
Abstract
The corrected midparental height method was introduced by Tanner in 1970 (Tanner method) and is commonly used to estimate target height in children to evaluate the effectiveness of growth-promoting therapies. It has not been established if the equation used to compute target height should be the same for children with short, normal, or tall parents. In this study, we examined the predicted target height values by parental heights in a large population-based study (n = 2402). A simple linear function of midparental height (x) was proposed to estimate target height (y): y = 45.99 + 0.78x (boys), y = 37.85+0.75x (girls), with a 95% predicted interval of about ±10 cm. The prediction model was similar for boys and girls in SD scores (SDS), and was not affected by assortative mating or difference in parental heights. The model may underestimate the potential stature by about 2 cm for children with midparental height below -2 SDS, or 163 cm. In comparison, the Tanner method may lead to a 6-cm error in underestimating target height for these children. The function would be a better choice than the Tanner method for estimating target height in the clinical evaluation of growth promotion treatments because it is common that short children also have short parents. Children with very short parents will usually be much taller than their parents in adult stature, and we believe that a different function should be developed. The results support the proposed nondominant, non-sex-linked, polygenic inheritance in stature. The estimated heritability values were 0.75-0.78 in cm or 0.55-0.60 in SDS.
Similar content being viewed by others

Main
Height is commonly recognized as a polygenic trait and is subject to both genetic and environmental influences (1–5). Previous studies on the influence of parental genetics on stature were based on observations on children born in the 1960s or earlier, and only a few studies have examined final height (2–12). The reported correlation coefficient between parental heights and the final height of the offspring varies from 0.4 to 0.6, whereas the reported heritability value ranges from 0.5 to 0.9. Almost all of these studies were based on normal healthy children, and little is known about the genetic potential in stature for children with short or tall parents.
The fact that the height of a child is related to parental heights is often used in the clinic to evaluate children in growth-promoting therapies (13–17). The genetic potential height, or target height, is commonly determined by the corrected midparental height method (adding or subtracting about 6.5 cm for boys or girls, respectively) that was introduced by Tanner et al. (18). It has not yet been resolved if the function for predicting target height should be the same for children with short, normal, or tall parents, nor if the prediction is influenced by the degree of similarity or dissimilarity between the two parents in height. The aim of this study was to analyze the relationship between final height and parental height for predicting target height in a large sample (n = 2402) of normal Swedish children who were born in the 1970s and to examine the prediction model in detail.
METHODS
The children included in this study were from a Swedish population-based growth study that has been described in detail elsewhere (19,20). A total of 3650 full-term healthy children with complete study records were included from the total study population of 5111 children who were in the last grade of school in 1992 in Göteborg, Sweden. All health and growth records from birth to the last grade in school were obtained. At the visit to the school, weight and height of the children were measured in a standardized way with a calibrated Harpenden stadiometer. Their parents were asked to report their current height and weight in connection with signing the written informed consent form. Children who had gained less than 0.5 cm during the past year and who had reached the age at peak height velocity at least 2 y before the last examination were considered to have reached final height. Children without data available on final height and/or parental height were omitted from the present analysis, which left 2402 children available for analyses. Midparental height was calculated as the average of father's and mother's height. Parental heights and final height were all converted into SDS. The height reference values used here consist of parental heights examined in this study and the height of the children in the total sample. The heritability value was taken as the regression coefficient between final height and midparental height (21).
Statistical analyses used scatter plots, curve-fitting by single linear and second or third degree polynomial function. The 95% CI of the regression coefficient was calculated as β ± t1-α/2·SE(β) (22). The goodness of fit for the regression functions was determined by analyzing the mean and SD of the residual values. The 95% CI for the mean residual values was computed as m ± 1.96·SE(m), whereas the 95% CI for residual SD was calculated as the square root of (S2/F0.025:n-1,∞ S2/F0.975:n-1,∞) (23). A t test was used to test the difference between the two groups and for one group with the expected mean value of zero. Skewness and kurtosis values (H0: value = 0, for n = 1200, expected skewness value ± 0.12, expected kurtosis value <0.24; for n = 2500 expected skewness value ±0.08, expected kurtosis value <0.16) were computed to evaluate the normality of the data (24). All statistics were computed by SAS (25). The data from two other Swedish pediatric growth studies were used to evaluate the validity of parental height values in the present study (26,27).
RESULTS
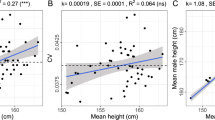
The mean and SD values of parental heights and final height for the total and the subsample used in this analysis are given in Table 1. A minor increase in height could be noted over the two generations, 0.7 cm in male and 1.0 cm in female subjects. The mean and SD of final height SDS in the children selected were not statistically different from these values in children not included (t test, p > 0.05). The correlation coefficient is 0.27 between father's height and mother's height, 0.48 between final height and father's height, 0.47 between final height and mother's height, 0.59 between final height and midparental height (the values are almost the same for boys and girls). The mean height of parents is almost the same as that of Swedes born in the 1950s (26). Similar correlation coefficients between final height and parental heights could be obtained using the data from another Swedish pediatric growth study (27), i.e. 0.61 between final height and midparental height.
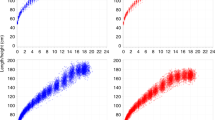
Figure 1 depicts the scatter plots of final height by different expressions of parental height (father's height, mother's height, or midparental height) in SDS. The figure also includes the linear regression, the 95% CI of the means (m ± 1.96·SE(m)), and the 95% CI of the predicted values (m ± 1.96·SD). The slopes and shapes of these plots were quite similar. No increased R2 could be noted when a nonlinear regression, i.e. a second or a third degree polynomial function was applied to the series. The simple linear function was found to be adequate for describing the final height relationship with parental heights.

Scatter plot of final height SDS by different expressions of parental height SDS. The interpolation includes the simple linear regression line, the 95% CI of the mean (middle dashed lines) and the 95% CI of the predicted values (peripheral dashed lines).
Table 2 includes the parameters for estimating target height by various linear functions of parental heights in SDS and centimeters. For both sexes, the R2 of the regression model was highest (0.36-0.37) when midparental height was included rather than the mother's or father's height. The higher predictive value of midparental height was also reflected by a lower residual final height SD value of 0.70 or 0.81 SDS for girls or boys, respectively, leading to a 95% CI of about ±1.5 SDS, or ±10 cm. The intercepts of all functions are virtually zero (in SDS), which implies that the intercepts could have been omitted from the regression. The slopes (β) are between 0.42 and 0.60. Based on final height regression coefficients to midparental height, the estimated heritability value is 0.75-0.78 in cm or 0.55-0.60 in SDS.
The 95% CIs of the regression coefficients of final height by father's height and mother's height are approximately the same in any group. The 95% CI of the regression coefficient is also similar for boys and girls in any of the three parental height SDS expressions (Table 2). There was no change in the R2 values when the SDS was replaced by centimeters in units. The intercept varied from 37.85 to 95.44 cm, and the residual SD value ranged from 4.86 to 5.94 cm in different models (Table 2). The least residual SD values were obtained when the midparental height was included as the independent variable, leading to a 95% CI of 9.72 and 10.70 cm for girls and boys, respectively.
The distribution of the residual final height SDS showed a positive skewness for boys and a negative skewness for girls (p < 0.05), but is normal when the two sexes are combined (Table 3). If three outliers (one boy, two girls) are excluded, all skewness and kurtosis values fall within normal ranges. The goodness of fit was also determined by the distribution of the residual values for one of the regression models, the midparental height SDS for both sexes individually and combined. The mean residual values were computed for the residual values over a 0.5 integer of midparental height SDS, and the results are shown in Table 3 and Figure 2. The mean residual value for estimating target height by midparental height show some fluctuation around the zero line, but are significantly (p < 0.05) above zero for children with midparental height below -2 SDS, or 163 cm. For boys with midparental height below -2 SDS, the mean of final height and the mean of estimated target height were 12.5 and 10.5 cm above midparental height, respectively (2-cm error). Similar results could be obtained for girls.

Mean residual final height SDS (with 95% CI) for various groups of midparental height ranges. The predicted target height was computed by the midparental height functions in Table 2.
We also analyzed the mean residual final height SDS values over the range of the difference between father's and mother's height, and the results were shown in Figure 3. There was no tendency for the predicted target height to be different for parents with similar height SDS compared with parents with different height SDS. The 95% CI for the mean of residuals varied slightly around the zero line in a similar fashion for boys, girls, and combined. The residual final height values over the range of final height SDS are depicted in Figure 4. The positive linear trend is apparent. The residual values are increasing for children with increasing final height.

Mean residual final height SDS (with 95% CI) for various groups of difference in parental heights (father's height SDS minus mother's height SDS). The predicted target height was computed by the midparental height functions in Table 2.

Mean residual final height SDS (with 95% CI) for various groups of children in final heights. The predicted target height was computed by the midparental height functions in Table 2.
The 95% CI for residual final height SD is given over the range of midparental height SDS in Figure 5, and over the range of difference in parental height (father's height SDS minus mother's height SDS) in Figure 6. These revealed that the residual SD was fairly constant over both the ranges of midparental height and the difference in parental heights.

Residual final height SD (with 95% CI) for various groups of midparental height SDS. The predicted target height was computed by the midparental height functions in Table 2.

Residual final height SD (with 95% CI) for various groups of difference in parental height (father's height SDS minus mother's height SDS). The predicted target height was computed by the midparental height functions in Table 2.
DISCUSSION
This is the first large population-based study of parental impact on stature for children born in the 1970s, because the surveyed children of previous studies were born in the 1960s or earlier (2–12). The increase in height over generations was only 0.7 cm for male and 1.0 cm for female subjects, much less than the increase observed in other populations (3–8). The series can be seen as an ideal one for examining the final height relationship with parental heights as no real secular change in height occurred over generations as occurred in other studies (3–12). The final height measurement was reliable because all children were measured in a standardized way by the study team (19). The parental heights are self-reported and may reflect little error. It should be noted that most Swedish adults knew their measured heights from health checkups. The validity of the reported parental heights is also verified by the fact that the mean and SD of the parental heights here are very close to the reference values for the Swedes born in the same decade (26). Similar correlation coefficients between final height and parental heights could be obtained using the data from another Swedish growth study with parental heights being carefully measured (27).
The intercepts (α), slopes (β), as well as R2 were similar for boys and girls in the linear functions of final height by any expression of parental height SDS for estimating target height. The regression slopes were also similar between final height SDS by father's height SDS and final height SDS by mother's height SDS. The result supports the proposed non-sex-linked, nondominant, polygenic model of inheritance for human stature (1,21). Inasmuch as there are several ways to calculate the heritability value, results from different studies may not be comparable. The method used here expresses the heritability value in terms of the regression coefficient between final height and midparental height (21). The estimated heritability value we found ranges from 0.55 to 0.60 in SDS or 0.75 to 0.78 in cm, the former value is similar to that of Solomon and Thompson (8), whereas the latter is similar to results from other published studies (2–7). We have estimated the heritability value in both SDS and centimeters, whereas most previous studies used centimeters or inches (2–10). It should be noted that the estimated heritability value would be different if heights in centimeters were converted into SDS.
The goodness of fit for estimating target height by midparental height (R2 = 0.36-0.37) is better than that achieved by using either the father's or mother's height (R2 = 0.21-0.25). As an indicator of genetic potential height, midparental height could account for one-third of the total variation and is better than either father's or mother's height. The 95% CI of the estimated target height by midparental height in our model is about ±1.5 SDS, or ±10 cm, approximately 3-4 cm wider than the 95% CI of commonly applied final height prediction methods (±6 to ±7 cm) which need several additional variables (28–30). Estimates of target height (y) by midparental height (x) in centimeters can be taken from Table 2, y = 45.99 + 0.78x (boys), y = 37.85 + 0.75x (girls).
The distributions of the mean of residuals and residual SD for estimating target height by midparental height SDS were rather constant over the range of midparental height of difference in parental heights except for children with very short parents. Neither midparental height nor the difference in parental height affects the residual values. Thus, the predictive accuracy was not affected by assortative mating, although the correlation coefficient between the two parents was 0.27 (an indication of assortative mating). We cannot make any comparison with other study findings because there have been no reports on the influence of difference in parental height on a child's target height. The higher residual values for children who were taller could be explained by the regression to the mean phenomenon.
The corrected midparental height method (adding or subtracting about 6.5 cm for boys or girls, respectively) for estimating target height was introduced by Tanner in 1970 (Tanner method) and is widely used by pediatric endocrinologists (14–18). If the Tanner method was used to estimate target height for the Swedish series, the mean residual would be significantly above the expected value of zero (mean = 0.16 SDS, p < 0.01). Figure 7 shows the estimated target height by the two methods (Tanner method and our model; the midparental functions in Table 2). The difference in the estimated target height by the two methods is within ±2 cm for midparental height above -1 SDS and below 2 SDS. The estimated target height by the Tanner method may be 4 cm below the target height estimated by our model for children with midparental height below -2 SDS, or 163 cm. The Tanner method will lead to a 6-cm bias in underestimating target height for children with midparental height below -2 SDS because the underestimation in our model for these children is 2 cm. Because it is common that short children also have short parents, it would be a common mistake to apply the Tanner method in the clinics as well as in growth-promoting studies. The dimensions in underestimating target height for these children by the Tanner method is too large to be acceptable, and our model would be a better choice.

Estimated target height and its difference between the corrected midparental height method of Tanner (triangle) and the midparental height functions given in Table 2 (black dots) for boys (solid lines) and girls (dashed lines).
There are still no reports on predicting target height for children with midparental height below -2 SDS. We could not propose a function for estimating target height for these children with very short parents because of the relatively small sample size in this category (25 boys, 29 girls). But, it could be noted that the error in underestimation is much smaller in our model (2 cm) than in the Tanner method (6 cm). The analyses indicate that we should be careful in estimating the target height of a child with short parents. The adult statures of the short parents may be far below their genetic potentials. It is possible that disease, malnutrition, or other nonhereditary events occurring in early childhood may account for the shortness of these parents, but will not impair their genetic potential for their offspring. Usually, children with very short parents will be much taller than their parents in adult stature. A different model should preferably be developed to estimate target height for these children.
We here propose that the midparental height functions shown in Table 2 could be used to estimate target height, with a 95% predicted interval of about ±10 cm. The prediction model is almost the same for boys and girls in SDS, and will not be affected by assortative mating. The predicted target height could also be read directly from the lower panel in Figure 7. The target height prediction model presented here represents a better choice than the currently applied method, i.e. the corrected midparental height method.
Abbreviations
- SDS:
-
SD score
- CI:
-
confidence interval
REFERENCES
Preece MA 1996 The genetics contribution to stature. Horm Res 45( suppl 2): 56–58
Pearson K, Lee A 1903 On the laws of inheritance in man. Biometrika 2: 359–372
Tanner JM, Israelsohn W 1963 Parent-child correlations for body measurements of children between the ages of one month and 7 years. Ann Hum Genet 26: 245–253
Mueller WH 1976 Parent-child correlations for stature and weight among school aged children. A reveiw of 24 studies. Hum Biol 48: 379–397
Susanne C 1975 Genetic and environmental influences on morphological characteristics. Ann Hum Biol 2: 279–287
Roberts DF, Billewicz WZ, McGregor IA 1978 Heritability of stature in a West African population. Ann Hum Genet 42: 15–24
Kaur DP, Singh R 1981 Parent-adult offspring correlations and heritability of body measurements in a rural Indian population. Ann Hum Biol 8: 333–339
Solomon PJ, Thompson EA 1983 The inheritance of height in a Finnish population. Ann Hum Biol 10: 247–256
Tilsala R, Antero RL 1971 Some parent-child correlations for height, weight and skeletal age up to 10 years. Acta Paediatr Scand Suppl 220: 42–48
Gerylovova A, Bouchalova M 1974 The relationship between children's and parents' height in the age range of 0 to 6 years. Ann Hum Biol 1: 223–232
Malina R, Mueller WH, Holman JD 1976 Parent-child correlation and heritability of stature in Philadelphia black and white children 6 to 12 years of age. Hum Biol 48: 475–486
Russell M. 1976 Parent-child and sibling-sibling correlationsheight and weight in a rural Guatemalan population of preschool children. Hum Biol 48: 501–515
Ranke MB, Lindberg A 1996 Growth hormone treatment of short children born small for gestational age or with Silver-Russell syndrome: results from KIGS (Kabi International Growth Study), including the first report on final height. Acta Padiatr Suppl 417: 18–26
Kristrom B, Karlberg J, Albertsson-Wikland K Swedish Paediatric Study Group for GH treatment 1995 Prediction of the growth response of short prepubertal children treated with growth hormone. Acta Padiatr 84: 51–57
Ranke MB, Guilbaud O, Lindberg A, Cole T, International Board of the Kabi Pharmacia International Growth Study 1993 Prediction of the growth response in children with various growth disorders treated with growth hormone: analyses of data from the Kabi Pharmacia International Growth Study. Acta Padiatr Suppl 391: 82–88
Albanese A, Stanhope R 1995 Predictive factors in the determination of final height in boys with constitutional delay of growth and puberty. J Pediatr 126: 545–550
Crowne EC, Shalet SM, Wallace HB, Eminson DM, Price DA 1990 Final height in boys with untreated constitutional delay in growth and puberty. Arch Dis Child 65: 1109–1112
Tanner JM, Goldstein H, Whitehouse RH 1970 Standards for children's height at ages 2:9 years allowing for height of parents. Arch Dis Child 45: 755–762
Karlberg J, Lawrence C, Albertsson-Wikland K 1994 Prediction of final height in short, normal and tall children. Acta Padiatr Suppl 406: 3–9
Karlberg J, Albertsson-Wikland K 1995 Growth in full-term small-for-gestational-age infants: from birth to final height. Pediatr Res 38: 733–739
Falkner F, Tanner JM 1978 Human Growth: Principles and Prenatal Growth. Cassell Ltd, London, 299–305.
Gardner JM, Altman GD 1989 Statistics with Confidence. BMJ, London, 37–39.
Burdick RK, Graybill FA 1992 Confidence Intervals on the Variance Components. Marcel Dekker, New York, 25–26.
Pearson ES, Hartley HO 1958 Biometrika Tables for Statisticians. University Press, Cambridge, UK, 183–184.
SAS Institute Inc 1996 SAS series. Version 6.10, 18-274. SAS Institute Inc, Cary, NC
Karlberg P, Taranger J, Engstrom I, Karlberg J, Landstrom T, Lichtenstein H, Lindstrom B, Svennberg-Redegren I 1976 Physical growth from birth to 16 y and longitudinal outcome of the study during the same age period. Acta Paediatr Scand Suppl 258: 7–76
Karlberg J 1989 A biological-oriented mathematical model (ICP) for human growth. Acta Padiatr Scand Suppl 350: 70–94
Tanner JM, Whitehouse RH, Marshall WA, Carter BS 1975 Prediction of adult height from height, bone age, and occurrence of menarche, at 4 to 16 with allowance for midparent height. Arch Dis Child 50: 14–26
Tanner JM, Landt KW, Cameron N, Carter BS, Patel J 1983 Prediction of adult height from height and bone age in childhood. Arch Dis Child 58: 767–776
Roche AF, Wainer H, Thissen D 1975 The RWT method for the prediction of adult stature. Pediatrics 56: 1026–1033
Author information
Authors and Affiliations
Additional information
Supported by The Faculty of Medicine, The University of Hong Kong, Hong Kong, SAR, Swedish Medical Research Council (7905), and Pharmacia Upjohn Inc., Stockholm, Sweden.
Rights and permissions
About this article
Cite this article
Luo, Z., Albertsson-Wikland, K. & Karlberg, J. Target Height as Predicted by Parental Heights in a Population-Based Study. Pediatr Res 44, 563–571 (1998). https://doi.org/10.1203/00006450-199810000-00016
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199810000-00016
This article is cited by
-
Evidence of correlations between human partners based on systematic reviews and meta-analyses of 22 traits and UK Biobank analysis of 133 traits
Nature Human Behaviour (2023)
-
Associations between meeting the Canadian 24-hour movement guidelines and physical, cognitive, social-emotional, and overall development in early childhood
Journal of Activity, Sedentary and Sleep Behaviors (2022)
-
Longitudinal associations between body composition and regional fat distribution and later attained height at school entry among preschool children predisposed to overweight
European Journal of Clinical Nutrition (2020)
-
Maternal pre-pregnancy body mass index, smoking in pregnancy, and alcohol intake in pregnancy in relation to pubertal timing in the children
BMC Pediatrics (2019)
-
Seasonal variations in vitamin D in relation to growth in short prepubertal children before and during first year growth hormone treatment
Journal of Endocrinological Investigation (2015)
