
Abstract
Objective:
To compare the effect of early extubation to nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) on the need for mechanical ventilation via endotracheal tube (MVET) at 7 days of age in preterm infants <30 weeks’ gestation requiring intubation and surfactant for respiratory distress syndrome (RDS) within 60 min of delivery.
Study Design:
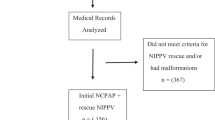
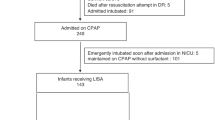
Multicenter, randomized, controlled trial. A total of 57 infants were randomized within 120 min of birth to NCPAP (BW 1099 g and GA 27.8 weeks) and 53 infants to NIPPV (BW 1052 g, and GA 27.8 weeks). Infants were stabilized on NCPAP at birth and were given poractant alfa combined with MVET within 60 min of age. When stabilized on MVET, they were extubated within the next hours or days to NCPAP or NIPPV.
Result:
A total of 40% of infants needed MVET at 7 days of age in the NCPAP group compared with 17% in the NIPPV group (OR: 3.6; 95% CI: 1.5, 8.7). Days on MVET were 12±11 days in NCPAP group compared with 7.5±12 days in the NIPPV group (median 1 vs 7 days; P=0.006). Clinical bronchopulmonary dysplasia (BPD) was 39% in the NCPAP group compared to 21% in the NIPPV group (OR: 2.4; 95% CI: 1.02, 5.6). Physiological BPD was 46% in the NCPAP group compared with 11% in the NIPPV group (OR: 6.6, 95% CI: 2.4, 17.8; P=0.001). There were no differences in any other outcomes between the two groups.
Conclusion:
NIPPV compared with NCPAP reduced the need for MVET in the first week, duration of MVET, and clinical as well as physiological BPD in preterm infants receiving early surfactant for RDS.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Bancalari E, del Moral T . Bronchopulmonary dysplasia and surfactant. Biol Neonate 2001; 80: 7–13.
Manktelow BN, Draper ES, Annamalai S, Field D . Factors affecting the incidence of chronic lung disease of prematurity in 1987, 1992, and 1997. Arch Dis Child Fetal Neonatal Ed 2001; 85: F33–F35.
Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC et al. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics 2010; 126: 443–456.
Speer CP . Inflammation and bronchopulmonary dysplasia: a continuing story. Semin Fetal Neonatal Med 2006; 11: 354–362.
Van Marter LJ, Allred EN, Pagano M, Sanocka U, Parad R, Moore M et al. Do clinical markers of barotrauma and oxygen toxicity explain inter-hospital variation in rates of chronic lung disease? Pediatrics 2000; 105: 1194–1201.
Vanpee M, WalfridssonSchultz U, KatzSalamon M, Zupancic JAF, Pursley D, Jonsson B . Resuscitation and ventilation strategies for extremely preterm infants: a comparison study between two neonatal centers in Boston and Stockholm. Acta Paediatr 2007; 96: 10–16.
Verder H, Albertsen P, Ebbesen F, Greisen G, Robertson B, Bertelsen A et al. Nasal continuous positive airway pressure and early surfactant therapy for respiratory distress syndrome in newborns of less than 30 weeks’ gestation. Pediatrics 1999; 103: E24.
Dani C, Bertini G, Pezzati M, Cecchi A, Caviglioli C, Rubaltelli FF . Early extubation and nasal continuous positive airway pressure after surfactant treatment for respiratory distress syndrome among preterm infants <30 weeks’ gestation. Pediatrics 2004; 113: e560–e563 .
Davis P, Davies M, Faber B . A randomised controlled trial of two methods of delivering nasal continuous positive airway pressure after extubation to infants weighing less than 1000 g: binasal (Hudson) versus single nasal prongs. Arch Dis Child Fetal Neonatal Ed 2001; 85: F82–F85.
Finer NN, Carlo WA, Duara S, Fanaroff AA, Donovan EF, Wright LL et al. Delivery room continuous positive airway pressure/positive end-expiratory pressure in extremely low birth weight infants: a feasibility trial. Pediatrics 2004; 114: 651–657.
Morley CJ, Davis PG, Doyle LW, Brion LP, Hascoet JM, Carlin JB . Nasal CPAP or intubation at birth for very preterm infants. N Engl J Med 2008; 358: 700–708.
Gupta S, Sinha SK, Tin W, Donn SM . A randomized controlled trial of post-extubation bubble continuous positive airway pressure versus Infant Flow Driver continuous positive airway pressure in preterm infants with respiratory distress syndrome. J Pediatr 2009; 154: 645–650.
Sandri F, Plavka R, Ancora G, Simeoni U, Stranak Z, Martinelli S et al. Prophylactic or early selective surfactant combined with nCPAP in very preterm infants. Pediatrics 2010; 125: e1402–e1e09.
Davis PG, Henderson-Smart DJ . Nasal continuous positive airway pressure immediately after extubation for preventing morbidity in preterm infants. Cochrane Database Syst Rev 2003; (2): CD000143. doi: 10.1002/14651858.
SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network. Early CPAP versus surfactant in extremely preterm infants. N Engl J Med 2010; 362: 1970–1979.
Stefanescu MB, Murphy WP, Hansell BJ, Fuloria M, Morgan TM, Aschner JL . A randomized, controlled trial comparing two different continuous positive airway pressure systems for the successful extubation of extremely low birth weight infants. Pediatrics 2003; 112: 1031–1038.
Davis PG, Lemyre B, De Paoli AG, Kirpalani H . Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for preterm neonates after extubation. Cochrane Database Syst Rev 2001; (3): CD003212. doi: 10.1002/14651858.
Friedlich P, Lecart C, Posen R, Ramicone E, Chan L, Ramanathan R . A randomized trial of nasopharyngeal-synchronized intermittent mandatory ventilation versus nasopharyngeal continuous positive airway pressure in very low birth weight infants after extubation. J Perinatol 1999; 19: 413–418.
Barrington KJ, Bull D, Finer NN . Randomized trial of nasal synchronized intermittent mandatory ventilation compared with continuous positive airway pressure after extubation of very low birth weight infants. Pediatrics 2001; 107: 638–641.
Khalaf MN, Brodsky N, Hurley J, Bhandari V . A prospective randomized, controlled trial comparing synchronized nasal intermittent positive pressure ventilation versus nasal continuous positive airway pressure as modes of extubation. Pediatrics 2001; 108: 13–17.
Kugelman A, Feferkorn I, Riskin A, Chistyakov I, Kaufman B, Bader D . Nasal intermittent mandatory ventilation versus nasal continuous positive airway pressure for respiratory distress syndrome: a randomized, controlled, prospective study. J Pediatr 2007; 150: 521–526.
Moretti C, Giannini L, Fassi C, Gizzi C, Papoff P, Colarizi P . Nasal flow-synchronized intermittent positive pressure ventilation to facilitate weaning in very low-birth weight infants: unmasked randomized controlled trial. Pediatr Int 2008; 50: 85–91.
Kulkarni A, Ehrenkranz RA, Bhandari V . Effect of introduction of synchronized nasal intermittent positive-pressure ventilation in a neonatal intensive care unit on bronchopulmonary dysplasia and growth in preterm infants. Am J Perinatol 2006; 23: 233–240.
Bhandari V, Finer NN, Ehrenkranz RA, Saha S, Das A, Walsh MC et al. Synchronized nasal intermittent positive-pressure ventilation and neonatal outcomes. Pediatrics 2009; 124: 517–526.
Bhandari V, Gavino RG, Nedrelow JH, Pallela P, Salvador A, Ehrenkranz RA et al. A randomized controlled trial of synchronized nasal intermittent positive pressure ventilation in RDS. J Perinatol 2007; 27: 697–703.
Kishore MSS, Dutta S, Kumar P . Early nasal intermittent positive pressure ventilation versus continuous positive airway pressure for respiratory distress syndrome. Acta Pædiatrica 2009; 98: 1412–1415.
Bisceglia M, Belcastro A, Poerio V, Raimondi F, Mesuraca L, Crugliano C et al. A comparison of nasal intermittent versus continuous positive pressure delivery for the treatment of moderate respiratory syndrome in preterm infants. Minerva Pediatr 2007; 59: 91–95.
Walsh MC, Yao Q, Gettner P, Hale E, Collins M, Hensman A et al. Impact of a physiologic definition on bronchopulmonary dysplasia rates. Pediatrics 2004; 114: 1305–1311.
Rojas MA, Lozano JM, Rojas MX, Laughon M, Bose CL, Rondon MA et al. Very early surfactant without mandatory ventilation in premature infants treated with early continuous positive airway pressure: a randomized, controlled trial. Pediatrics 2009; 123: 137–142.
Aghai ZH, Saslow JG, Nakhla T, Milcarek B, Hart J, Lawrysh-Plunkett R et al. Synchronized nasal intermittent positive pressure ventilation (SNIPPV) decreases work of breathing (WOB) in premature infants with respiratory distress syndrome (RDS) compared to nasal continuous positive airway pressure (NCPAP). Pediatr Pulmonol 2006; 41: 875–881.
Kiciman NM, Andreasson B, Bernstein G, Mannino FL, Rich W, Henderson C et al. Thoracoabdominal motion in newborns during ventilation delivered by endotracheal tube or nasal prongs. Pediatr Pulmonol 1998; 25: 175–181.
Meneses J, Bhandari V, Alves JG, Herrmann D . Noninvasive ventilation for respiratory distress syndrome: a randomized controlled trial. Pediatrics 2011; 127: 300–307.
Garland JS, Nelson DB, Rice T, Neu J . Increased risk of gastrointestinal perforations in neonates mechanically ventilated with either face mask or nasal prongs. Pediatrics 1985; 76: 406–410.
Schmidt B, Roberts RS, Davis P, Doyle LW, Barrington KJ, Ohlsson A et al. Caffeine therapy for apnea of prematurity. N Engl J Med 2006; 354: 2112–2121.
Acknowledgements
We acknowledge parents of our study subjects for their trust and participation, nursing and respiratory care practitioners, neonatal fellows and faculty, and the following study coordinators: Rosanna Erickson, NNP (CA), Richard Hernandez, RCP (CA), Mike McCoy, MS, ARNP (OK), Karen Corff, MS, ARNP (OK), Debra McAnn, MS, ARNP (OK), Brooke Burks, MS, ARNP (OK), Michelle Huynh, MS, ARNP (OK), Caitlin Thi, MS, ARNP (OK), Raja Nandyal, MD (OK), Venu Gottipati, MD (OK), Kathy Arnell, RNC (SD) and Delores Gilles, RN, BSN (GA); DSMB members: Dr Vinod Bhutani from Stanford University and Dr Philippe Friedlich from Children's Hospital Los Angeles; Independent Biostatistician Dr Fred Dorey from Children's Hospital Los Angeles (CA). Funding was provided through an unrestricted grant by Dey LP and Chiesi Farmaceutici, SpA. All data analysis and interpretation of the data were independent of the funding agencies. (ClinicalTrials.gov NCT00486850; Funded by Dey LP and Chiesi Farmaceutici, SpA). This study was supported by an unrestricted grant from Dey LP and Chiesi Farmaceutici, SpA.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Ramanathan, R., Sekar, K., Rasmussen, M. et al. Nasal intermittent positive pressure ventilation after surfactant treatment for respiratory distress syndrome in preterm infants <30 weeks’ gestation: a randomized, controlled trial. J Perinatol 32, 336–343 (2012). https://doi.org/10.1038/jp.2012.1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jp.2012.1
Keywords
This article is cited by
-
High-flow nasal cannula (HFNC) vs continuous positive airway pressure (CPAP) vs nasal intermittent positive pressure ventilation as primary respiratory support in infants of ≥ 32 weeks gestational age (GA): study protocol for a three-arm multi-center randomized controlled trial
Trials (2023)
-
Current Controversies and Advances in Non-invasive Respiratory Support for Preterm Infants
Current Treatment Options in Pediatrics (2022)
-
Reintubation rates after extubation to different non-invasive ventilation modes in preterm infants
BMC Pediatrics (2021)
-
Current insights in non-invasive ventilation for the treatment of neonatal respiratory disease
Italian Journal of Pediatrics (2019)
-
Enteral Nutrition Tolerance And REspiratory Support (ENTARES) Study in preterm infants: study protocol for a randomized controlled trial
Trials (2019)
