
Abstract
Background:
To evaluate whether the extent of baseline acute prostate inflammation (API) and chronic prostate inflammation (CPI) was associated with risk of prostate cancer (PCa) at 2-year repeat prostate biopsy in a clinical trial with systematic biopsies independent of PSA.
Methods:
A retrospective analysis of 6065 men with a negative baseline biopsy in the reduction by dutasteride of PCa events (REDUCE) trial undergoing 2-year biopsy. API and CPI extent (percentage of cores involved) and PCa (present or absent) were assessed by central pathology. The association of baseline API and CPI with PCa at the 2-year biopsy was evaluated with logistic regression in uni- and multivariable analyses.
Results:
API extent was classified as absent or involving 1–25%, 26–50%, 51–75% and >75% cores in 5140 (85%), 742 (12%), 151 (2%), 17 (<1%) and 15 (<1%) cases, respectively. CPI extent was classified as absent or involving 1–25%, 26–50%, 51–75% and >75% cores in 1367 (22%), 2532 (42%), 1474 (24%), 397 (7%) and 295 (5%) cases, respectively. More extensive API was associated with younger age, lower PSA and lower prostate volume, while more extensive CPI was associated with older age, lower PSA and higher prostate volume (all P<0.01). In both uni- and multivariable analyses, API and CPI extent were associated with lower risk of PCa at the 2-year biopsy (both P<0.01).
Conclusions:
In a cohort of men undergoing repeat prostate biopsy 2 years after a negative baseline biopsy, a greater extent of baseline API and CPI was independently associated with lower PCa risk.
Similar content being viewed by others

Introduction
Histological inflammation is a common finding among prostate biopsies done for cancer detection. Previous studies have shown that between 35 and 100% of prostate needle biopsies have some degree of histological inflammation.1, 2, 3, 4 However, the clinical implications of prostate inflammation are controversial. Whereas some studies have shown a correlation between inflammation and higher risk of prostate cancer (PCa),5, 6, 7, 8 many have failed to demonstrate any relationship between inflammation and cancer9 and others have found inflammation to be associated with a lower PCa risk.10, 11, 12 Indeed, we previously showed that the presence and severity of acute prostate inflammation (API) and chronic prostate inflammation (CPI) were associated with lower PCa risk in repeat biopsies.13 However, the extent of the inflammatory infiltrate in the prostate varies from patient to patient.14 While some men have focal inflammation, others have a more diffuse prostate involvement. To date, no studies have evaluated the association of the extent of inflammation with PCa. Thus, we sought to evaluate whether the extent of baseline API and CPI was associated with the incidence of PCa at the 2-year repeat prostate biopsy among subjects in the Reduction by Dutasteride of PCa Events (REDUCE) study, a clinical trial with systematic biopsies regardless of PSA levels.15 Given our previous finding that inflammation was associated with lower PCa risk, we hypothesized that more extensive inflammation was associated with lower PCa risk.13
Materials and Methods
Study sample
The design of the REDUCE trial has been published previously.15 In brief, eligible men were aged 50–75 years, had serum PSA ⩾2.5 or 3.0 ng ml−1 according to age (50–60 and 60–75 years, respectively) but ⩽10 ng ml−1, and had undergone single negative prostate biopsy (6–12 cores) within 6 months of enrollment. Men were excluded if they had history of PCa, high-grade intraepithelial neoplasia, atypical small acinar proliferation, prostate volume >80 ml, previous prostate surgery, or an International Prostate Symptom Score ⩾25 or ⩾20 on alpha-blockers. Medical history was obtained at baseline. All men were randomized in a double-blind fashion to receive orally either dutasteride 0.5 mg or placebo daily and followed every 6 months for 4 years. To maintain the blinded nature of the study, PSA levels in the dutasteride-treated men were doubled (given dutasteride reduces PSA levels by approximately half)16 and randomly adjusted by 0.1 ng ml−1 so that the final reported values were equally even and odd. Ten-core transrectal, ultrasound-guided biopsies were performed as part of the protocol at 2 and 4 years regardless of changes in PSA. Baseline biopsies had been performed before the start of the study (and independently of the study) and were reread centrally (at Bostwick Laboratories, Glen Allen, VA, USA). Biopsies that were performed as part of the study were also read centrally. Inflammation was reviewed by two pathologists independently; when discrepancies were encountered, brief discussion invariably led to consensus. The central pathology laboratory had no access to the randomization codes. PCa, API and CPI were coded as present or absent for each biopsy core. Inflammation was defined by the presence of nests of 10 or more inflammatory cells. CPI consisted mainly of lymphocytes and a variable number of plasma cells and macrophages. API consisted of neutrophillic infiltrate.17 The extent of API and CPI was determined by dividing the number of biopsy cores with inflammation (regardless of the extension within the core) by the total number of cores sampled. The protocol was approved by the institutional review board at each research site, and all participants provided written informed consent. Of the 8231 men enrolled in the study, 6316 (77%) had a per-protocol 2-year prostate biopsy. The details of the men who underwent at least one on-study biopsy have been published previously.18 Of these, we excluded 251 (4%) due to missing data in one or more of the covariates in study (see below). This resulted in a total study sample of 6065 men.
Statistical analysis
The extent of API and CPI was divided into five groups: absent, or involving 1–25%, 26–50%, 51–75% and >75% of the biopsy cores. Univariable comparisons of baseline characteristics across API and CPI groups were performed using Fisher’s exact test for categorical data and linear regression for continuous variables, with the extent of inflammation coded as a 5-level categorical variable. The association of the extent of API with that of CPI was evaluated with linear regression, with extent as a linear variable (0 –100%). The association of the extent of API and CPI with risk of PCa at the 2-year repeat biopsy was evaluated with logistic regression in uni- and multivariable analyses. Multivariable analyses were adjusted for age (continuous, in years), race (white or non-white), body mass index (continuous, in kg/m2), family history of PCa (positive or negative), digital rectal exam (coded as normal or abnormal), prostate volume (continuous, in cm3), baseline PSA (continuous, in ng ml−1) and treatment arm (dutasteride or placebo). API and CPI groups were modeled as linear variables (1–5) to analyze trends. Locally weighted scatterplot smoothing regression was used to generate a plot depicting the association of the extent of inflammation with the risk of prostate cancer. All covariates were determined prior to the repeat biopsy. All statistical analyses were two-tailed and performed using Stata 12.0 (StataCorp, College Station, TX, USA). A P<0.01 was considered to indicate statistical significance.
Results
Of the 6065 men included in the study, 5568 (92%) were white. The median (and interquartile range) age and body mass index were 63 years (58–67) and 26.8 kg/m2 (24.8–29.4), respectively. A total of 800 men (13%) had a positive family history of PCa and 221 (3%) had abnormal digital rectal exam. The median (and interquartile range) baseline PSA was 5.7 ng ml−1 (4.4–7.3) and prostate volume was 43 cm3 (33–56).
The extent of API was classified as absent or involving 1–25%, 26–50%, 51–75% and >75% cores in 5140 (85%), 742 (12%), 151 (2%), 17 (<1%) and 15 (<1%) cases, respectively (Table 1). More extensive API was associated with younger age, lower PSA and lower prostate volume (all P<0.01). The extent of CPI was classified as absent or involving 1–25%, 26–50%, 51–75% and >75% cores in 1367 (22%), 2532 (42%), 1474 (24%), 397 (7%) and 295 (5%) cases, respectively (Table 2). More extensive CPI was associated with older age, lower PSA and higher prostate volume (all P<0.01). Although a greater extent of API was associated with a greater extent of CPI, the strength of the association was weak (coefficient 0.13, P<0.001).
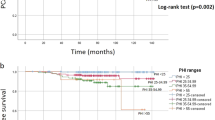
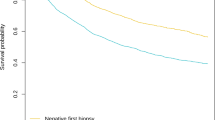
In univariable analysis, the extent of API and CPI were both associated with lower risk of PCa at the 2-year biopsy (both P for trend<0.01). Overall, compared with men without API, those with API had a lower risk of PCa (P for trend=0.01). Similarly, men with CPI had a lower risk of PCa compared with those without CPI (P for trend<0.001). In multivariable analysis, greater extent of API and CPI was independently associated with lower PCa risk (both P for trend<0.01, Table 3, Supplementary Figure 1).
Discussion
The greater extent and severity of the inflammatory infiltrate in the prostate has previously been associated with PSA levels.19 Given elevated PSA is usually the trigger for a prostate biopsy, many of the previous studies evaluating the association of inflammation and PCa were limited by PSA selection, where only those with elevated PSA underwent biopsy and were potentially diagnosed with PCa. As such, patients with PSA elevation due to inflammation would be more likely to undergo biopsy and eventually be diagnosed with PCa. This could give the false impression that inflammation was associated with increased PCa risk. To avoid this limitation, we used data from the REDUCE trial, where patients underwent repeat biopsies regardless of PSA levels. We evaluated whether the extent of baseline API and CPI was associated with the subsequent risk of PCa. In both uni- and multivariable analysis, we found greater extent of baseline API and CPI to be independently associated with lower PCa risk at the 2-year repeat biopsy.
The presence and extent of inflammation is not routinely reported by all pathologists in a systematic fashion. Indeed, a study among European pathologists showed that only half of the pathologists systematically reported the presence of inflammation in prostate needle biopsies.20 Moreover, how the extent of inflammation was determined varied from pathologist to pathologist. For example, some studies have measured the extent of inflammation based on the confluence of the inflammatory infiltrate, while others, including our study, measured inflammation based on the percentage of cores with inflammatory infiltrate.19 Regardless of how inflammation was reported, several studies have shown that the extent of inflammatory infiltrate in the prostate of men undergoing needle biopsy for PCa detection varies considerably from patient to patient.19, 21 For example, in a study of men with a prostate biopsy negative for PCa, nearly one-third had inflammation in <20%, 20–50% and >50% of the cores sampled, respectively.21 In our study, we found API involving 1–25%, 26–50%, 51–75% and >75% of the cores in 12%, 3%, <1% and <1% of the cases, respectively. CPI was found in 1–25%, 26–50%, 51–75% and >75% of the cores in 42%, 24%, 7% and 5% of the cases, respectively. Thus, given the variability of inflammation extent and the multiplicity of measuring schemes, standards of inflammation reporting are needed. Moreover, given the association between greater extent of inflammation and lower cancer risk on subsequent biopsy observed in our study, our results suggest inflammation should be routinely reported in negative prostate biopsies.
The causes and clinical implications of asymptomatic prostate inflammation are not completely understood. Previously, chronic inflammatory infiltrate has been associated with older age and larger prostates.22 Similarly, we found that more extensive CPI was associated with older age and higher prostate volume. In contrast, API was associated with younger age and lower prostate volume. These findings suggest that the potential causes of API and CPI may differ, for example, one is associated with larger prostates while the other is associated with smaller prostates. Moreover, previous studies have linked inflammation to elevated PSA.2, 19 In our study, where inflammation was divided into acute and chronic based on the type of inflammatory infiltrate, more extensive API and CPI were associated with lower PSA levels. Thus, further studies evaluating the association of inflammation and PSA levels are still needed to help counsel patients with prostate inflammation and elevated PSA levels, that is, whether the elevated PSA level is related to inflammation or another cause such as PCa.
The establishment of causality in retrospective studies is often not possible given the potential influence of confounders. However, certain study characteristics such as temporal connection, where the cause precedes the outcome, and a dose–response relationship between cause and effect provide additional support for a causal hypothesis. Thus, in the current study, we evaluated the risk of PCa as a function of the extent of API and CPI measured in a baseline biopsy done 2 years prior to the index biopsy. Although we acknowledge that a negative prostate biopsy does not completely rule out PCa, our study indicates a temporal relationship where inflammation was present before the diagnosis of PCa. Moreover, given the extent of API and CPI was independently associated with a lower risk of PCa showing a dose–response relationship, these findings suggest a potential causal association of inflammation and lower risk of PCa. Nevertheless, validation of our results, as well as further research into understanding the potential causality of inflammation and lower risk of PCa, is needed to confirm our findings.
Although the REDUCE trial has many strengths, including its large international and multicentric population, per-protocol biopsies regardless of PSA levels, prospective data acquisition and central pathology review, it is not devoid of limitations. The main limitation of our study is that only men with PSA levels between 2.5 and 10 ng dl−1 were included. Moreover, men with high-grade intraepithelial neoplasia, atypical small acinar proliferation, prostate volume >80 ml, and those with history of previous prostate surgery or International Prostate Symptom Score ⩾25 or ⩾20 on alpha-blockers were excluded. These exclusions increase the homogeneity of the sample but also limit the generalizability of our findings. Although the pathology review was done in a single center with pre-specified criteria for acute and chronic inflammation, some interobserver variability across different uropathologists may be present. As such, studies using a computerized pathology system may minimize the variation between pathologists. In addition, we did not analyze off-protocol biopsies, including transrectal/transperineal needle biopsies, transurethral resections and prostatectomies of any kind. For-cause biopsies were not analyzed given the inclusion of them would also pose a potential bias, as these biopsies were triggered by elevated PSA and/or abnormal digital rectal exam. Also, we did not evaluate the extent of inflammation within each core. Less than 1% of subjects had an extent of acute prostate inflammation >50%. Finally, we did not evaluate specific types of inflammation such as granulomatous and eosinophilic prostatitis as separate entities, given these are not commonly found in prostate biopsies.
In conclusion, among men undergoing repeat prostate biopsy 2 years after a negative baseline biopsy, greater extent of baseline API and CPI was independently associated with lower PCa risk.
References
Pepe P, Aragona F . Does an inflammatory pattern at primary biopsy suggest a lower risk for prostate cancer at repeated saturation prostate biopsy? Urol Int 2011; 87: 171–174.
Gui-Zhong L, Libo M, Guanglin H, Jianwei W . The correlation of extent and grade of inflammation with serum PSA levels in patients with IV prostatitis. Int Urol Nephrol 2011; 43: 295–301.
Sfanos KS, De Marzo AM . Prostate cancer and inflammation: the evidence. Histopathology 2012; 60: 199–215.
Schatteman PH, Hoekx L, Wyndaele JJ, Jeuris W, Van Marck E . Inflammation in prostate biopsies of men without prostatic malignancy or clinical prostatitis: correlation with total serum PSA and PSA density. Eur Urol 2000; 37: 404–412.
Rosenblatt KA, Wicklund KG, Stanford JL . Sexual factors and the risk of prostate cancer. Am J Epidemiol 2001; 153: 1152–1158.
Sarma AV, McLaughlin JC, Wallner LP, Dunn RL, Cooney KA, Schottenfeld D et al. Sexual behavior, sexually transmitted diseases and prostatitis: the risk of prostate cancer in black men. J Urol 2006; 176: 1108–1113.
Dennis LK, Lynch CF, Torner JC . Epidemiologic association between prostatitis and prostate cancer. Urology 2002; 60: 78–83.
Cheng I, Witte JS, Jacobsen SJ, Haque R, Quinn VP, Quesenberry CP et al. Prostatitis, sexually transmitted diseases, and prostate cancer: the California Men's Health Study. PLoS One 2010; 5: e8736.
Yli-Hemminki TH, Laurila M, Auvinen A, Maattanen L, Huhtala H, Tammela TL et al. Histological inflammation and risk of subsequent prostate cancer among men with initially elevated serum prostate-specific antigen (PSA) concentration in the Finnish prostate cancer screening trial. BJU Int 2013; 112: 735–741.
Gann PH, Fought A, Deaton R, Catalona WJ, Vonesh E . Risk factors for prostate cancer detection after a negative biopsy: a novel multivariable longitudinal approach. J Clin Oncol 2010; 28: 1714–1720.
Fujita K, Hosomi M, Tanigawa G, Okumi M, Fushimi H, Yamaguchi S . Prostatic inflammation detected in initial biopsy specimens and urinary pyuria are predictors of negative repeat prostate biopsy. J Urol 2011; 185: 1722–1727.
Kryvenko ON, Jankowski M, Chitale DA, Tang D, Rundle A, Trudeau S et al. Inflammation and preneoplastic lesions in benign prostate as risk factors for prostate cancer. Mod Pathol 2012; 25: 1023–1032.
Moreira DM, Nickel JC, Gerber L, Muller RL, Andriole GL, Castro-Santamaria R et al. Baseline prostate inflammation is associated with a reduced risk of prostate cancer in men undergoing repeat prostate biopsy: Results from the REDUCE study. Cancer 2013; 121: 4271.
Yaman O, Gogus C, Tulunay O, Tokatli Z, Ozden E . Increased prostate-specific antigen in subclinical prostatitis: the role of aggressiveness and extension of inflammation. Urol Int 2003; 71: 160–164.
Andriole GL, Bostwick DG, Brawley OW, Gomella LG, Marberger M, Montorsi F et al. Effect of dutasteride on the risk of prostate cancer. N Engl J Med 2010; 362: 1192–1202.
Andriole GL, Kirby R . Safety and tolerability of the dual 5alpha-reductase inhibitor dutasteride in the treatment of benign prostatic hyperplasia. Eur Urol 2003; 44: 82–88.
Nickel JC, Roehrborn CG, O'Leary MP, Bostwick DG, Somerville MC, Rittmaster RS . Examination of the relationship between symptoms of prostatitis and histological inflammation: baseline data from the REDUCE chemoprevention trial. J Urol 2007; 178: 896–900.
Wu C, Moreira DM, Gerber L, Rittmaster RS, Andriole GL, Freedland SJ . Diabetes and prostate cancer risk in the REDUCE trial. Prostate Cancer Prostatic Dis 2011; 14: 326–331.
Kandirali E, Boran C, Serin E, Semercioz A, Metin A . Association of extent and aggressiveness of inflammation with serum PSA levels and PSA density in asymptomatic patients. Urology 2007; 70: 743–747.
Berney DM, Algaba F, Camparo P, Comperat E, Griffiths D, Kristiansen G et al. Variation in reporting of cancer extent and benign histology in prostate biopsies among European pathologists. Virchows Arch 2014; 464: 583–587.
Simardi LH, Tobias-MacHado M, Kappaz GT, Taschner Goldenstein P, Potts JM, Wroclawski ER . Influence of asymptomatic histologic prostatitis on serum prostate-specific antigen: a prospective study. Urology 2004; 64: 1098–1101.
Di Silverio F, Gentile V, De Matteis A, Mariotti G, Giuseppe V, Luigi PA et al. Distribution of inflammation, pre-malignant lesions, incidental carcinoma in histologically confirmed benign prostatic hyperplasia: a retrospective analysis. Eur Urol 2003; 43: 164–175.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
RC-S is employed by GlaxoSmithKline. SJF has received a grant from GlaxoSmithKline. JCN has acted as a consultant for GlaxoSmithKline, Pfizer, Astellas and Lilly. He has provided expert testimony for GlaxoSmithKline and has received a grant from the company for the BPH Prostatitis Investigator-Initiated Study. GLA has received a grant from GlaxoSmithKline as well as a consulting fee for acting as chair of the REDUCE Steering Committee. He has also acted as a consultant for Bayer, Genomic Health, GlaxoSmithKline and Myriad Genetics. DMM declares no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Prostate Cancer and Prostatic Diseases website
Supplementary information
Rights and permissions
About this article

Cite this article
Moreira, D., Nickel, J., Andriole, G. et al. Greater extent of prostate inflammation in negative biopsies is associated with lower risk of prostate cancer on repeat biopsy: results from the REDUCE study. Prostate Cancer Prostatic Dis 19, 180–184 (2016). https://doi.org/10.1038/pcan.2015.66
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pcan.2015.66
This article is cited by
-
The combination of histological prostate atrophy and inflammation is associated with lower risk of prostate cancer in biopsy specimens
Prostate Cancer and Prostatic Diseases (2017)
