
Abstract
Gastric hyperplastic polyps in organ transplant recipients have been recently described; however, the clinical significance of hyperplastic polyps in this setting remains unclear. The aim of this study is to further characterize the clinical presentation and histopathology of gastric hyperplastic polyps in organ transplant recipients as compared to hyperplastic polyps in non-transplant individuals. All gastric hyperplastic polyps diagnosed in our institute from 1999 to 2005 were retrieved. Clinical data including endoscopic findings were reviewed. Twenty cases without history of transplantation were randomly selected for a control population. Hematoxylin and eosin and Genta stains were reviewed. 104 cases of gastric hyperplastic polyps were identified. Sixteen (15%) had a history of solid organ (one liver/kidney, four livers, one lung, one kidney, one kidney/pancreas, three hearts) or bone marrow transplantation (five). The average time after transplantation was 28 months. Signs/symptoms leading to endoscopy were more frequently nausea/vomiting in transplant patients as compared to bleeding/hematemesis/anemia in non-transplant patients. The transplant patients tended to be younger with a reversed M:F ratio, but age was the only demographic factor that was statistically significant. There was no difference in polyp size, location and number. Histologically, no difference was observed in the frequency of active inflammation, Helicobacter pylori infection or intestinal metaplasia. Dysplasia was not present in any of the cases. None of the patients had a history of polyposis syndrome. In conclusion, a significant percentage of gastric hyperplastic polyps (15%) were from organ transplant patients, further suggesting a strong association of gastric hyperplastic polyps with transplantation. The younger age in the transplant group may be explained by the nature of the cohort qualified for transplantation. While no statistically significant differences in histopathologic features were found between transplant and non-transplant groups, analysis was limited by small case numbers. Overall, gastric hyperplastic polyps in the post transplant setting is a common, but under-recognized entity and merits further clinicopathologic analysis.
Similar content being viewed by others


Main
Gastrointestinal complications in transplant recipients can affect any portion of the gastrointestinal tract and may involve multiple processes.1, 2 Gastric complications include peptic ulcer disease, post-transplant lymphoproliferative disorders, graft-versus-host disease and infection and may be linked to medication, infection or exacerbation of pre-existing lesions.1, 2 An uncommon occurrence in the general population, the development of gastric hyperplastic polyps in the solid organ transplant recipient recently has been described.3 Hyperplastic polyp is one of the most common gastric epithelial polyps. Although its pathogenesis remains unclear, it is associated with chronic gastritis and Helicobacter pylori infection.4, 5 Although hyperplastic polyp is generally considered benign, dysplasia and malignancy have been described; however, the relative risk for neoplastic transformation does exceed that of the background pathology in which hyperplastic polyp arises.4, 6, 7, 8, 9, 10 Neither the biologic relationship between hyperplastic polyps and transplantation nor the clinical significance of hyperplastic polyps in this context has been determined. The aim of this study is to characterize the clinical and histopathologic features of hyperplastic polyps that developed in organ transplant recipients as compared with hyperplastic polyps in non-transplant individuals.
Materials and methods
The study protocol was reviewed and approved by the Human Subject Division at the University of Washington. A search of the pathology database at the University of Washington (Powerpath) was performed to identify specimens with the diagnosis of hyperplastic polyp between 1 January 1999 and 31 December 2005. Clinical and endoscopic data were obtained from the patients' computerized records. A total of 104 cases were identified, 16 (15%) of which had a history of solid organ or bone marrow transplantation. Twenty non-transplant associated cases were randomly selected as a control population. Hematoxylin and eosin (H&E) and Genta stains performed for routine histologic evaluation on the 16 transplant-associated cases and the 20 non-transplant-associated control cases were reviewed. Three gastric lesions in bone marrow transplant recipients had H&E and argyrophil stains available for review. The diagnosis of hyperplastic polyp was confirmed by the polypoid appearance on endoscopy and the microscopic presence of hyperplastic foveolar epithelium forming tortuous and cystically dilated structures with or without inflamed stroma (Figure 1a–c), according to histopathologic criteria previously characterized.4 When available, the following clinical and histologic data were collected: age, gender, size and location of polyp, the presence of intestinal metaplasia, dysplasia and active inflammation. The presence of Helicobacter pylori was evaluated in H&E and Genta stains (or argyrophile). Statistical analysis was preformed using χ2 and two-tailed t-tests. A P-value of <0.05 was considered statistically significant.

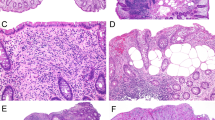
An example of a transplant-associated gastric hyperplastic polyp showing a polypoid configuration with tortuous and hyperplastic foveolar epithelium in low magnification (a). Higher magnification shows hyperplastic and tortuous foveolar epithelium of the gastric hyperplastic polyp (b). The lamina propria shows edematous stroma and scarce inflammation (c) and there is focal intestinal metaplasia without dysplasia (d).
Results
Among 104 examples of gastric hyperplastic polyp, none were associated with a history of a polyposis syndrome. As is shown in Table 1, 16 cases had a history of previous organ transplantation including liver/kidney (n=1), lung (n=1), liver (n=4), kidney (n=1), heart (n=3), kidney/pancreas (n=1) and allogenic bone marrow (n=5). The relevant gastric biopsy was obtained an average of 28 months after transplantation (range, 9 days–13 years). As is revealed in Table 2, the average age of the transplant group at the time of gastric biopsy was 47 years compared to 60 years in the control group (P=0.0002); a slight male predominance was noted in the transplant group, whereas a female predominance was apparent in the control group (P=0.31). The most common sign or symptom leading to endoscopy in the transplant group was nausea/vomiting (50%) while hematemesis/bleeding/anemia (53%) was most common in the non-transplant group. The incidence of diarrhea (7 vs 5%), epigastric pain/dyspepsia (29 vs 21%), dysphagia/odynophagia/cough (14 vs 11%) and evaluation for malignancy (14 vs 5%) was generally similar in transplant and non-transplant groups, respectively. Importantly, group-based differences were not statistically significant for any symptom/sign cluster. The average polyp size overall was nearly equal for both groups: 1.3 cm (range, 0.3–10 cm) in the transplant group and 1.6 cm (range 0.3–4.0 cm) in the control group (P=0.23). Similarly, there was no significant difference in polyp number and location between the two groups with the majority occurring singly and in the antrum (single/antral in 56/58% of the transplant and 75/70% of the non-transplant patients, P=0.97). Of seven transplant patients who had concomitant viral culture and/or CMV serologies performed, only one was CMV-positive on culture (histologically occult).
Histologic review of active inflammation, eosinophil counts, intestinal metaplasia, dysplasia and Helicobacter pylori infection revealed no statistically significant difference between the two groups (Table 3). Active inflammation approached significance: it was more frequently seen in non-transplant-associated polyps (75%) when compared to transplant-associated polyps (31%, P=0.06). Viral cytopathic effect was observed only in one transplant patient; this patient's biopsy had only focal active inflammation and no intestinal metaplasia/dysplasia (no culture/serologic studies were performed). Eosinophil counts performed in the most eosinophil rich areas for both were about equal with an average of 18 eosinophils/10 hpf (s.d. 21) for the transplant group and 26 eosinophils/10 hpf (s.d. 19) in the non-transplant group (P=0.23). Furthermore, there was no significant difference in erosion between the two groups. Ulcer is not a common finding in either group. Intestinal metaplasia (Figure 1d) was relatively common in both groups, seen in three (18%) transplant-associated polyps and seven (35%) non-transplant-associated polyps (P=0.75). Dysplasia was not present in any of the polyps reviewed. Helicobacter pylori was not identified in the transplant group and in only one patient (5%) in the non-transplant group (P=0.84).
Background (non-polyp) gastric mucosal biopsies were available for evaluation in six (37%) transplant and five (25%) non-transplant patients. Of the transplant-associated polyps, background gastric pathology included two cases of chronic gastritis and Helicobacter pylori negative, one example of reactive gastropathy with amyloidosis, one with erosive gastropathy and two samples with normal gastric mucosa. Of the non-transplant-associated polyps, background gastric pathology included two cases of chronic gastritis, one Helicobacter pylori positive, one instance of antral reactive gastropathy, one example of antral intestinal metaplasia with carcinoid tumor and one sample with normal gastric mucosa. Only one of the five bone marrow transplant patients had histologic evidence of graft-versus-host disease (GVHD) involving the stomach (graded as mild).
Discussion
Gastric epithelial polyps are relatively uncommon in the general population. The estimated incidence is less than 1%, and hyperplastic polyps are the most common.2, 5, 11, 12, 13 The development of gastric hyperplastic polyps in recipients of solid organ transplants has been recently described by Amaro et al.3 In their study, 10 solid organ transplant recipients (seven men, three women, 61 years median age) with hyperplastic polyps were examined. Notably hyperplastic polyps in these cases were more often multiple, involving the atrium and lacking neoplastic change. These lesions were not associated with Helicobacter pylori gastritis. Bone marrow transplant recipients were not included, and histopathologic comparison to non-transplant related hyperplastic polyps was not performed. A goal of our study was to better define the incidence of transplant-associated gastric hyperplastic polyps and to provide a clear comparison of these lesions with non-transplant hyperplastic polyps. Our selected transplant population included both bone marrow and solid organ transplantation, so that the potential implications of allograft recipient status could be more fully explored.
Of 104 hyperplastic polyps diagnosed at our institution over the time interval studied (84 months), a surprisingly large number occurred in transplant recipients (15%). Even allowing for the population bias at our institution (transplant-rich) and for the sampling bias due to the frequency of endoscopic examination in transplant patients, the number of hyperplastic polyps in this group nevertheless appears disproportionately high. In addition, our study indicates that this association applies to all organ transplantation, including five (31%) bone marrow transplant patients.
In the original report by Amaro et al,3 most of the patients had multiple polyps (nine of 10 cases) located in the antrum, all less than 1.5 cm in size. In contrast, results of our study do not indicate a higher preponderance of multiple polyps in the transplant recipient as compared to controls. Although we also noted a predilection for antral involvement in transplant patients, antral location was also most common in non-transplant patients and, indeed, represents the most common location for hyperplastic polyps in all patients.4
Since hyperplastic polyp is thought to arise in a background of chronic gastritis, immunosuppression and infection might reasonably play an important role in the pathogenesis of and predilection for hyperplastic polyp in transplant patients.4 Instead, evidence of infection was conspicuously absent in the earlier series. Neither Helicobacter pylori nor chronic active gastritis/intestinal metaplasia were identified in any of the 10 cases, and CMV serologies were negative in nine patients.3 Similarly, we found no evidence of Helicobacter pylori by Genta/argyrophile stains in any patient. Evidence of CMV infection was seen in only two of 16 patients (12%; one positive only on culture and histologically occult) representing a higher frequency than the 2% reported in all patients,4 (and likely an artifact of small sample size).
Intestinal metaplasia, dysplasia and malignancy have been identified in hyperplastic polyp, but the malignant potential of the hyperplastic lesions does not rise above that of whatever background mucosal pathology may exist.4 Although Amaro et al3 did not find intestinal metaplasia in their examples, this phenomenon was not infrequent in the transplant-associated polyps in our series. Nevertheless neither dysplasia nor malignancy was identified in any of our cases.
In our comparison of hyperplastic polyps arising in transplant recipients and in non-transplant patients, we found no significantly different clinical or histopathologic feature (apart from age), indicating that hyperplastic polyps in these two populations likely share a common pathogenesis. Further, eosinophil counts and apoptotic debris were not significantly increased in transplant hyperplastic polyp, making other conditions such as parasitic infestations, hypersensitivity and drug reactions less likely etiologies, and only minimal GVHD was seen in only one of the five bone marrow transplant cases. Notably, background mucosal biopsies were lacking for both groups. As noted earlier, evaluation of background mucosa is an important element in the assessment of biologic potential in hyperplastic polyp and biopsy of only the gastric polyp is a limitation of the present study, but also a note of caution in the endoscopic evaluation of gastric polyps in general.4
In conclusion, gastric hyperplastic polyp occurred in a surprisingly high proportion (15%) of transplant recipients at our institution, a population that included bone marrow transplant recipients in addition to solid organ transplant recipients. Transplant patients with hyperplastic polyp tended to be younger with a male predominance, though this may reflect the patient population selected for transplantation. No other clear clinical or histopathologic differences were identified, between transplant and non-transplant patients. Given the challenge of the immunocompromised patient, clinical concern for infection is paramount. Results of this study show that both histologic and microbiologic methods of assessing infectious status, particularly CMV viral infection, were important, since histologic viral cytopathic effect was seen in only one of the two patients with proven CMV infection. Importantly, lack of background mucosal biopsies in this series limited our ability to assess the pathology out of which the hyperplastic polyps arose. Further study of hyperplastic polyp including series from other transplant centers is required to confirm our observation that these lesions arise more frequently in the transplant recipient compared to the general population, and whether hyperplastic polyp in this setting may yet be the product of a distinctive pathogenesis with a biologic behavior that arises from the norm. However, this study does illustrate the need for combined laboratory assessment of infectious status in transplant recipients, and emphasizes the importance of obtaining biopsies of the background mucosa in patients with polypoid lesions.
References
Ponticelli C, Passerini P . Gastrointestinal complications in renal transplant recipients. Transplant Int 2005;18:643–650.
Hsi ED, Singleton TP, Swinnen L, et al. Mucosa-associated lymphoid tissue-type lymphomas occurring in post-transplantation patients. Am J Surg Pathol 2000;24:100–106.
Amaro R, Neff GW, Karnam US, et al. Acquired hyperplastic gastric polyps in solid organ transplant patients. Am J Gastroenterol 2002;97:2220–2224.
Abraham SC, Singh VK, Yardley JH, et al. Hyperplastic polyps of the stomach; associations with histologic patterns of gastritis and gastric atrophy. Am J Surg Pathol 2001;25:500–507.
Ljubicic N, Kujundzic M, Roic G, et al. Benign epithelial gastric polyps—frequency, location and age, and sex distribution. Coll Antropol 2002;26:55–60.
Orlowska J, Jarosz D, Pachlewski J, et al. Malignant transformation of benign epithelial gastric polyps. Am J Gastroenterol 1995;90:2152–2159.
Gencosmanoglu R, Sen-Oran E, Kurtkaya-Yapicier O, et al. Gastric polypoid lesion: analysis of 150 endoscopic polypectomy specimens from 91 patients. World J Gastroenterol 2003;9:2236–2239.
Papa A, Cammarota G, Tursi A, et al. Histologic types and surveillance of gastric polyps: a seven year clinico-pathological study. Hepatogastroenterology 1998;45:579–582.
Snover DC . Benign epithelial polyps of the stomach. Pathol Annu 1985;20 (Part 1):303–329.
Murakami K, Mitomi H, Yamashita K, et al. P53, but not c-Ki-ras, mutation and down-regulation of p21WAF1/CIP1 and cyclin D1 are associated with malignant transformation in gastric hyperplastic polyps. Am J Clin Pathol 2001;115:224–234.
Archimandritis A, Spiliadis C, Tzivras M, et al. Gastric epithelial polyps: a retrospective endoscopic study of 12974 symptomatic patients. Ital J Gastroenterol 1996;28:387–390.
Deppisch LM, Rona VT . Gastric epithelial polyps. A 10-year study. J Clin Gastroenterol 1989;11:110–115.
Macenlle Garcia R, Bassante Flores LA, Fernandez Seara J . Gastric epithelial polyps. A retrospective study 1995–2000. Rev Clin Esp 2003;203:368–372.
Acknowledgements
This work was presented in part at the Annual Meeting of the United States and Canadian Academy of Pathology, 2006.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jewell, K., Toweill, D., Swanson, P. et al. Gastric hyperplastic polyps in post transplant patients: a clinicopathologic study. Mod Pathol 21, 1108–1112 (2008). https://doi.org/10.1038/modpathol.2008.87
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.2008.87
Keywords
This article is cited by
-
Gastric Hyperplastic Polyps: A Review
Digestive Diseases and Sciences (2009)
