LVH regression does, is less clear. In the Losartan Intervention for Endpoint Reduction in Hypertension Trial (LIFE), a reduction in LA diameter during follow-up has been found to be related to LVH regression and to a lower incidence of new-onset atrial fibrillation or mitral regurgitation.35
Because hypertension is the major modifiable risk factor for LAE, a number of echocardiographic studies have addressed the relationship between LA size and BP status. To provide comprehensive information on this topic, we performed a meta-analysis focusing on LAE prevalence in hypertension.36 A total of 15 studies published from January 2000 to July 2012, including 10 141 untreated and treated subjects (mean age range 46–72 years, 54% men), were considered. Approximately 90% of the pooled population was Caucasian; the overall prevalence of type 2 diabetes mellitus (14 studies, 9977 patients) was 7.6%; a marginal fraction of patients (n=385 patients, 3.8%) had previous cardiovascular events.
LAE was defined according to 11 different criteria based on two echocardiographic parameters (that is, anteroposterior diameter and LA volume); its prevalence consistently varied among studies, from 16 to 83%, with an average prevalence of 32% in the pooled population. According to a sex-based analysis of 9 out of 15 studies (8588 patients), the LAE prevalence was similar in women as in men, although this finding should be taken with caution because of the heterogeneity of diagnostic criteria (sex and non-sex specific) used to define LAE in the studies. Notably, Aurigemma et al.37 have examined 230 healthy elderly participants in the Cardiovascular Health Study and have observed that in aging women, LA tends to increase in the supero-inferior diameter, whereas in aging men, LA shape tends to become more spherical. Thus, in elderly male populations, LA volume rather than LA diameter should provide a better estimate of the prevalence and severity of LA size changes. Finally, data from 10 out of 15 studies (n=9,354 patients) indicate that LVH prevalence is significantly higher in patients with LAE (68%) than in those without LAE (42%). Owing to the intrinsic limitations of the meta-analytic method, our literature review did not address important aspects such as the clinical correlates of LAE. In this regard, two recent analyses of the PAMELA database38, 39 have provided interesting new findings on the prognostic implications of LA size and factors influencing long-term changes of LA diameter. In the first paper,38 we have found that LA diameter in the overall PAMELA population is normally distributed, as are most biological parameters; thus, only arbitrary thresholds can separate abnormal from normal values. The LA diameter showed a direct relationship with demographic factors (age and male sex), as well as with office and out-of-office BP, metabolic indexes such as BMI, total cholesterol, triglycerides, fasting glucose and the LVM index. Increased LA dimensions, therefore, occur concomitantly with an array of abnormalities associated with cardiovascular risk. In the entire population, the LAE prevalence at the baseline observation varied from 5% (LA diameter indexed to BSA) to 10% (non-indexed LA diameter); these figures indicate that LAE is not a rare condition in a general population sample. Notably, these findings refer to a middle-aged population, with an average age of 47 years. Further qualifying information from our analysis is that the LA diameter predicted the incidence of nonfatal and fatal cardiovascular events over a 12-year observation period, independently of several cardiovascular risk factors. This finding confirms previous observations on the adverse prognostic importance of LA dimension and extends the conclusion to a longer follow-up period compared with previous longitudinal studies. Interestingly, the cardiovascular risk indicated by the LAE presence in subjects without LVH was superimposable with that indicated by LVH alone in subjects without LAE. This finding suggests that isolated alterations of LA structure are as prognostically important as isolated alterations of LV structure.
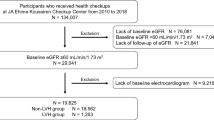
Available information on the extent of LA dimension changes over time and their correlates in the general population is limited to a number of North American prospective studies. Our report on this issue39 included 1045 subjects with normal LA at the baseline evaluation and a readable echocardiogram at the end of the follow-up. Over a 10-year period, a substantial fraction of participants (12%) progressed to LAE; these subjects were older and exhibited higher entry office, home and ambulatory systolic and diastolic BP values as well as higher fasting blood glucose and serum cholesterol compared with subjects who did not develop LAE. The incidence of new-onset LAE significantly increased from the lowest to the highest tertile of baseline office, home and 24-h BP, as well as the BMI, fasting blood glucose and LVM index. In a multivariate analysis, the baseline LA diameter, female sex, office systolic BP, BMI and LVM index emerged as key correlates of new-onset LAE (Figure 2). Interestingly, the LA diameter increased to a similar extent from the lowest to the highest BP tertile irrespective of whether office, home or 24 h mean values were considered.

Incidence of new-onset left atrium enlargement (LAE) in tertiles of body mass index (BMI), waist circumference (WC) and serum glucose. *P<0.05 between tertiles.
Together, our findings support the following conclusions: (1) LAE is a powerful integrated marker of cardiovascular risk, (2) LAE has a similar prognostic value as LVH and (3) maintenance of BP, BMI and LVM within normal levels during adult life may contribute to preventing LAE and its adverse complications. In a practical perspective, assessment of LA dimensions (diameter and/or volume) should be recommended during routine ECHO examination to improve cardiovascular risk stratification in the general population.
Aortic root dilatation
The AR is the most proximal portion of the systemic arterial tree. It is a complex structure extending from the basal attachment of the aortic valve cusps within the LV outflow tract to the distal attachment at the tubular tract of the aorta (the so-called sinotubular junction), including Valsalva sinuses.
Accumulating evidence indicates that AR dilatation in the general population and in hypertensive cohorts may be regarded as a target organ damage that parallels other subclinical markers of established prognostic values such as LVH, carotid atherosclerosis, retinal alterations and microalbuminuria.40, 41, 42 More importantly, emerging data, including those recently provided by the PAMELA Study, suggest that AR dilatation is an independent predictor of cardiovascular morbidity and mortality.
The risk of life-threatening vascular complications such as thoracic aorta dissection and rupture has been reported to be strictly related to AR and ascending aorta diameter.43 Systemic hypertension tends to increase aortic wall stress and is a major modifiable risk factor for the development of thoracic aorta aneurysms.44 In addition, systemic and local growth factors involved in cardiac remodeling also play a role in AR dilatation in the hypertensive setting.
The relative contribution of BP in AR dilatation, however, in both normotensive and hypertensive subjects, appears to be substantially lower than that of other factors such as age, sex and anthropometric variables, including height, weight and their derivatives, BSA and BMI.45, 46 The crucial influence of age on aorta dimensions is related to the progressive thinning and fragmentation of elastic fibers during the aging process combined with the effects of chronic cyclic stress. Furthermore, recent evidence indicates that AR dilatation is independently associated with abdominal obesity, metabolic syndrome and inflammatory markers (for example, C-reactive protein), thus supporting a role of metabolic and low-grade inflammatory factors in the pathogenesis of large artery alterations.47
AR dilatation has been shown to occur more frequently in hypertensive than in normotensives individuals,48 and an association between AR size and LVH has been reported in hypertensive patients. Studies evaluating the hemodynamic and nonhemodynamic determinants of AR size, however, have yielded inconsistent results.49, 50 In a cross-sectional analysis of subjects enrolled in the Hypertension Genetic Study, the prevalence of AR dilatation was similar between 2096 hypertensives and 361 normotensives (∼4%), and AR adjusted for BSA was nonsignificantly higher in the hypertensive group.51
The prevalence of AR dilatation depends on the clinical characteristics of the subjects under investigation as well as on the criteria defining this phenotype. In this respect, normal reference values and methods for normalizing aortic diameter to body size remain a matter of debate; AR diameter normalized to BSA has been indicated to be a reliable parameter accounting for differences in body size. This approach, however, has the major limitation of relying on the geometric difference between the linear dimension of aortic root diameter and the quadratic dimension of BSA. Alternatively, indexation to height has been recommended by ECHO guidelines.
The prevalence of AR dilatation has been found to be higher in selected hypertensive populations with ECG- or ECHO-LVH than in unselected hypertensive cohorts. In a LIFE substudy, Bella et al.40 have found that 10% of 947 patients with moderate and severe hypertension and ECG-LVH fulfilled diagnostic criteria for AR dilatation. A similar figure (10.5%) has been reported by Cipolli et al.47 in 438 hypertensives with ECHO-LVH (that is, LV mass index >51 g height−2.7). Among 3366 untreated and treated essential hypertensives (mean age 53±12 years) consecutively attending an out-patient hypertension clinic, we have found that AR dilatation was present in 6% of the sample.41
A recent meta-analysis of 8 studies including 10 791 hypertensive subjects has shown that the prevalence of AR dilatation in the pooled population was 9.1%, and the prevalence in men was nearly 3 times higher than that in women (12.7% and 4.5%, respectively).52 A significant difference in AR prevalence was evident among studies (3.7–16.7%), primarily because of heterogeneity in the clinical characteristics of enrolled patients and, to a lesser extent, differences in diagnostic criteria of AR dilatation. Notably, hypertensive subjects with AR dilatation compared with those with normal AR size had similar office systolic and diastolic BP values, but they were older (+4 years) and had higher LVM index values.
The value of the AR diameter in predicting cardiovascular outcomes in the absence of aneurysmatic alterations remains incompletely elucidated. Before this topic was addressed in the PAMELA population, available information was limited to two prospective studies performed in North American population-based samples. The Cardiovascular Health Study has demonstrated that the AR diameter at baseline is associated with an increased risk of incident stroke and cardiovascular mortality (HRs 1.3 and 1.6, respectively, for each 1 cm increase of AR diameter) over a 10-year follow-up.53 Among the 6483 middle-aged and older adults followed in the Framingham Heart Study over a 8-year period, the risk of incident heart failure increased with AR diameter values at baseline (HR 1.19 for a 1 s.d. increase, 95% CI 1.04–1.38).54 After adjustment for LVM as well as for traditional risk factors, the association of baseline AR diameter with incident heart failure lost the statistical significance.
The new piece of information added by the PAMELA Study55 on the clinical and prognostic significance of AR diameter can be summarized as follows. First, AR dilatation defined by sex-specific cutoffs indexed to body size measures tended to be more prevalent in men than in women (5.9% vs. 5.2% for AR diameter indexed to BSA and 10.1% vs. 9.1% for AR diameter indexed to height, respectively). Second, age, LVM/BSA, male sex and 24 h systolic BP/diastolic BP in a multiple regression analysis were the most important predictors of AR diameter normalized to height. Our data provide the first indication of the role of out-of-office BP in AR remodeling. This result is relevant, given that the effect of ambulatory BP on AR diameter has not previously been prospectively investigated in large population studies. Third, after adjustment for several covariates (age, sex, BP, fasting blood glucose, total cholesterol, smoking status, previous cardiovascular disease and use of antihypertensive drugs), the AR diameter indexed to height emerged as a significant predictor of incident cardiovascular morbidity and mortality (HR 2.62 for every 1 unit increase, 95% CI 1.19–5.75, P=0.01). Fourth, when participants were classified according to the presence/absence of LVH and AR dilatation, the fully adjusted risk of cardiovascular events was markedly greater in subjects with concomitant LVH and aortic dilatation than in their counterparts with LVH alone. Thus, the overall risk is significantly increased when parallel changes occur in LV structure and aortic dimension compared with isolated alterations of LV structure. Together, these results showed that the assessment of AR diameter contributes to refining the prognostic assessment and preventive strategies in the general population. This biomarker is a reliable predictor of adverse cardiovascular prognosis, and AR dilation associated with LVH represents a high-risk condition.
Conclusions
Abnormalities in the LV structure/geometry and LA and AR size are common at the community level. Findings from the PAMELA population indicate that unhealthful risk factors such as elevated office and out-of-office BP, metabolic alterations and overweight/obesity are the most important modifiable determinants of the development and progression of such markers of target organ damage, and they are clearly predictive of increased long-term incidence of cardiovascular outcomes. From a clinical perspective, the search for cardiac organ damage is an important means to improve cardiovascular risk stratification and, more importantly, to prevent cardiovascular morbidity and mortality in the general population.
References
Kannel WB, Gordon T, Offut D . Left ventricular hypertrophy by electrocardiogram. Prevalence, incidence, and mortality in the Framingham Study. Ann Intern Med 1969; 71: 89–105.
Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP . Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart study. N Engl J Med 1990; 322: 1561–1566.
Vakili BA, Okin PM, Devereux RB . Prognostic implications of left ventricular hypertrophy. Am Heart J 2001; 141: 334–341.
Verdecchia P, Porcellati C, Reboldi G, Gattobigio R, Borgioni C, Pearson TA, Ambrosio G . Left ventricular hypertrophy as an independent predictor of acute cerebrovascular events in essential hypertension. Circulation 2001; 104: 2039–2044.
Kotsis V, Stabouli S, Toumanidis S, Tsivgoulis G, Rizos Z, Trakateli C, Zakopoulos N, Sion M . Obesity and pulse pressure are predictors of left ventricular hypertrophy in true normotensives. J Hypertens 2010; 28: 1065–1073.
Poppe KK, Edgerton Bachmann M, Triggs CM, Doughty NN, Whalley GA . Geographic variations in left ventricular mass and left ventricular mass index: a systematic review. J Hum Hypertens 2012; 26: 420–429.
Catena C, Colussi GL, Valeri M, Sechi LA . Association of aldosterone with left ventricular mass: interaction with plasma fibrinogen levels. Am J Hypertens 2012; 26: 111–117.
Olivetti G, Melissari M, Balbi T, Quaini F, Cigola E, Sonnenblick EH, Anversa P . Myocyte cellular hypertrophy is responsible for ventricular remodelling in the hypertrophic heart of middle-aged individuals in the absence of heart failure. Cardiovasc Res 1994; 28: 1199–1208.
Gonzalez A, Lopez B, Diez J . Fibrosis in hypertensive heart disease role of the angiotensin-aldosterone system. Med Clin N Am 2004; 88: 83–97.
Ruilope LM, Schmieder RE . Left ventricular hypertrophy and clinical outcomes in hypertensive patients. Am J Hypertens 2008; 21: 500–506.
Cuspidi C, Facchetti R, Bombelli M, Sala C, Grassi G, Mancia G . Accuracy and prognostic value of electrocardiographic markers of left ventricular hypertrophy in a general population: findings from the Pressioni Arteriose Monitorate e Loro Associazioni population. J Hypertens 2014; 32: 921–928.
Cuspidi C, Facchetti R, Bombelli M, Sala C, Tadic M, Grassi G, Mancia G, Does QRS . Voltage correction by body mass index improve the accuracy of electrocardiography in detecting left ventricular hypertrophy and predicting cardiovascular events in a general population? J Clin Hypertens 2016; 18: 415–421.
Cuspidi C, Facchetti R, Sala C, Bombelli M, Negri F, Carugo S, Grassi G, Mancia G . Normal values of left ventricular mass: findings from the PAMELA study. J Hypertens 2012; 30: 997–1003.
Sega R, Trocino G, Lanzarotti A, Carugo S, Cesana G, Schiavina R, Bombelli M, Giannattasio C, Zanchetti A, Mancia G . Alterations of cardiac structure in patients with isolated office, ambulatory, or home hypertension: data from the general population (Pressioni Arteriose Monitorate E Loro Associazioni [PAMELA] Study). Circulation 2001; 104: 1385–1392.
Cuspidi C, Facchetti R, Bombelli M, Sala C, Negri F, Grassi G, Mancia G . Nighttime blood pressure and new-onset left ventricular hypertrophy: findings from the Pamela population. Hypertension 2013; 62: 78–84.
Bombelli M, Facchetti R, Carugo S, Madotto F, Arenare F, Quarti-Trevano F, Capra A, Giannattasio C, Dell’Oro R, Grassi G, Sega R, Mancia G . Left ventricular hypertrophy increases cardiovascular risk independently of in-office and out-of-office blood pressure values. J Hypertens 2009; 27: 2458–2464.
Cuspidi C, Facchetti R, Bombelli M, Sala C, Tadic M, Grassi G, Mancia G . Prognostic value of left ventricular mass normalized to different body size indexes: findings from the PAMELA population. J Hypertens 2015; 33: 1082–1089.
Lavie CJ, Milani RV, Shah SB, Gilliland YE, Bernal JA, Dinshaw H, Ventura HO . Impact of left ventricular geometry on prognosis- a review of Ochsner studies. Ochsner J 2008; 8: 11–17.
Khouri MG, Peshock RM, Ayers CR, de Lemos JA, Drazner MH . A 4-tiered classification of left ventricular hypertrophy based on left ventricular geometry: the Dallas Heart Study. Circ Cardiovasc Imaging 2010; 3: 164–171.
Cuspidi C, Facchetti R, Bombelli M, Sala C, Tadic M, Grassi G, Mancia G . Risk of mortality in relation to an updated classification of left ventricular geometric abnormalities in a general population: the Pamela study. J Hypertens 2015; 33: 2133–2140.
Raman SV . The hypertensive heart. An integrated understanding informed by imaging. J Am Coll Cardiol 2010; 55: 91–96.
Douglas P . The left atrium. A biomarker of chronic diastolic dysfunction and cardiovascular disease risk. J Am Coll Cardiol 2003; 42: 1206–1207.
Milan A, Puglisi E, Magnino C, Naso D, Abram S, Avenatti E, Rabbia F, Mulatero P, Veglio F . Left atrial enlargement in essential hypertension: role in the assessment of subclinical hypertensive heart disease. Blood Press 2012; 21: 88–96.
Tsioufis C, Stougiannos P, Taxiarchou E, Skiadas I, Chatzis D, Thomopoulos C, Lalos S, Stefanadis C, Kallikazaros I . The interplay between hemodynamic load, brain natriuretic peptide and left atrial size in the early stages of essential hypertension. J Hypertens 2006; 24: 965–972.
Kim H, Jun DW, Cho YK, Nam CW, Han SW, Hur SH, Kim YN, Kim KB . The correlation of left atrial volume index to the level of N-terminal pro-BNP in heart failure with preserved ejection fraction. Echocardiography 2008; 25: 961–967.
Pritchett AM, Jacobsen SJ, Mahoney DW, Rodeheffer RJ, Bailey KR, Redfield MM . Left atrial volume as an index of left atrial size: a population-based study. J Am Coll Cardiol 2003; 41: 1036–1043.
Stritzke J, Markus MR, Duderstadt S, Lieb W, Luchner A, Doring A, Keil U, Hense HW, Schunkert H . MONICA/KORA Investigators. The aging process of the heart: obesity is the main risk factor for the left atrial enlargement during aging the MONICA/KORA (monitoring of trends and determinations in cardiovascular disease/cooperative research in the region of Augsburg) study. J Am Coll Cardiol 2009; 17: 1982–1989.
Cipollini F, Arcangeli E, Seghieri G . Left atrial dimension is related to blood pressure variability in newly diagnosed untreated hypertensive patients. Hypertens Res 2016; 39: 583–587.
Fang NN, Sui DX, Yu JG, Gong HP, Zhong M, Zhang Y, Zhang W . Strain/strain rate imaging of impaired left atrial function in patients with metabolic syndrome. Hypertens Res 2015; 38: 758–764.
Vaziri S, Larson M, Benjamin EJ, Levy D . Echocardiographic predictors of non-rheumatic atrial fibrillation. The Framingham Heart Study. Circulation 1994; 89: 724–730.
Benjamin EJ, D’Agostino RB, Belanger AJ, Wolf PA, Levy D . Left atrial size and the risk of stroke and death: the Framingham Heart Study. Circulation 1995; 92: 835–841.
Di Tullio MR, Sacco RL, Sciacca RR, Homma S . Left atrial size and the risk of ischemic stroke in an ethnically mixed population. Stroke 1999; 30: 2019–2024.
Moller JE, Hillis GS, On JK, Seward JB, Reeder GS, Wright RS, Park SW, Bailey KR, Pellikka PA . Left atrial volume. A powerful predictor of survival after acute myocardial infarction. Circulation 2003; 107: 2207–2212.
Meris A, Amigoni M, Uno H, Thune JJ, Verma A, Kober L, McMurray JJ, Velazquez EJ, Maggioni AP, Ghali J, Arnold JM, Zelenkofske S, Pfeffer MA, Solomon SD . Left atrial remodelling in patients with myocardial infarction complicated by heart failure, ventricular dysfunction or both: the VALIANT Echo study. Eur Heart J 2009; 30: 56–65.
Gerdts E, Wachtell K, Omvik P, Otterstad JE, Oikarinen L, Boman K, Dahlöf B, Devereux RB . Left atrial size and risk of major cardiovascular events during antihypertensive treatment. Losartan Intervention for Endpoint Reduction in Hypertension Trial. Hypertension 2007; 49: 311–316.
Cuspidi C, Rescaldani M, Sala C . Prevalence of echocardiographic left-atrial enlargement in hypertension: a systematic review of recent clinical studies. Am J Hypertens 2013; 26: 456–464.
Aurigemma GP, Gottdiener JS, Arnold AM, Chinali M, Hill JC, Kitzman D . Left atrial volume and geometry in healthy aging. The Cardiovascular Health Study. Circ Cardiovasc Imaging 2009; 2: 282–289.
Bombelli M, Facchetti R, Cuspidi C, Villa P, Dozio D, Brambilla G, Grassi G, Mancia G . Prognostic significance of left atrial enlargement in a general population: results of the PAMELA study. Hypertension 2014; 64: 1205–1211.
Bombelli M, Cuspidi C, Facchetti R, Sala C, Tadic M, Brambilla G, Re A, Villa P, Grassi G, Mancia G . New-onset left atrial enlargement in a general population. J Hypertens 2016; 34: 1838–1845.
Bella JN, Wachtell K, Boman K, Palmieri V, Papademetriou V, Gerdts E, Aalto T, Olsen MH, Olofsson M, Dahlöf B, Roman MJ, Devereux RB . Relation of left ventricular geometry and function to aortic root dilatation in patients with systemic hypertension and left ventricular hypertrophy (the LIFE study). Am J Cardiol 2002; 89: 337–341.
Cuspidi C, Meani S, Fusi V, Valerio C, Sala C, Zanchetti A . Prevalence and correlates of aortic root dilatation in patients with essential hypertension: relationship with cardiac and extra-cardiac organ damage. J Hypertens 2006; 24: 573–580.
Rosenbaum D, Kachenoura N, Koch E, Paques M, Cluzel P, Redheuil A, Girerd X . Relationships between retinal arteriole anatomy and aortic geometry and function and peripheral resistance in hypertensives. Hypertens Res 2016; 39: 536–542.
Shirali AS, Bischoff MS, Lin HM, Oife I, Lookstein R, Griepp RB, Di Luozzo G . Predicting the risk for acute type B aortic dissection in hypertensive patients using anatomic variables. JACC Cardiovasc Imaging 2013; 36: 349–357.
Pape LA, Tsai TT, Isselbacher EM, Oh JK, O'Gara PT, Evangelista A, Fattori R, Meinhardt G, Trimarchi S, Bossone E, Suzuki T, Cooper JV, Froehlich JB, Nienaber CA, Eagle KA . International Registry of Acute Aortic Dissection I. Aortic diameter >or=5.5 cm is not a good predictor of type a aortic dissection: Observations from the international registry of acute aortic dissection (IRAD). Circulation 2007; 116: 1120–1127.
Lam CS, Xanthakis V, Sullivan ML, Lieb W, Aragam J, Redfield MM, Mitchell GF, Benjamin EJ, Vasan RS . Aortic root remodeling over the adult life course. Longitudinal data from the Framingham Heart Study. Circulation 2010; 122: 884–890.
Vasan RS, Larson MG, Levy D . Determinants of echocardiographic aortic root size. Circulation 1995; 91: 734–740.
Cipolli JA, Souza FAS, Ferreira-Sae MCS, Magalhaes JAP, Figueiredo ES, Vidotti VG, Matos-Souza JR, Franchini KG, Nadruz W . Sex-specific hemodynamic and non-hemodynamic determinants of aortic root size in hypertensive subjects with left ventricular hypertrophy. Hypertens Res 2009; 32: 956–961.
Kim M, Roman MJ, Cavallini MC, Schwartz JE, Pickering TG, Devereux RB . Effect of hypertension on aortic root size and prevalence of aortic regurgitation. Hypertension 1996; 28: 47–52.
Farasat SM, Morrell CH, Scuteri A, Ting CT, Yin FCP, Spurgeon HA, Chen CH, Lakatta EG, Najjar SS . Do hypertensive individuals have enlarged aortic root diameters? Insights from studying the various subtypes of hypertension. Am J Hypertens 2008; 21: 558–563.
de Simone G, Chinali M . Aortic root dimension and hypertension: a chicken-egg dilemma. Am J Hypertens 2008; 21: 489–490.
Palmieri V, Bella JN, Arnett DK, Roman MJ, Oberman A, Kitzman DW, Hopkins PN, Paranicas M, Rao DC, Devereux RB . Aortic root dilatation at sinuses of Valsalva and aortic regurgitation in hypertensive and normotensive subjects: the Hypertension Genetic Epidemiology Network Study. Hypertension 2001; 37: 1229–1235.
Covella M, Milan A, Totaro S, Cuspidi C, Re A, Rabbia F, Veglio F . Echocardiographic aortic root dilatation in hypertensive patients: a systematic review and meta-analysis. J Hypertens 2014; 32: 1928–1935.
Gardin JM, Arnold AM, Polak J, Jackson S, Smith V, Gottdiener J . Usefulness of aortic root dimension in persons>65 years of age in predicting heart failure, stroke, cardiovascular mortality, all-cause mortality and acute myocardial infarction (from the Cardiovascular Health Study). Am J Cardiol 2006; 97: 270–275.
Lam CSP, Gona P, Larson MG, Aragam J, Lee DS, Mitchell GF, Levy D, Cheng S, Benjamin EJ, Vasan RS . Aortic root remodeling and risk of heart failure in the Framingham Heart Study. JACC Heart Fail 2013; 1: 79–83.
Cuspidi C, Facchetti R, Bombelli M, Re A, Cairo M, Sala C, Tadic M, Grassi G, Mancia G . Aortic root diameter and risk of cardiovascular events in a general population: data from the PAMELA study. J Hypertens 2014; 32: 1879–1887.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Cuspidi, C., Sala, C., Casati, A. et al. Clinical and prognostic value of hypertensive cardiac damage in the PAMELA Study. Hypertens Res 40, 329–335 (2017). https://doi.org/10.1038/hr.2016.153
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2016.153
Keywords
This article is cited by
-
High blood pressure with elevated resting heart rate: a high risk “Sympathetic” clinical phenotype
Hypertension Research (2023)
-
Home sphygmomanometers can help in the control of blood pressure: a nationwide field survey
Hypertension Research (2018)
-
Higher plasma leptin levels are associated with reduced left ventricular mass and left ventricular diastolic stiffness in black women: insights from the Genetic Epidemiology Network of Arteriopathy (GENOA) study
Hypertension Research (2018)
-
Big Data and Blood Pressure Control: Insights from the PAMELA and BP-CARE Study Cohorts
Current Hypertension Reports (2018)
