
Abstract
Introduction
The purpose of this study was to examine the relationships between screening questions for secondhand smoke (SHS) exposure and biomarker results using hair nicotine levels. Our ultimate goal was to develop sensitive and valid screening tools in pediatric clinical settings for SHS exposure.
Methods
Investigators developed a core set of questions regarding exposure. Data from two separate ongoing studies of well children and those with bronchopulmonary dysplasia (BPD) were used to assess the concordance between responses and hair nicotine levels. Sensitivity, a positive predictive value, and accuracy were examined.
Results
There was no single question with similar sensitivity in both populations. The question with the highest positive predictive value (90.8% well-cohort and 84.6% BPD cohort) for both the groups was whether the child had been exposed to in-home smoking in the last 7 days. The question with the highest accuracy for both groups was the number of smokers at home (0 vs ≥ 1), with an accuracy of 72.4% for well children and 79.0% for the BPD cohort.
Conclusions
There was a wide variability in the performance of specific questions. These data demonstrate that a “one-size-fits-all” approach to screening for secondhand tobacco smoke exposure may not be appropriate for all pediatric populations.
Similar content being viewed by others

Introduction
Secondhand smoke (SHS) exposure during childhood is linked to multiple health issues, including increased prevalence and severity of asthma, bronchiolitis, and influenza, increased rates of otitis media, and sudden infant death syndrome 1–7. Smoke exposure may be assessed using biomarkers, environmental measures, and survey measures. Survey measures of smoke exposure have been used for field and epidemiologic research, to assess smoking bans, and in clinical settings [8, 9]. Pediatric health care providers need simple ways to screen for SHS exposure in children, both as a risk stratification measure and to identify caregivers who smoke. Screening is important to promote smoking cessation and exposure reduction, such as having smoke-free homes and cars.
However, the research on the concordance of parental report and a biological marker of exposure has been mixed, with more agreement between these in a non-clinical setting. Hair nicotine has been used to assess for home exposure to tobacco smoke in young children [10, 11] with a significant dose–response relationship between hair nicotine level and the presence and number of parental smokers. Among elderly non-smoking adults, hair nicotine level has been used to successfully validate a brief survey scale to assess tobacco exposure in the primary care setting [12].
Using the epidemiological survey question of “any reported smokers in the home,” NHANES III data showed a sensitivity of 0.65 and a specificity of 0.92 in detecting a serum cotinine of 0.2 ng/mL or greater [13]. In the same study, Spearman correlations between cotinine levels and the number of smokers in the home and the number of cigarettes consumed were significant at 0.67 and 0.68, respectively [13].
However, studies performed in clinical settings have shown weaker relationships between survey responses and biomarkers, particularly in the setting of a child with a chronic respiratory condition such as asthma or bronchopulmonary dysplasia [14]. Howrylak et al. [15] found that in a cohort of asthmatic children, biomarkers (serum and salivary cotinine) were related to the increased risk of readmission for asthma, but a caregiver report of any tobacco exposure was not. Among children whose caregivers reported no tobacco exposure, 39% had detectable serum cotinine, and almost 70% had detectable saliva cotinine. Similar findings among asthmatic children were found by other investigators [16].
Additionally, survey measures may not elicit responses detecting low levels of exposure. Research has shown that very low levels of smoke exposure, which may be missed by standard screening questions and are lower than standard cut points accepted as SHS exposure based on NHANES data [13], are associated with eurocognitive deficits [17]. Low levels of exposure have also been associated with decreased serum antioxidant levels [18], and with increased risk of asthma exacerbations [15]. Children with low levels of exposure may be exposed by a parent who smokes only outside. Also, biomarkers can capture “third-hand” smoke exposure which is the nicotine residue left on surfaces (such as a caregiver’s clothes), which is then ingested, dermally absorbed, and/or inhaled by young children [19]. Matt et al. [20] found that infants whose mother smoked only outside had significantly elevated urine cotinine levels.
The purpose of this study was to examine the relationships between screening questions for SHS and biomarker results using hair nicotine in two different populations of children. Our ultimate goal was to develop sensitive and valid screening tools in pediatric clinical settings for SHS exposure.
Methods
Survey questions
At the start of the process, a search was conducted of tobacco-related literature, as well as national surveys, to develop an exhaustive list of questions about smoking behaviors, SHS exposure, knowledge and attitudes about tobacco smoking, and demographics. Each team member also shared their local survey tools. These questions were mapped by a topic area, and through an iterative process, questions were kept as core, optional, or deleted. Questions were prioritized by (1) previous validation, (2) current use by large national datasets such as NHANES, (3) current use in the Social Climate Survey of Tobacco Control [21], and (4) previously used in published tobacco research [22,23,24,25,26,27,28]. The list of core and optional questions, with references, can be at viewed at https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/Richmond-Center/Pages/Measurement-Core.aspx by clicking the “SHS exposure and use” tab. Data from two separate ongoing studies that examine the relationship between SHS and disease were used to assess the concordance between the responses to these questions and biological measures. Investigators from the two studies selected items from the core and optional questions when creating their survey tools.
Nationwide Children’s Hospital (the well-child group)
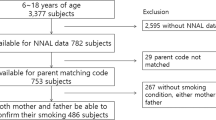
Healthy children (n = 148) aged 2–5 years were recruited by convenience sampling at one of Nationwide Children’s Hospital’s (NCH, Columbus, Ohio) Pediatric Primary Care Centers, and by e-mail recruiting throughout the NCH community. Inclusion criteria were children of ages 2–5, with any level of reported smoke exposure or no reported smoke exposure, and an English-speaking parent. Exclusion criteria were the use of daily medication, including inhaled steroids, recent (within 1 week) antihistamine or decongestant use, and congenital heart disease. All children were evaluated at the Clinical Studies Center at NCH (outside of the primary care visit), a few weeks after recruitment. This study was approved by the Nationwide Children’s Hospital IRB (Protocol # IRB11-00437). Of 250 eligible patients approached, 149 were studied, with adequate hair samples obtained on 148 patients.
Johns Hopkins University Hospital (BPD group)
One-hundred-and-forty-three preterm children aged 0.12–9.47 years were recruited from the Johns Hopkins Bronchopulmonary Dysplasia (BPD) Clinic between January 2012 and January 2014. Patients were referred to the clinic by area neonatal intensive care units or pediatricians by having the diagnosis of BPD. Of 227 eligible patients approached, 151 consented for the collection of hair samples. The final study population included 143 subjects from whom hair samples and questionnaires were able to be successfully collected during a clinic visit. The Johns Hopkins Institutional Review Board approved the study (Protocol #: NA_051884).
Biological testing
At both sites, approximately 20–40 shafts of hair, 2–3 cm in length were cut at the root at the occipital area. Hairs were stored and later sent for assays at Johns Hopkins School of Public Health. Hair was analyzed as previously described by Kim et al. 29. Briefly, between 10 and 30 mg of each hair sample (depending on availability of hair) was washed using 3 mL of dichloromethane and sonicated (Model 250HT, Aquasonic, Hayward, CA, USA) for 30 min before nicotine extraction and analysis [29]. This process removed any nicotine adherent to the surface of the hair, limiting the measurement of nicotine to that accumulated by inhalation, ingestion, and dermal absorption, and subsequent incorporation into the growing hair. Nicotine was extracted from the hair samples using an isotope dilution method with diethyl ether and an internal standard (nicotine-d3, Supelco, St. Louis, MO, USA) as previously described by Kim et al. [29]. Hair nicotine analysis was performed using gas chromatography/mass spectrometry (GC-17/MS-QP5000, Shimadzu, Canby, OR, USA) in selected ion monitoring (SIM) and splitless modes. For quality control, approximately 10% of the hair samples were subjected to duplicate analyses. The limit of detection (LOD) was 0.41 ng/mg for a 30-mg hair sample. Hair nicotine was run in several batches; this represents the highest LOD for all batches.
Statistical methods
To calculate the geometric mean for each question response for each dataset, below the limit of detection (LOD) values were imputed using Bayesian techniques with JAGS/R software. A log-normal distribution was assumed, with imputed values restricted to the left tail of the distribution, ranging from 0 to the batch LOD. Models to impute the data were fit using a GIBBS sample. Ten Markov chains were run until convergence, and an iteration near the end of each chain was outputted as an imputed dataset. The ten imputed datasets were then analyzed using simple linear regression, and the results were combined to determine the overall geometric mean. Hair nicotine levels were dichotomized as exposed or unexposed, using the maximum batch LOD across the two sites of 0.41 ng/mL as a cutoff, to evaluate question performance at each of the sites.
Descriptive statistics were used to describe the different patient populations at each site. Sensitivity, positive predictive value, and accuracy were examined for each question. Sensitivity was the proportion of those exposed (hair nicotine values above 0.41 ng/mg) that were correctly identified by the question as having been exposed to SHS. A positive predictive value (PPV) was the proportion of positive responses to the question of those that were truly exposed. Accuracy or the correct classification rate was the proportion of subjects correctly classified as exposed or unexposed to SHS.
Results
A demographic description of the two groups can be found in Table 1. The two groups differed in several respects. The mean age for children in the BPD group was younger than the well-child group (1.19 years compared to 3.21 years). There were more multiracial and Hispanic/Latino children in the well-child group compared to the BPD group, but approximately the same proportion of African-American children. The children in the well-child group were insured by Medicaid in 86% of cases compared to 63% of the BPD group. Maternal educational attainment was lower in the well-child group, with 30% having less than a high school education compared with 8% in the BPD group.
The well-child group was highly exposed to tobacco smoke with 98 (66%) of children living with or cared for by a smoker (Table 2). The overall geometric mean of hair nicotine for this group was 1.72 ng/mg (CI 1.28 and 2.31). Sixty children (41%) lived with one smoker, 18% with two smokers, and 9% with more than two smokers. Exposure was most common in the home (59%), relatives’ homes (45%), and cars (30%). In contrast, the reported SHS exposure was less common among the BPD population, with 31 (22%) of children living with or cared for by a smoker. The overall geometric mean of hair nicotine for the BPD group was 0.07 ng/mg (CI 0.04 and 0.13). Thirteen children (9%) lived with one smoker, 8% with two smokers, and 4% with more than two smokers. Exposure was most common in the home (9%), outdoor public places (8%), and relatives’ homes (5%). The well-child group had higher hair nicotine than the BPD group for almost all questions regarding exposure.
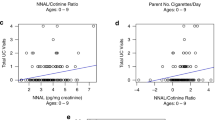
Question 3 of Table 2 (How many people living in this child’s home smoke cigarettes, cigars, cigarillo, and pipes?) differentiated the most exposed from those less exposed in both the well-child and BPD groups sequentially by the number of smokers in the home, with the geometric mean of hair nicotine increasing from 0 to 4 or more smokers. However, question 5 (Table 2) (How often does anyone smoke inside your home?) did not capture exposure as well.
We also examined how smoking is handled in the car, and whether smoking takes place in the home, outside the home, or both (Table 2). Fifty nine (40%) of well-child participants responded that no one is allowed to smoke in the car, whereas 136 (95%) of BPD participants had this rule. Similarly, 49 (67%) of well-child participants stated that they smoked both indoors and outdoors compared to only three (10%) of BPD participants. Three caregivers of subjects (well-child) endorsed smoking inside only, 49 both inside and outside, and 21 outside only, with the geometric mean hair nicotine levels of the children at 11.3 ng/mg, 4.70 ng/mg, and 1.75 ng/mg. In the BPD group, no one endorsed smoking inside only, three endorsed both inside and outside, and 28 endorsed outside only, with the geometric mean hair nicotine levels of 0.13 ng/mg and 1.19 ng/mg, respectively (Table 2).
In Table 3, we present sensitivity, a positive predictive value, and the correct classification rate (accuracy) for the questions found in Table 2. There was no single question with similar sensitivity in both populations. For example, question 3, with the highest sensitivity (75.7%) for the well-child group: (How many people living in the home smoke cigarettes…?) had 51% sensitivity in the BPD group. In contrast, the positive predictive values for questions 1–4 were at least 83% and are similar between groups. The question with the highest PPV (90.8% well-child, 84.6% BPD) for both the groups was Question 2––whether the child had been exposed to in-home smoking versus elsewhere in the last 7 days. The question with the highest PPV (98.1%) overall was regarding smoking rules location (question 7) only for the well-child group. However, this question did not perform as well in the BPD group (66.7%). Regarding accuracy, approximately 25% of the well-child group and 20% of the BPD group were not correctly classified by the best question for each group. The question with the highest accuracy for both groups was #3 (How many people living in this child’s home smoke cigarettes, cigars, cigarillo, and pipes?) with an accuracy of 72.4% for the well-child group and 79.0% for the BPD group. No combination of questions performed better than did the individual screening questions.
Discussion
Secondhand tobacco smoke is a significant health hazard for infants and children, both healthy individuals and those with chronic respiratory disease. This study attempted to assess the sensitivity and validity of screening questions using two different pediatric populations. The strengths of this study include a common core of questions with an identical biomarker assessment at the same laboratory. Overall, questions that asked who smoked tended to have a higher sensitivity and a predictive value than questions asked about where smoking occurred or how it was handled in certain locations. Nevertheless, there was a variation in the performance of specific questions. The limitations of the study include a low prevalence of smoke exposure in the BPD group, the choice of hair nicotine as a “gold standard” and limited generalizability with a largely minority population, and a high prevalence of public insurance.
The reasons for the gaps between parental report of children’s smoke exposure and biomarkers are complex and may include poor recall of exposure, the lack of parental awareness of potential sources of the exposure if a parent does not smoke, social desirability of reporting no smoke exposure, and the context of where the questions were asked. Children may be exposed to tobacco smoke drifting in from a neighboring apartment [18], but parents may not consider that to be “exposure.” Likewise, if children are exposed on the streets, or at a friend or relative’s house, parents may not think to report this exposure, contributing to the underestimation.
Social desirability bias may be different depending on the population of children studied. The well-child population consisted of healthy children without an underlying illness, compared to the BPD population which represented a younger and sicker population. A bias to report no exposure for the child may lead to more false-negative reporting and hence lower sensitivity of the screening questions in the BPD group compared to the well-child group. Parents of healthy children may feel free to discuss their smoking as their children are not sick, but parents of hospitalized or chronically ill children may underreport SHS exposure. Additionally, the setting where the questions were asked may influence the performance of the questions. The questionnaires were administered in a research setting for the well-child population, whereas they were administered in a clinical setting for the BPD population. As mentioned previously, studies performed in clinical settings have shown weaker relationships between survey responses and biomarkers [14, 15].
The prevalence of smoke exposure within each group as measured by hair nicotine impacts the PPV of the screening question. Hair nicotine levels overall in the well-child group were much higher than in the BPD group, and therefore, the PPV of each screening question was lower for the BPD group.
As mentioned above, the low prevalence of nicotine exposure in the BPD group is a limitation of this study. For this group, over half the values (52%) were less than the LOD per batch. There were four-batch LODs for the BPD group: 0.029 ng/mg, 0.043 ng/mg, 0.046 ng/mg, and 0.36 ng/mg. With more than half of the values below their corresponding batch LOD, it is reasonable to have a geometric mean lower than the maximum batch LOD across both sites (0.41 ng/mg).
We selected hair nicotine as the “gold standard” for smoke exposure because it was easy to collect, store, and transport compared to other biomarkers such as urine and serum cotinine. While hair nicotine has been validated as a biomarker for smoke exposure in children [8], it measures months of exposure and is not sensitive to daily variability in exposure [8]. It is unknown if it reflects other sources of nicotine exposure such as an electronic nicotine delivery device vapor.
Overall, these data demonstrate that a “one-size-fits-all” approach to screening for SHS exposure may not be ideal for all pediatric populations. Although questions that ask who smokes may perform better, questionnaires may need to be different for clinical versus research settings. Also, biological markers may be critical in settings where the social desirability of nonexposure is the greatest, including inpatient assessment of patients with a severe disease or those from vulnerable populations (cystic fibrosis and BPD). Given the difficulty of obtaining biomarker assessment clinically, future efforts should focus on advocating for hospital and university laboratories to conduct high-quality, rapid testing for nicotine or its metabolite, cotinine.
Implications
The performance of screening questions for secondhand smoke exposure in children depends on the pediatric population being assessed. Biological measures of smoke exposure may be necessary for high-risk populations as there may be no single question or a set of questions to identify exposed children accurately.
References
Stapleton M, Howard-Thompson A, George C, Hoover RM, Self TH. Smoking and asthma. J Am Board Fam Med. 2011;24:313–22.
Eisner M, Klein J, Hammond S, Koren G, Lactao G, Iribarren C. Directly measured second hand smoke exposure and asthma health outcomes. Thorax. 2005;60:814–21.
Jones LL, Hassanien A, Cook DG, Britton J, Leonardi-Bee J. Parental smoking and the risk of middle ear disease in children: a systematic review and meta-analysis. Arch Pediatr Adolesc Med. 2012;166:18–27.
Ahn A, Edwards KM, Grijalva CG, et al. Secondhand smoke exposure and illness severity among children hospitalized with pneumonia. J Pediatr. 2015;167:869–74.
Wilson KM, Pier JC, Wesgate SC, Cohen JM, Blumkin AK. Secondhand tobacco smoke exposure and severity of influenza in hospitalized children. J Pediatr. 2013;162:16–21.
Treyster Z, Gitterman B. Second hand smoke exposure in children: environmental factors, physiological effects, and interventions within pediatrics. Rev Environ Health. 2011;26:187–95.
Jones LL, Hashim A, McKeever T, Cook DG, Britton J, Leonardi-Bee J. Parental and household smoking and the increased risk of bronchitis, bronchiolitis and other lower respiratory infections in infancy: systematic review and meta-analysis. Respir Res. 2011;12:1465–9921.
Avila-Tang E, Al-Delaimy WK, Ashley DL, et al. Assessing secondhand smoke using biological markers. Tob Control. 2013;22:164–71.
Avila-Tang E, Elf JL, Cummings KM, et al. Assessing secondhand smoke exposure with reported measures. Tob Control. 2013;22:156–63.
Vardavas CI, Tzatzarakis MN, Tsatsakis AM, et al. Biomarkers of passive smoking among Greek preschool children. Eur J Pediatr. 2006;165:891–6.
Tzatzarakis MN, Vardavas CI, Terzi I, et al. Hair nicotine/cotinine concentrations as a method of monitoring exposure to tobacco smoke among infants and adults. Hum Exp Toxicol. 2012;31:258–65.
Vardavas CI, Agaku I, Filippidis F, et al. The Secondhand Smoke Exposure Scale (SHSES): a hair nicotine validated tool for assessing exposure to secondhand smoke among elderly adults in primary care. Tob. Prev. Cessation. 2017;3:9.
Wilkinson JD, Arheart KL, Lee DJ. Accuracy of parental reporting of secondhand smoke exposure: The National Health and Nutrition Examination Survey III. Nicotine Tob Res. 2006;8:591–7.
Collaco JM, Aherrera AD, Breysse PN, Winickoff JP, Klein JD, McGrath-Morrow SA. Hair nicotine levels in children with bronchopulmonary dysplasia. Pediatrics. 2015;135:2014–501.
Howrylak JA, Spanier AJ, Huang B, et al. Cotinine in children admitted for asthma and readmission. Pediatrics. 2014;133:2013–422.
McCarville M, Sohn MW, Oh E, Weiss K, Gupta R. Environmental tobacco smoke and asthma exacerbations and severity: the difference between measured and reported exposure. Arch Dis Child. 2013;98:510–4.
Yolton K, Dietrich K, Auinger P, Lanphear BP, Hornung R. Exposure to environmental tobacco smoke and cognitive abilities among U.S. children and adolescents. Environ Health Perspect. 2005;113:98–103.
Wilson KM, Finkelstein JN, Blumkin AK, Best D, Klein JD. Micronutrient levels in children exposed to secondhand tobacco smoke. Nicotine Tob Res. 2011;13:800–8.
Mahabee-Gittens EM, Merianos AL, Matt GE. Preliminary evidence that high levels of nicotine on children’s hands may contribute to overall tobacco smoke exposure. Tob Control. 2017;30:2016–053602.
Matt GE, Quintana PJ, Hovell MF, et al. Households contaminated by environmental tobacco smoke: sources of infant exposures. Tob Control. 2004;13:29–37.
Winickoff JP, McMillen RC, Carroll BC, et al. Addressing parental smoking in pediatrics and family practice: a national survey of parents. Pediatrics. 2003;112:1146–51.
U.S. Department of Health and Human Services. National Health and Nutrition Examination Survey, 2005–2006. Centers for Disease Control. https://wwwn.cdc.gov/nchs/nhanes/Search/DataPage.aspx?Component=Questionnaire&CycleBeginYear=2005
2010 National Health Interview Survey. Centers for Disease Control and Prevention Web site http://www.cdc.gov/nchs/nhis/quest_data_related_1997_forward.htm.
Groner JA, Huang H, Nicholson L, Kuck J, Boettner B, Bauer JA. Secondhand smoke exposure and hair nicotine in children: age-dependent differences. Nicotine Tob Res. 2012;14:1105–9.
Halterman JS, Borrelli B, Tremblay P, et al. Screening for environmental tobacco smoke exposure among inner-city children with asthma. Pediatrics. 2008;122:1277–83.
National Social Climate Survey of Tobacco Control. The Social Climate of Tobacco Control Web site http://www.socialclimate.org/. Accessed June 2013.
Centers for Disease Control and Prevention, World Health Organization. Tobacco Questions for Surveys: a subset of key questions from the Global Adult Tobacco Survey (GATS). http://www.who.int/tobacco/surveillance/tqs/en/.
Wipfli H, Avila-Tang E, Navas-Acien A, et al. Secondhand smoke exposure among women and children: evidence from 31 countries. Am J Public Health. 2008;98(4):672–9.
Kim SR, Wipfli H, Avila-Tang E, Samet JM, Breysse PN. Method validation for measurement of hair nicotine level in nonsmokers. Biomed Chromatogr. 2009;23:273–9.
Acknowledgements
This work was supported by the American Academy of Pediatrics Julius B. Richmond Center of Excellence through a Center of Excellence grant from the Flight Attendant Medical Research Institute and by grants from the Truth Initiative (formerly American Legacy Foundation). The findings and conclusions are those of the authors and do not necessarily represent the official position of any of these institutions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Groner, J.A., Rule, A.M., McGrath-Morrow, S.A. et al. Assessing pediatric tobacco exposure using parent report: comparison with hair nicotine. J Expo Sci Environ Epidemiol 28, 530–537 (2018). https://doi.org/10.1038/s41370-018-0051-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41370-018-0051-z
Keywords
This article is cited by
-
Association between secondhand marijuana smoke and respiratory infections in children
Pediatric Research (2022)
