
Abstract
Measurements of cerebral oxygen consumption (CVo2) may improve our understanding of cerebral oxygenation, but there are few published data for sick neonates. Although cerebral maturation is associated with an increase in cerebral glucose consumption, the relationship between CVo2 and increasing gestational age has not previously been assessed in humans. The aims of this study were to evaluate a noninvasive method for the estimation of CVo2 in the neonate using near infrared spectroscopy, and to investigate the relationship between gestational age and CVo2. Twenty babies who were undergoing intensive care in the neonatal period were studied. Cerebral hemoglobin flow (CHbF) and cerebral venous oxyhemoglobin saturation (CSvo2) were measured using near infrared spectroscopy. Arterial oxyhemoglobin saturation was measure by pulse oximetry (Spo2). CVo2 was calculated from the equation: CVo2 = CHbF ×(Spo2 - Svo2 × 4. The median (range) CVo2 was 0.9(0.52-1.76) mL·100 g-1 min-1. There was an increase in CVo2 with advancing gestational age (n = 20, ρ = 0.55,p = 0.014). We conclude that CVo2 can be estimated in sick neonates using noninvasive optical methods. The values obtained are similar to those obtained in other studies by more invasive methods, and are in agreement with values which would be expected from the known rate of cerebral glucose consumption in neonates. Mean (SD) CVo2 at 24-26 wk was 0.5 (0.18) mL·100 g-1 min-1 and rose with increasing gestation to term by 0.03 mL·100 g-1 min-1 per wk.
Similar content being viewed by others


Main
Cerebral hypoxia and ischemia are important causes of long-term morbidity among babies who have undergone neonatal intensive care. Because of this there has been much interest in studying the cerebral circulation during the neonatal period using a variety of methods. These studies have provided important insights into the mechanisms which control or influence CBF in health and disease. However, despite the information generated by these studies, they have had little impact on clinical management during neonatal intensive care. A possible reason for this is that most of the studies have concentrated on measuring CBF or changes in CBF. Although such measurements provide information about the rate of oxygen delivery, or changes in the rate of oxygen delivery, to the brain, they cannot give a complete picture of cerebral oxygenation because they do not take into account the cerebral oxygen requirement. Cerebral oxidative metabolism and energetics have been studied after perinatal asphyxia using magnetic resonance spectroscopy(1), but these techniques cannot be easily performed at the cotside during the course of intensive care. Attempts have also been made to study changes in cerebral oxygenation using NIRS to monitor changes in the cerebral concentration of cytochrome aa3(2). However, this technique has, as yet, found limited acceptance. There have been concerns about the differences in the algorithms used by different NIRS systems for measuring cytochrome aa3(3,4), and concerns have been raised that the changes observed after perinatal asphyxia may represent changes in the optical characteristics of the brain, rather than true changes in cytochrome aa3(5).
Clinical events and interventions during the course of neonatal intensive care have been shown to alter cerebral hemodynamics. As long as oxygen delivery remains sufficient for the brain's requirements, a reduction in perfusion is unlikely to be of any clinical relevance. In these circumstances, a reduction in the rate of CDo2 would not be accompanied by a reduction the rate of oxygen consumption as long as the level of cerebral activity did not alter significantly. A spontaneous reduction in CVo2 may be a consequence of reduced cerebral activity. However, reduced CVo2 due to a reduction in cerebral perfusion may indicate that oxygen delivery has been reduced to a level that does not meet cerebral oxygen demand. Such a reduction would represent true hypoxia and is likely to be of clinical relevance. The implication of this is that measurements of CVo2 may provide useful information about the adequacy of cerebral oxygenation.
Measurements of CVo2 seem to be of use when studying adults with cerebral ischemia. A range for CVo2 of 3.2 to 3.7 mL·100 g-1 min-1 is typically seen in resting healthy adults(6–12). Several studies in adults with cerebral ischemia have shown that rates of CVo2 of less than 1.3-1.5 mL·100 g-1 min-1 are strongly associated with permanent cerebral ischemic injury(13,14) and that areas of brain vulnerable to infarction are better identified by measurements of CVo2 than by measurements of CBF, cerebral blood volume, or cerebral oxygen extraction(14). The adult brain, however, is structurally and metabolically different from the neonatal brain as there are significant maturational changes within the brain during the last trimester. It is possible that the minimal level of CVo2 that applies to the adult brain may be inappropriate for the neonate. For example, Altman et al.(15) measured CVo2 in 11 babies using positron emission tomography and documented normal neurologic outcome in four babies with CVo2 values less than 1.3 mL·100 g-1 min-1. The aims of this study were to evaluate a noninvasive method for the assessment of CVo2 at the cotside using near infrared spectroscopy, and to investigate the relationship between gestational age and CVo2.
METHODS
CVo2 and CDo2 were calculated in micromoles·100 g-1 min-1 from: Equation 1,Equation 2 where CHbF is micromoles·100 g-1/min-1; Sao2 and CSvo2 are present.


To allow for comparison with previously published data, CVo2 was recalculated in milliliters·100 mL-1 min-1. Details of the derivation of Equations 1 and 2, and the method used to recalculate the CVo2 values in milliliters·100 mL-1 min-1 are explained in the "Appendix."
Sao2 was measured by pulse oximetry (Datex Satlite Trans, Datex, Finland). CSvo2 and CHbF were measured using NIRS (NIRO 500, Hamamatsu Photonics, UK).
NIRS was used to measure changes in cerebral concentrations of Hbo2 and Hb and total hemoglobin. The NIRS optodes were placed more than 4 cm apart in a frontotemporal or frontoparietal position determined by the size of the subject's head. A differential path length factor of 4.99 and a tissue density of 1.05 were used to quantify the data in micromoles/100 100 g(16). NIRS data were collected every half second. Pulse oximetry was performed with the oximeter operating in beat-to-beat mode. NIRS and pulse oximetry data were collected into a computer file using data logging software designed for the NIRO 500 (Onmain version 1.32). Subsequent analysis was performed using a computer spreadsheet package(Quattro Pro for Windows version 5.00, Borland International).
CSvo2 was calculated from the NIRS data obtained during partial jugular venous compression using a previously validated method(17). Unilateral partial jugular venous compression was applied for less than 10 s. CSvo2 was calculated from the NIRS data obtained during the first 5 s of the compression. Sao2 was taken as the mean of the 10 pulse oximetry measurements recorded during the first 5 s of venous compression. The NIRS data collected during each jugular venous compression were examined and were accepted as suitable for the calculation of CSvo2 if there was a stable baseline before the occlusion, a rise in the cerebral concentrations of both Hbo2 and Hb during the compression and a return to the same baseline after release of the compression.
CHbF (micromoles·100 g-1 min-1) was measured by NIRS using a technique in which a bolus of Hbo2 is delivered to the brain(18,19). The fraction of inspired O2 was increased to induce a rapid rise in Sao2. CHbF measurements were calculated from the data collected during the first 6 s of the rise in Sao2 and cerebral Hbo2 concentration. The NIRS and Spo2 data collected during each measurement of CHbF were also examined before the calculation of CHbF to determine their acceptability for calculation of CHbF. Spo2 data were accepted as suitable if Spo2 was less than 92% with a steady baseline before the measurement and there was a rise in Spo2 of greater than 5% over 6 s. NIRS data were accepted as suitable if there was a steady baseline for both Hbo2 and Hb before the measurement and the rise in Hbo2 was mirrored by a fall in Hb so that HbT remained constant through the study. CBF(milliliters·100 g-1 min-1) was calculated from the NIRS data by dividing the CHbF value by the arterial hemoglobin concentration(grams/mL) measured in each subject during each study.
Twenty babies were studied. A total of 48 CVo2 estimates were made with a median (range) of 2(1–5) estimates per subject. To assess the relationship with gestational age, the median value for CVo2, CDo2, and CSvo2 was taken for each subject. Correlations between gestational age and CVo2, CSvo2, and CDo2 were assessed by calculating Spearman's rank correlation coefficient (ρ). Correlations between CVo2 and both Paco2 and postnatal age were calculated using analysis of covariance to assess correlation within subjects(20), and a weighted correlation coefficient was calculated to assess correlation between subjects(21).
RESULTS
There were 9 male and 11 female infants studied. All were receiving intensive care. The median (range) gestation and birth weights were 27(24–41) wk and 1.1 (0.5-3.6) kg, respectively. Eight babies were sedated with morphine (200 µg/kg i.v. six hourly), two babies were receiving pancuronium, and one baby was receiving phenobarbitone (2.5 mg/kg 12 hourly) for previous seizures. None was having clinically apparent seizures at the time of the studies. Three babies had abnormal cranial ultrasound appearances at the time of the studies, including one who had a parenchymal hemorrhage. Thirty-five of the 48 studies were performed in the first 2 d of life, five more studies were performed between d 3 and 7, and the other eight were performed before d 21.
For each CVo2 estimation, CSvo2, Sao2, and CHbF were measured repeatedly over a 30-min period. A median (range) of 5(2–15) attempted measurements of CSvo2 and 4(2–8) attempted measurements of CHbF were made during each study. Not all attempted NIRS measurements met the predetermined success criteria. The median (range) success rates for CSvo2 and CHbF measurements in each subject were 82% (20-100%) and 75% (22-100%), respectively. The median number (range) of successful measurements of CSvo2 was therefore 4(2–10), and the median number(range) of successful CHbF measurements was 3(2–5) in each study. Mean values of CSvo2, Sao2, and CHbF obtained during each study were used to calculate the CVo2 estimate for that study.
The reproducibility of the estimate was assessed by calculating the coefficient of variation of each component measurement during each estimation. The median (interquartile range) coefficients of variation for CSvo2, Sao2, and CHbF were 4.9% (3-7.6%), 1.1% (0.5-2.8%), and 20.6% (10.5-28%), respectively.
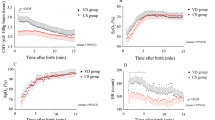
Table 1 shows the median (range) values for CHbF, CSvo2, Sao2, CBF, CDo2, and CVo2 from all 48 studies. There was a significant positive correlation between CVo2 and gestational age (n = 20, ρ = 0.55,p = 0.014) as shown in Figure 1. There was also a significant positive correlation between CDo2 and gestational(n = 20, ρ = 0.56, p = 0.012) as shown in Figure 2, but there was no significant correlation between CSvo2 and gestational age (n = 20, ρ =-0.041, p = 0.86).

Plot of the relationship between median CVo2 from each individual and gestational age.

Plot of the relationship between median CDo2 from each individual and gestational age.
There was no significant correlation between CVo2 and Paco2 either intersubject (r = 0.25, p > 0.1) or intrasubject(r = 0.5, p = 0.35). There was also no apparent correlation between CVo2 and postnatal age either intersubject(r = 0.1, p > 0.1) or intrasubject (r = 0.2,p = 0.33). There was no significant difference in CVo2 between the eight patients who were receiving morphine sedation and the 11 who were not receiving any sedation (p = 0.32, Mann-Whitney U test). The subject who was receiving phenobarbitone had a median value for CVo2 of 0.66 mL·100 g-1 min-1 and this is within the range of values seen in the other subjects. The values for CVo2 obtained in the three subjects with abnormal cerebral ultrasound appearances were also within the range of values seen in the other subjects and there was no significant difference between CVo2 in these three individuals and the rest of the subjects (p = 0.71, Mann-Whitney U test).
DISCUSSION
Previous studies of CVo2 in neonates have relied on invasive measurements with direct cannulation of the jugular bulb(22,23) or exposure to ionizing radiation during xenon-133 measurements of CBF(24) or positron emission tomography(15). We have described a noninvasive optical method for the estimation of CVo2 in neonates that can be performed at the cotside. The highest rates we observed were nine times greater than the lowest rates. We observed an increase in CVo2 with increasing gestational age, although there was only full-term baby in this study. There was no suggestion from this study that CVo2 was influenced by Paco2 or postnatal age, although the main aim of the study was not to test those hypotheses and it is possible that a study designed to address those specific questions may find otherwise. CVo2 was not obviously different in babies with abnormal cranial ultrasound scans but the number of babies with abnormal scans was small and it is likely that a larger study would be more conclusive. Similarly, CVo2 was not obviously different in babies who were receiving sedative drugs although the numbers of such babies in this study were too small for us to reach any definite conclusions about this.
The accuracy of the CVo2 estimate will be affected by a combination of the inaccuracies in each of the component measurements of Sao2, CSvo2, and CHbF. Each of these three separate measurements has been validated previously. Nearly all studies evaluating measurements of Sao2 by pulse oximetry in neonates have found pulse oximetry to be accurate to within ±2%(25). We have validated the method for measurement of CSvo2 by comparison with co-oximetry of blood from the jugular bulb and found close agreement, with a mean difference between NIRS and co-oximetry measurements of 1.5%(17). Measurements of CBF in neonates using NIRS have been validated by comparison with xenon-133 measurements(26,27). The measurement of CHbF is the measurement which caused the greatest inaccuracy in the estimate. The measurement shows the poorest reproducibility with a median coefficient of variation of 20.6%. This is similar to that noted in other studies which have used this particular NIRS method to measure blood flow(26,28,29).
The technique for CHbF measurement is not applicable to all sick neonates. To make the measurement it is necessary to induce a rapid rise in Sao2 by manipulation of the inspired oxygen concentration. This is not possible in babies with severe respiratory disease, or in babies who remain well oxygenated with low inspired oxygen concentrations. This is a major limitation of the technique. Alternative NIRS techniques for blood flow measurement, such as injecting indocyanine green(30) will be more widely applicable and may show better repeatability.
The quantification of NIRS data for the calculation of hemoglobin flow or blood flow requires accurate knowledge of the optical path length. This is calculated by multiplying the distance between the two NIRS optodes by a"differential path length factor" to account for scattering of light within the tissues. The differential path length factor of 4.99 used in this study was obtained from measurements made in neonates using phase resolved spectroscopy(16). However, other studies have measured the differential path length factor from the time of flight of picosecond pulses of light and have produced different, although similar, values(31,32). It is likely that the optical characteristics of each baby's brain will be different and whichever differential path length factor is used, it can be considered only as an estimate. This problem could be resolved by performing NIRS with real time measurements of optical path length which may be possible as the technology develops.
Ignoring dissolved oxygen undoubtedly leads to an underestimation of CVo2. Across the range of hemoglobin concentrations and oxygen tensions seen in the subjects of this study, less than 1% of the oxygen carried in the blood would be dissolved rather than bound to hemoglobin, and the underestimate will therefore be small.
The measurement of CSvo2 by NIRS with jugular venous compression is easily performed on neonates undergoing intensive care. It causes no apparent distress to the babies and no change in the heart rate or the arterial saturation as measured by pulse oximetry (our unpublished observations). Bilateral jugular venous occlusion has been used to measure CBF in these babies using strain gauge plethysmography and electrical impedance(33–35). An increase in the risk of intracranial hemorrhage has not been reported with these methods. We have observed that the change in cerebral blood volume which occurs during unilateral jugular compression is less than that which occurs during an unsynchronized expiration by a mechanically ventilated infant. Abolition of such unsynchronized expirations by neuromuscular paralysis during mechanical ventilation has not been shown to reduce the risk of intraventricular hemorrhage. It is highly unlikely that the measurement of CSvo2 by NIRS with unilateral jugular venous compression will increase the risk of intraventricular hemorrhage.
The values for CVo2 obtained in this study are comparable with the few published measurements of CVo2 in neonates obtained by more invasive methods. Garfunkel et al.(22) measured CVo2 in 33 children including three term neonates with severe brain abnormalities. CVo2 in these babies was between 1.1 and 2.1 mL·100 g-1 min-1. Frewen et al.(23) measured CBF, Cao2, and CSvo2 from the internal jugular vein in a group of nine term babies with hypoxic ischemic encephalopathy. Although they did not report CVo2 values for individual subjects, CVo2 calculated from the mean values for Cao2, CSvo2, and CBF gave values of 1.7 mL·100 g-1 min-1 in normal survivors and 1.3 mL·100 g-1 min-1 in babies who died or survived with severe brain damage. The first published measurements of CVo2 in preterm neonates were those reported by Skov et al.(24) who used xenon-133 to measure CBF, and NIRS with head tipping to measure CSvo2. That group reported a value of 1.4 mL·100 g-1 min-1 in 10 asphyxiated term babies and a lower value of 1.0 mL·100 g-1 min-1 in nine preterm babies with hyaline membrane disease. Altman et al.(15) measured CVo2 using positron emission tomography and reported CVo2 to be between 0.4 and 1.3 mL·100 g-1 min-1 in six term babies, four of whom had hypoxic ischemic encephalopathy, and values of 0.06-0.54 mL·100 g-1 min-1 in five preterm babies.
Most of the CVo2 estimates obtained in this study were considerably lower than the value of 1.3 mL·100 g-1 min-1, which has been reported as the lower limit for brain viability in adults, and lower values were seen in babies with a lower gestational age. The reason for the neonatal values of CVo2 being lower than adult values is likely to be due to the changes in the structural complexity and functional activity of the brain which occur across the range of gestational ages studied. There is an enormous change in the architecture of the cerebrum, with an increase in the number of neurones and in the number of synapses(36). This increase in the structural complexity is accompanied by an increase in functional activity as evidenced by electroencephalography(37). It is not surprising then that the oxygen demand of the brain increases with increasing brain maturity during this period. Measurements of CVo2 in fetal sheep have shown a similar rise with increasing maturity(38). This is the first study to show such a relationship in the human in vivo, although Himwich et al.(39) described a similar relationship from in vitro work using minced brain samples obtained from recently dead fetuses and babies.
The demand for other metabolic fuels also increases during the process of cerebral maturation. In a recent positron emission tomography study, Kinnala et al.(40) demonstrated an increase in cerebral glucose consumption with increasing postconceptional age. In that study the mean value for the rate of cerebral glucose consumption between 32 and 34 wk was 5.5 µmol·100 g-1 min-1. In our study, the mean CVo2 for the four infants between 32 and 34 wk was 31.47µmol·100 g-1 min-1. The ratio of oxygen to glucose consumption calculated from these two values is 5.7 µmol of oxygen for each µmol of glucose. This is similar to the ratio reported in the adult human brain(41–44). This calculation lends further support to our estimates of CVo2 being of the correct magnitude.
Examination of the published data suggests that CVo2 continues to increase through childhood. Figure 3 shows CVo2 measurements obtained from several studies in various different groups of older children(15,22–24,45–48). The details of these studies are shown in Table 2. Most of the children in these studies were anesthetized or sedated, and many were undergoing intensive care; there are few published data from healthy, stable children. The value of 5.17 mL·100 g-1 min-1 obtained by Kennedy and Sokoloff(48) from a group of children with a median age of 6.1 y is higher than the values of 3.2-3.7 mL·100 g-1 min-1 typically seen in healthy adults(6–12). The values obtained by Kennedy and Sokoloff were from invasive methods, including cannulation of the jugular bulb, in unsedated children in whom cooperation was achieved by allowing them to watch "moving pictures." The anxiety caused by the procedures or the increased arousal from watching the moving pictures may have artificially elevated the CVo2 in these children. However, Chugani et al.(49) have demonstrated that cerebral glucose consumption increases through early childhood to a maximum value at about 8-9 y of age and subsequently falls slowly with the approach of adulthood. From this observation it may be expected that CVo2 would show a similar pattern of change with age through childhood, and the high values reported by Kennedy and Sokoloff may be representative of this. Later in adult life there is evidence that CVo2 decreases with aging after the age of 20 y(50,51).

Plot of mean CVo2 against mean age from studies measuring CVo2 in children. The open circle represents this study, closed circles represent data from the studies in Table 2.
There was an increase in CDo2 with increasing gestational age, but no change in CSvo2. This suggested that the increased oxygen demands of the maturing brain were met by increasing the rate of oxygen delivery, rather than by increasing the proportion of available oxygen which is extracted from the circulation.
We have shown the feasibility of estimating CVo2 in sick neonates at the cotside using noninvasive, optical methods. The values obtained were similar to those obtained, by more invasive techniques, in other studies and are in agreement with values which we would expect from the known rate of cerebral glucose consumption in neonates. There is an increase in CVo2 with increasing brain maturity and it is likely that this increase continues through childhood. The increasing oxygen demands of the brain with maturation are met by an increase in CDo2.
Abbreviations
- Cao 2 :
-
arterial oxygen content
- CBF :
-
cerebral blood flow
- CDo 2 :
-
cerebral oxygen delivery
- CHbF :
-
cerebral hemoglobin flow
- CSvo 2 :
-
cerebral venous oxyhemoglobin saturation
- Cvo 2 :
-
venous oxygen content
- CVo 2 :
-
cerebral oxygen consumptiony
- Hb :
-
deoxyhemoglobin
- Hbo 2 :
-
oxyhemoglobin
- [Hb] :
-
hemoglobin concentration in the blood
- NIRS :
-
near infrared spectroscopy
- Sao 2 :
-
arterial oxyhemoglobin saturation
- So 2 :
-
oxyhemoglobin saturation
- Spo 2 :
-
arterial oxyhemoglobin saturation by pulse oximetry
- Svo 2 :
-
venous oxyhemoglobin saturation
References
Wyatt JS, Edwards AD, Azzopardi D, Reynolds EOR 1989 Magnetic resonance and near infrared spectroscopy for investigation of perinatal hypoxic-ischemic brain injury. Arch Dis Child 64: 953–963.
Van Bel F, Dorrepaal CA, Benders MJNL, Zeeuve PEM, van der Bor M, Berger HM 1993 Changes in cerebral hemodynamics and oxygenation in the first twenty four hours after birth asphyxia. Pediatrics 92: 365–372.
Matcher SJ, Elwell CE, Cooper CE, Cope M, Delpy DT 1995 Performance comparison of several published tissue near-infrared spectroscopy algorithms. Anal Biochem 227: 54–68.
Gagnon RE, Gagnon FA, Macnab AJ 1996 Identification of software errors in near infrared spectroscopic measurement of changes in oxidised cytochrome aa3. Eur J Appl Physiol 74: 487–495.
Marks KA, Mallard EC, Roberts I, Williams CE, Sirimanne ES, Johnstone B, Gluckman PD, Edwards AD 1996 Delayed vasodilation and altered oxygenation after cerebral ischaemia in fetal sheep. Pediatr Res 39: 48–54.
Madsen PL, Vorstrup S, Schmidt JF, Paulson OB 1990 Effect of acute and prolonged treatment with propranolol on cerebral blood flow and cerebral oxygen metabolism in healthy volunteers. Eur J Clin Pharmacol 39: 395–297.
Schmidt JF, Waldemar G, Paulson OB 1990 The acute effect of captopril on cerebral blood flow, its CO2 reactivity, and cerebral oxygen metabolism in human volunteers. J Cardiovasc Pharmacol 16: 1007–1010.
Jakobsen J, Schmidt JF, Waldemar G, Paulson OB 1990 The acute effect of dilevalol on cerebral blood flow and oxygen consumption in normotensive humans. J Cardiovasc Pharmacol 15: 574–578.
Madsen PL, Schmidt JF, Holm S, Vorstrup S, Lassen NA, Wildschiodtz G 1991 Cerebral oxygen metabolism and cerebral blood flow in man during light sleep (stage 2). Brain Res 557: 217–220.
Hino A, Ueda S, Mizukawa N, Imahori Y, Tenjin H 1992 Effect of haemodilution on cerebral haemodynamics and oxygen metabolism. Stroke 23: 423–426.
Madsen PL, Schmidt JF, Holm S, Jorgensen H, Wildschiodtz G, Christensen NJ, Friberg L, Vorstrup S, Lassen NA 1992 Mental stress and cognitive performance do not increase overall level of cerebral O2 uptake in humans. J Appl Physiol 72: 420–426.
Madsen PL, Holm S, Herning M, Lassen NA 1993 Average blood flow and oxygen uptake in the human brain during resting wakefulness: a critical appraisal of the Kety-Schmidt technique. J Cereb Blood Flow Metab 13: 646–655.
Baron JC, Rougemont D, Bousser MG, Lebrun-Grandie P, Iba-Zizan MT, Chivas JC 1983 Local CBF, oxygen extraction fraction and CMRO2: prognostic value in recent supratentorial infarction. J Cereb Blood Flow Metab 3( suppl 1): s1–s3.
Powers WJ, Grubb RL, Darriet D, Raichle ME 1985 Cerebral blood flow and cerebral metabolic rate of oxygen for cerebral function in humans. J Cereb Blood Flow Metab 5: 600–608.
Altman DJ, Perlman JM, Volpe JJ, Powers WJ 1993 Cerebral oxygen metabolism in newborns. Pediatrics 92: 99–104.
Duncan A, Meek JH, Clemence M, Elwell C, Tyszczuk L, Cope M, Delpy DT 1995 Optical pathlength measurements on adult head, calf and forearm and the head of the newborn infant using phase resolved spectroscopy. Phys Med Biol 40: 295–304.
Yoxall CW, Dawani N, Weindling AM, Peart I 1995 Measurement of cerebral venous oxyhaemoglobin saturation in children by near infrared spectroscopy and partial jugular venous occlusion. Pediatr Res 38: 319–323.
Edwards AE, Wyatt J, Richardson C, Delpy DT, Cope M, Reynolds EOR 1988 Cotside measurement of cerebral blood flow in ill newborn infants by near infrared spectroscopy. Lancet 2: 770–771.
Edwards AD, Richardson C, Van der Zee P, Elwell C, Wyatt JS, Cope M, Delpy DT, Reynolds EOR 1993 Measurement of haemoglobin flow and blood flow by near infrared spectroscopy. J Appl Physiol 75: 1884–1889.
Bland JM, Altman DG 1995 Calculating correlation coefficients with repeated observations. 1. Correlation within subjects. BMJ 310: 446
Bland JM, Altman DG 1995 Calculating correlation coefficients with repeated observations. 2. Correlation between subjects. BMJ 310: 633
Garfunkel JM, Baird HW, Zeigler J 1954 The relationship of oxygen consumption to cerebral functional activity. J Pediatr 44: 64–72.
Frewen TC, Kissoon N, Kronick J, Fox M, Lee R, Bradwin N, Chance G 1991 Cerebral blood flow, cross brain oxygen extraction and fontanelle pressure after hypoxic-ischaemic injury in newborn infants. J Pediatr 118: 265–271.
Skov L, Pryds O, Greisen G, Lou H 1993 Estimation of cerebral venous saturation in newborn infants by near infrared spectroscopy. Pediatr Res 33: 52–55.
Fanconi S, Tschupp A 1994 Accuracy of a new transmittance-reflectance pulse oximetry sensor in critically ill neonates. Crit Care Med 22: 1142–1146.
Skov L, Pryds O, Greisen 1993 Estimating cerebral blood flow in newborn infants: comparison of near infrared spectroscopy and133 Xe clearance. Pediatr Res 30: 570–573.
Bucher HU, Edwards AD, Lipp AE, Duc G 1993 Comparison between near infrared spectroscopy and 133Xe clearance for estimation of cerebral blood flow in critically ill, preterm infants. Pediatr Res 33: 56–60.
Edwards AD, Wyatt JS, Richardson CE, Delpy DT, Cope M, Reynolds EOR 1989 Precision of cerebral blood flow measurement by near infrared spectroscopy. Pediatr Res 26: 520
Brun N, Greisen G 1994 Cerebrovascular responses to carbon dioxide as detected by near infrared spectrophotometry: comparison of three different measures. Pediatr Res 36: 20–24.
Roberts I, Fallom P, Kirkham FJ, Lloyd Thomas A, Cooper C, Maynard R, Elliott M, Edwards AD 1993 Estimation of cerebral blood flow with near infrared spectroscopy and indocyanine green. Lancet 342: 1425
Wyatt JS, Cope M, Delpy DT, van der Zee P, Arridge SR, Edwards AD, Reynolds EOR 1990 Measurement of optical pathlength for near infrared spectroscopy in newborn infants. Dev Neurosci 12: 140–144.
Van der Zee P, Cope M, Arridge AR, Essenpreis M, Potter LA, Edwards AD, Wyatt JS, McCormick DC, Roth SC, Reynolds EOR, Delpy DT 1992 Experimentally measured optical pathlengths for the adult head, calf and forearm and the head of the newborn infant as a function of interoptode spacing. Adv Exp Med Biol 316: 143–153.
Cooke RW, Rolfe P, Howat P 1977 A technique for estimation of cerebral blood flow in the newborn infant. J Med Eng Technol 1: 263–266.
Cross KW, Dear PR, Hathorn MK, Hyams A, Kerslake DM, Milligan DW, Rahilly PM, Stothers JK 1979 An estimation of cerebral blood flow in the newborn infant. J Physiol 289: 329–345.
Weindling AM, Rolfe P, Tarassenko L, Costeloe K 1983 Cerebral haemodynamics in newborn babies studied by electrical impedance. Preliminary results. Acta Paediatr Suppl 311: 14–19.
England MA 1995 Anatomical development of the central nervous system. In Levene MI, Lilford RJ (eds) Fetal and Neonatal Neurology and Neurosurgery. Churchill Livingstone, Edinburgh, 3–27.
Koyangi T, Nakano H 1995 Functional development of the fetal nervous system. In Levene MI, Lilford RJ (eds) Fetal and Neonatal Neurology and Neurosurgery. Churchill Livingstone, Edinburgh, 31–44.
Gleason CA, Hamm C, Jones MD 1989 Cerebral blood flow, oxygenation, and carbohydrate metabolism in immature fetal sheep in utero. Am J Physiol 256:R1246–R1268.
Himwich WA, Benaron HB, Tucker BE, Babuna C, Stripe MC 1959 Metabolic studies on perinatal human brain. Physiol 14: 873–877.
Kinnala A, Suhonen-Polvi H, Äärimma T, Kero P, Korvenranta H, Ruotsalainen U, Bergman J, Haaparanta M, Solin O, Nuutila P 1996 Cerebral metabolic rate for glucose during the first six months of life: an FDG positron emission tomography study. Arch Dis Child 74: 153–157.
Seisjo BK 1978 Brain Energy Metabolism. John Wiley& Sons, New York, 103–106.
Frackowiak RSJ, Herold S, Petty RKH, Morgan-Hughes JA 1988 The cerebral metabolism of oxygen and glucose measured by positron emission tomography in patients with mitochondrial diseases. Brain 111: 1009–1024.
Ogawa M, Fukuyama H, Ouchi Y, Yamauchi H, Kimura J 1996 Altered energy metabolism in Alzheimers disease. J Neurol Sci 139: 78–82.
Madsen PL, Hasselbalch SG, Hageman LP, Olsen K, Persistent resetting of the cerebral oxygen/glucose uptake ratio by brain activation: evidence obtained with the Kety-Schmidt technique. J Cereb Blood Flow Metab 15: 485–491.
Greeley WJ, Bracey VA, Ungerleider RM, Griebel JA, Kern FH, Boyd JL, Reves JG, Piantadosi CA 1991 Recovery of cerebral metabolism and mitochondrial oxidation state is delayed after hypothermic circulatory arrest. Circulation 84: suppl III 400–406.
Settergren G, Lindblad BS, Persson B 1976 Cerebral blood flow and exchange of oxygen, glucose, ketone bodies, lactate, pyruvate and amino acids in babies. Acta Paediatr Scand 65: 343–353.
Connors R, Frewen TC, Kissoon N, Kronick J, Sommeraur J, Lee R, Singh N, Tiffin N, Brown T 1992 Relationship of cross-brain oxygen content difference, cerebral blood flow and metabolic rate to neurologic outcome after near drowning. J Pediatr 121: 839–844.
Kennedy C, Sokoloff L 1957 An adaptation of the nitrous oxide method to the study of the cerebral circulation in children; normal values for cerebral blood flow and cerebral metabolic rate in childhood. J Clin Invest 36: 1130–1137.
Chugani HT, Phelps ME, Mazziotta JC 1987 Positron emission tomography study of human brain functional development. Ann Neurol 22: 487–497.
Marchal G, Rioux P, Petit-Taboue MC, Sette G, Travere JM, LePoec C, Courtheoux P, Derlon JM, Baron JC 1992 Regional cerebral oxygen consumption, blood flow and blood volume in healthy human aging. Arch Neurol 49: 1013–1020.
Vaz M Rajkumar C Wong J Mazzeo RS Turner AG Cox HS Jennings GL Esler MD 1996 Oxygen consumption in the heart, hepatomesenteric bed and brain in young and elderly human subjects and accompanying sympathetic nervous activity. Metabolism 45: 1487–1492.
Author information
Authors and Affiliations
APPENDIX
APPENDIX
CDO2 and CVO2 can be calculated from the standard equation Equation A1, Equation A2 where CDO2 is milliliters of O2·100 g of brain-1 min-1, CBF is milliliters of blood·100 g of brain-1 min-1), CaO2 is milliliters of O2/mL of blood, CVO2 is milliliters of O2·100 g of brain-1 min-1, and CvO2 is milliliters of O2/mL of blood.


The oxygen content of blood (milliliters of O2/mL of blood) can be calculated from: Equation A3 or, Equation A4 where [Hb] = grams/mL, SO2 = percentage HbO2 saturation, 1.39 = the stoichiometric value of oxygen for hemoglobin (milliliters/g), PO2 = partial pressure of O2 (mm Hg), and 0.00003 = coefficient of oxygen solubility(milliliters of O2/mL of blood).


Within the range of hemoglobin concentrations seen in neonates, at physiologic oxygen tensions approximately 99% of the oxygen in the blood is carried bound to hemoglobin. Dissolved oxygen can therefore be reasonably disregarded in the calculation of blood oxygen content. Blood oxygen content can therefore be calculated from: Equation A5 CDO2 and CVO2 can then be calculated by rearrangingEquations A1, A2, and A5Equation A6, Equation A7 where CHbF is grams of hemoglobin·100 g of brain-1 min-1, SaO2 and CSvO2 are percent.



Because each molecule of hemoglobin binds 4 molecules of O2, if the concentration of hemoglobin in blood is expressed in micromoles/mL, the blood oxygen content can be calculated in micromoles/mL using a modification of Equation A5: Equation A8 CDO2 and CVO2 can then be calculated in micromoles·100 g-1 min-1 from:Equation A9, Equation A10



To express CVO2 in milliliters of O2·100 mL of brain-1 min-1, the CHbF value was converted to grams·100 mL-1 min-1 from:Equation A11 where 64 500 = molecular weight of hemoglobin (grams/mol).

CVO2 and CDO2 were then recalculated in milliliters/100 g/min using Equations A6 and A7.
Rights and permissions
About this article
Cite this article
Yoxall, C., Weindling, A. Measurement of Cerebral Oxygen Consumption in the Human Neonate Using Near Infrared Spectroscopy: Cerebral Oxygen Consumption Increases with Advancing Gestational Age. Pediatr Res 44, 283–290 (1998). https://doi.org/10.1203/00006450-199809000-00004
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199809000-00004
This article is cited by
-
Proteomic phenotype of cerebral organoids derived from autism spectrum disorder patients reveal disrupted energy metabolism, cellular components, and biological processes
Molecular Psychiatry (2022)
-
Brain Oximetry and the Quest for Quantified Metabolic Rate: Applications Using MRI and Near-Infrared Spectroscopy
Applied Magnetic Resonance (2021)
-
Elevated brain oxygen extraction fraction in preterm newborns with anemia measured using noninvasive MRI
Journal of Perinatology (2018)
-
Investigating the effects of cerebrospinal fluid removal on cerebral blood flow and oxidative metabolism in infants with post-hemorrhagic ventricular dilatation
Pediatric Research (2017)
-
Magnetic resonance imaging based noninvasive measurements of brain hemodynamics in neonates: a review
Pediatric Research (2016)
