
Abstract
Background/Objectives
Obesity is associated with a lower mortality risk among patients with heart failure (HF). Whether this obesity paradox applies to all-cause hospitalizations is unknown. We aimed to investigate the association between body mass index (BMI) and 30-day all-cause readmissions following HF hospitalization.
Subjects/Methods
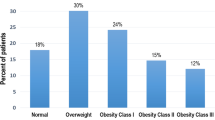
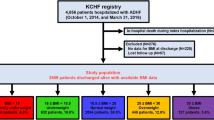
We retrospectively evaluated 2252 HF hospital admissions of Centers of Medicare Services beneficiaries from an academic medical center. We classified obesity using established BMI categories. All 30-day postdischarge readmission to all hospitals and mortality events were documented. We evaluated 30-day postdischarge unplanned, all-cause readmission and death in the total cohort, propensity-matched cohort, and by ejection fraction (EF).
Results
An Overweight-Obese BMI (BMI ≥ 25 kg/m2) was paradoxically associated with a lower mortality rate than a Normal BMI (18.5–24.9 kg/m2) (5.0% vs 8.5%, p = 0.0018). In contrast, an Overweight-Obese BMI was associated with a 29% (95% CI: 1.03–1.63) increased relative risk of all-cause readmission compared with a Normal BMI (23.2% vs 18.9%, p = 0.0288), which was consistent across obesity severity subgroups. Among 966 matched admissions, an Overweight-Obese BMI retained higher readmission risk compared with a Normal BMI (25.1% vs 17.2%, p = 0.003). After matching, readmissions remained higher for Overweight-Obese vs Normal BMI in admissions with reduced EF (25.7% vs 17.8%, p = 0.032) and preserved EF (23.0% vs 15.0%, p = 0.048). No difference in the percentage of readmissions for HF (40%) or noncardiovascular causes (45%) existed between Overweight-Obese and Normal BMI groups.
Conclusions
Despite a lower mortality risk, increased BMI is associated with increased all-cause hospital readmission rates in an elderly HF population which persists after propensity matching.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others
References
Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2014;384:766–81.
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics-2015 update: a report from the American Heart Association. Circulation. 2015;131:e29–e322.
Nagarajan V, Kohan L, Holland E, Keeley EC, Mazimba S. Obesity paradox in heart failure: a heavy matter. ESC Heart Fail. 2016;3:227–34.
Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR, Woo MA, Tillisch JH. The relationship between obesity and mortality in patients with heart failure. J Am Coll Cardiol. 2001;38:789–95.
Fonarow GC, Srikanthan P, Costanzo MR, Cintron GB, Lopatin M, Committee ASA, et al. An obesity paradox in acute heart failure: analysis of body mass index and inhospital mortality for 108,927 patients in the acute decompensated heart failure national registry. Am Heart J. 2007;153:74–81.
Padwal R, McAlister FA, McMurray JJ, Cowie MR, Rich M, Pocock S, et al. The obesity paradox in heart failure patients with preserved versus reduced ejection fraction: a meta-analysis of individual patient data. Int J Obes (Lond). 2014;38:1110–4.
Tsujimoto T, Kajio H. Abdominal obesity is associated with an increased risk of all-cause mortality in patients with HFpEF. J Am Coll Cardiol. 2017;70:2739–49.
Zamora E, Lupon J, Enjuanes C, Pascual-Figal D, de Antonio M, Domingo M, et al. No benefit from the obesity paradox for diabetic patients with heart failure. Eur J Heart Fail. 2016;18:851–8.
Vest AR, Wu Y, Hachamovitch R, Young JB, Cho L. The heart failure overweight/obesity survival paradox: the missing sex link. JACC Heart Fail. 2015;3:917–26.
Piepoli MF, Corra U, Veglia F, Bonomi A, Salvioni E, Cattadori G, et al. Exercise tolerance can explain the obesity paradox in patients with systolic heart failure: data from the MECKI score research group. Eur J Heart Fail. 2016;18:545–53.
Zafrir B, Salman N, Crespo-Leiro MG, Anker SD, Coats AJ, Ferrari R, et al. Body surface area as a prognostic marker in chronic heart failure patients: results from the heart failure registry of the heart failure association of the european society of cardiology. Eur J Heart Fail. 2016;18:859–68.
Sharma A, Lavie CJ, Borer JS, Vallakati A, Goel S, Lopez-Jimenez F, et al. Meta-analysis of the relation of body mass index to all-cause and cardiovascular mortality and hospitalization in patients with chronic heart failure. Am J Cardiol. 2015;115:1428–34.
Schafer MH, Ferraro KF. Long-term obesity and avoidable hospitalization among younger, middle-aged, and older adults. Arch Intern Med. 2007;167:2220–5.
Finkelstein EA, Trogdon JG, Cohen JW, Dietz W. Annual medical spending attributable to obesity: payer-and service-specific estimates. Health Aff (Millwood). 2009;28:w822–31.
Dharmarajan K, Hsieh AF, Lin Z, Bueno H, Ross JS, Horwitz LI, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309:355–63.
Nutrition physical activity and obesity data trends and maps. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC), National Center for Chronic Disease Prevention and Health Promotion, Division of Nutrition, Physical Activity and Obesity, Atlanta, GA. 2015. http://www.cdc.gov/nccdphp/DNPAO/index.html. Accessed Dec 2016.
Yale New Haven Health Services Corporation/Center for Outcomes Research & Evaluation prepared for the Centers for Medicare & Medicaid Services. 2016. Condition-specific measures updates and specifications report hospital-level 30-day risk-standardized readmission measures. Heart failure version 9.0. March 2016. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/Measure-Methodology.html. Accessed 30 June 2016.
Pi-Sunyer FX, Becker DM, Bouchard C, Carleton RA, Colditz GA. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report. National Institutes of Health: National Heart, Lung, and Blood Institute. 1998; No. 98-4083:1–262. https://www.nhlbi.nih.gov/files/docs/guidelines/ob_gdlns.pdf. Accessed Jan 2018.
World Health Organtization global database on body mass index: the international classification of adult underweight, overweight and obesity according to BMI. 2017. http://apps.who.int/bmi/index.jsp?introPage=intro_3.html. Accessed Jan 2018.
Shah R, Gayat E, Januzzi JL Jr., Sato N, Cohen-Solal A, diSomma S, et al. Body mass index and mortality in acutely decompensated heart failure across the world: a global obesity paradox. J Am Coll Cardiol. 2014;63:778–85.
Centers for Medicare and Medicaid Services Hierarchical Condition Category Risk Adjustment Model V22. https://www.cms.gov/medicare/health-plans/medicareadvtgspecratestats/risk-adjustors.html. Accessed Mar 2019.
Tsimploulis A, Lam PH, Arundel C, Singh SN, Morgan CJ, Faselis C, et al. Systolic blood pressure and outcomes in patients with heart failure with preserved ejection fraction. JAMA Cardiol. 2018;3:288–97.
Cox ZL, Lai P, Lewis CM, Lindenfeld J, Collins SP, Lenihan DJ. Customizing national models for a medical center's population to rapidly identify patients at high risk of 30-day all-cause hospital readmission following a heart failure hospitalization. Heart Lung. 2018;47:290–6.
SAS Institute INC. Performing a 1:N case-control match on propensity score. SAS Institute INC. https://support.sas.com/resources/papers/proceedings/proceedings/sugi29/165-29.pdf. Accessed April 2019.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46:399–424.
Austin PC. Primer on statistical interpretation or methods report card on propensity-score matching in the cardiology literature from 2004 to 2006: a systematic review. Circ Cardiovasc Qual Outcomes. 2008;1:62–7.
Joshy G, Korda RJ, Attia J, Liu B, Bauman AE, Banks E. Body mass index and incident hospitalisation for cardiovascular disease in 158 546 participants from the 45 and Up Study. Int J Obes (Lond). 2014;38:848–56.
Bello NA, Claggett B, Desai AS, McMurray JJ, Granger CB, Yusuf S, et al. Influence of previous heart failure hospitalization on cardiovascular events in patients with reduced and preserved ejection fraction. Circ Heart Fail. 2014;7:590–5.
Solomon SD, Dobson J, Pocock S, Skali H, McMurray JJ, Granger CB, et al. Influence of nonfatal hospitalization for heart failure on subsequent mortality in patients with chronic heart failure. Circulation. 2007;116:1482–7.
Carson PE, Anand IS, Win S, Rector T, Haass M, Lopez-Sendon J, et al. The hospitalization burden and post-hospitalization mortality risk in heart failure with preserved ejection fraction: results from the I-PRESERVE trial (Irbesartan in heart failure and preserved ejection fraction). JACC Heart Fail. 2015;3:429–41.
Lala A, McNulty SE, Mentz RJ, Dunlay SM, Vader JM, AbouEzzeddine OF, et al. Relief and recurrence of congestion during and after hospitalization for acute heart failure: insights from diuretic optimization strategy evaluation in acute decompensated heart failure (DOSE-AHF) and cardiorenal rescue study in acute decompensated heart failure (CARESS-HF). Circ Heart Fail. 2015;8:741–8.
Powell-Wiley TM, Ngwa J, Kebede S, Lu D, Schulte PJ, Bhatt DL, et al. Impact of body mass index on heart failure by race/ethnicity from the get with the guidelines-heart failure (GWTG-HF) registry. JACC Heart Fail. 2018;6:233–42.
Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B, et al. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. 2014;370:1383–92.
Redfield MM, Chen HH, Borlaug BA, Semigran MJ, Lee KL, Lewis G, et al. Effect of phosphodiesterase-5 inhibition on exercise capacity and clinical status in heart failure with preserved ejection fraction: a randomized clinical trial. JAMA. 2013;309:1268–77.
Haass M, Kitzman DW, Anand IS, Miller A, Zile MR, Massie BM, et al. Body mass index and adverse cardiovascular outcomes in heart failure patients with preserved ejection fraction: results from the Irbesartan in heart failure with preserved ejection fraction (I-PRESERVE) trial. Circ Heart Fail. 2011;4:324–31.
Paulus WJ, Tschope C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013;62:263–71.
Obokata M, Reddy YNV, Pislaru SV, Melenovsky V, Borlaug BA. Evidence supporting the existence of a distinct obese phenotype of heart failure with preserved ejection fraction. Circulation. 2017;136:6–19.
Shah SJ, Katz DH, Selvaraj S, Burke MA, Yancy CW, Gheorghiade M, et al. Phenomapping for novel classification of heart failure with preserved ejection fraction. Circulation. 2015;131:269–79.
Rossi AP, Bianchi L, Volpato S, Bandinelli S, Guralnik J, Zamboni M, et al. Dynapenic abdominal obesity as a predictor of worsening disability, hospitalization, and mortality in older adults: results from the InCHIANTI study. J Gerontol A Biol Sci Med Sci. 2017;72:1098–104.
Zhang X, Zhang W, Wang C, Tao W, Dou Q, Yang Y. Sarcopenia as a predictor of hospitalization among older people: a systematic review and meta-analysis. BMC Geriatr. 2018;18:188.
Streng KW, Voors AA, Hillege HL, Anker SD, Cleland JG, Dickstein K, et al. Waist-to-hip ratio and mortality in heart failure. Eur J Heart Fail. 2018;20:1269–77.
Clark AL, Fonarow GC, Horwich TB. Waist circumference, body mass index, and survival in systolic heart failure: the obesity paradox revisited. J Card Fail. 2011;17:374–80.
Fulster S, Tacke M, Sandek A, Ebner N, Tschope C, Doehner W, et al. Muscle wasting in patients with chronic heart failure: results from the studies investigating co-morbidities aggravating heart failure (SICA-HF). Eur Heart J. 2013;34:512–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Cox, Z.L., Lai, P., Lewis, C.M. et al. Body mass index and all-cause readmissions following acute heart failure hospitalization. Int J Obes 44, 1227–1235 (2020). https://doi.org/10.1038/s41366-019-0518-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-019-0518-6
This article is cited by
-
The Association Between Obesity and Key Health or Psychosocial Outcomes Among Autistic Adults: A Systematic Review
Journal of Autism and Developmental Disorders (2022)
