
Abstract
Objective
We investigated the effect of a change of altitude of maternal living address on infant birth weight.
Method
Data on infant birth weights of the first and second pregnancies from same women were extracted from all Austrian birth certificates between 1984 and 2016.
Results
A total of 544,624 pair pregnancies were identified and analyzed. We observed a statistically significant interaction (p < .0001) between altitudes of two births and birth weight. Among women having first birth at low altitude (200 m), the estimated second mean birth weight was 3567 g for those remained at low altitudes, and reduced to 3536 g for those ascended (1200 m). In contrast, among women having first births at high altitudes, the estimated birth weight of second birth at high altitude was 3414 g, yet increased to 3499 g compared to those descended to lower altitudes.
Conclusion
We demonstrated a longitudinal negative effect of altitude on birth weight within the same mother from first and second birth. This association is likely to be casual. Relocation of mothers within low-to-medium altitude level may have profound effects on infants’ birth weight.
Similar content being viewed by others

Introduction
Birth weight is a unique maker in health research.1 Low birth weight is an established and powerful predictor for infant mortality and morbidity.2 Beyond infants, the negative impact of low birth weight may persist through adolescence presenting as increased risks of asthma, low intelligence quotient, and mild problem in cognition.3,4,5 More importantly, low birth weight has been recognized as an early life risk factor for a wide range of health outcomes over the life course. In recent years, consistent associations of low birth weight with increased risks of several chronic conditions in adulthood have been documented, including cardiovascular disease, type 2 diabetes, and metabolic syndromes.6,7,8
Factors influencing infants’ birth weight are multifaceted. Epidemiological studies suggested that infant weight differs by fetal gender,9 with boys being heavier than girls at the population level.10 A number of maternal factors have been identified as key determinants of low birth weight including young and advanced maternal age,11,12 social economics status,13 cigarettes smoking,14 primiparity,15 poor maternal nutrition, and low pre-pregnancy weight.16 Another strong determinant of low birth weight is residential altitude. Characterized as an environmental factor, the impact of high altitude has been extensively studied and linked with low birth weight accounting for other fetal and maternal factors in cross-sectional studies.17,18,19,20,21,22,23,24,25,26
At present, mechanisms by which altitude is retarding fetal growth are not completely understood.27 A few biological plausible pathways have been proposed, including maternal oxygen deprivation pathway, which is thought to induce growth-limiting hypobaric hypoxia,28,29,30,31 and a glucose pathway, where the lower arterial glucose concentrations at higher altitude may lower the glucose delivery to and consumption by the fetus.32,33,34 Meanwhile, immigration studies suggested a compensatory genetic or epigenetic process toward high altitude adaption, such that the altitude-associated reduction in birth weight appeared to be greater in shorter staying high-altitude residents compared to those of longest staying.29,31,35,36 Earlier studies suggested that birth weight decrease occur above 2000 m, a threshold for a critical barometric pressure reaching a hypoxic effect.27 In fact, an altitude-associated reduction in birth weight has been consistently reported across low to medium (<2000 m)18,37 to high (2500–4500 m) altitude.21,23,24,28,38 However, prior studies are limited by using cross-sectional designs.
To fill the knowledge gap, we investigate for the first time the longitudinal effect of low-to-medium maternal altitude on infant birth weight using Austria-based birth certificate data. We analyzed maternal altitude and birth weight data of the first and second pregnancies from same women. The approach facilitates adjustments for un-documented maternal factors, providing evidence similarly to a cross-over design study. The range of altitude in our analyses is up to 1600 m and therefore able to exhibit the effect of altitude in countries where the effect was thought to be negligible because of low altitude.
Methods
The Austrian statistical office (Statistics Austria)39 routinely documents national health data across the country. The nature of birth certificate data from Statistics Austria has been detailed previously.18 In brief, data cover all births in Austria and Statistics Austria facilitates linkages of siblings through matching unique mother identifiers. We retrieved maternal- and birth-related data on linked birth sets of siblings and their mothers between 1984 and 2016. We limited our study sample to women with two births only (i.e., two siblings only) to avoid potential confounding from multiple births. All data were retrieved in an anonymous form.
Measurement of birth altitude
Altitude, in meter, was determined by the centroid of the municipality according to mothers’ living addresses. We extracted information on altitude of the first and second births. To enable a prospective investigation on the effect of second birth altitude taking account for the first birth altitude, we derived a ratio metric, which was calculated as a division between the first and second birth altitude. Hence, a value of 1 indicates same altitude for first and second birth, and values >1 indicate increases in altitude from the first to the second birth.
Measurement of birth weight
Birth weight was measured in grams. Birth weight was recorded in intervals of 100, 10, and 1 g between 1984 and 1998, between 1999 and 2010, and 2011 onwards, respectively.
Maternal- and birth-related characteristics
Information on socio-demographic characteristic of mother (i.e., maternal characteristics) including nationality, education, age at second birth, and gender of the first birth, as well as information on the second birth including gender, year of born, time to previous birth, gestational age, and birth length was retrieved.
Inclusion criteria
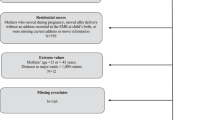
Following information was used to define inclusion criteria: Austrian citizenship of the mother, maternal age 15–45 years, live birth, gestational age 36–44 weeks, birth length 42–60 cm, birth weight >1000 g.18
Statistical analysis
Characteristics of mother and associated two births were described using frequencies for categorical variables (education, sex of two births) and summary statistics for other continuous variables. We examined the prospective association of maternal altitude with birth weight using multivariable regression, modeling the first and second maternal altitudes as a function predicting birth weight of the second born.
The multivariable regression model included a number of adjustments. The effect of a change in altitude may be dependent of the first birth altitude, thus the ratio of altitudes of the two births was included. Additional adjustments included maternal characteristics (age of mother at second birth, education level), characteristics of the first birth (sex, altitude, birth weight), and characteristics of the second birth (year of born, sex, time to previous birth, gestational age, birth length). We further included a squared term for mothers’ age at second birth, time to previous birth, gestational age of the second birth, and second birth length to improve the goodness of fitness of the model. Because of the large number of observations, the significance level was set to p = 0.001. Main effects (altitude) were kept in the model irrespectively of their p values. Sensitivity analyses were carried out by the sex of two births (boy–boy, boy–girl, girl–girl, and girl–boy).
Finally, to visually illustrate the effect of altitude on birth weight of the second born, estimated second birth weight (means and 95% confidence intervals (CIs)) in four scenarios are presented in the figure. We used 200 and 1200 m to indicate low and high altitudes and defined four scenarios as following: low–low (first birth at low altitude and second birth at low altitude); low–high (first birth at low altitude and second birth at high altitude); high–high (first birth at high altitude and second birth at high altitude); and high–low (first birth at high altitude and second birth at low altitude). Means and 95% CIs of second birth weight in each scenario were estimated using multivariable regression while holding all other maternal- and birth-related factors constant, with mother and first and second birth characteristics set arbitrarily as such: age of mother at second birth = 28.5 years, education of mother = secondary school, male infants, first birth weight = 3300 g, year of second birth = 2001, time to previous birth = 32 months, gestational age of second birth = 40 weeks, and second birth length = 50 cm.
All analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Study population
Between 1984 and 2016, a total number of 2,769,811 births were recorded in Austria, among which 544,624 women with two births fulfilling inclusion criteria were identified and sequentially included in our analyses.
Sample characteristics
Table 1 summarizes characteristics of mothers and their two births. The average age of mothers at their second birth was 28.5 years (interquartile range (IQR): 7 years), which was 33 months (IQR: 29 months) from previous birth. The average altitude of the first and second birth were 410 m (IQR: 302 m), and 411 m (IQR: 300 m) respectively. Majority of mothers lived at altitude between 300 and 900 m for their first birth (Table 2). Overall change in residential altitudes between first and second birth was small. About 90% of mothers showed an altitude change smaller than about 60 m and 2% showed >300 m change in altitude. Table 2 describes the mean differences in altitude from the first to second birth of a same mother according to the first birth altitude.
Associations between maternal altitude and second birth weight
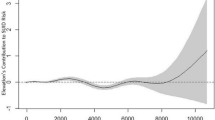
Table 3 shows prospective associations of maternal altitude with second birth weight in the multivariable regression model. Because this analysis focused on a longitudinal association of altitude with birth weight, results was described for main effects only but not for non-altitude-related variables. After adjusting for maternal characteristics and characteristics of the first and second birth, we found that first birth altitude, altitude ratio (second birth/first birth), and altitude ratio second birth/first birth were strong predictors for weight of the second birth. Sensitivity analyses according to sexes of two births returned similar results (Supplemental Tables S1 and S2).
To illustrate the effect size of these predictors, we estimated the means and 95% CIs of second born birth weight (g) depending on altitude of the first and second birth in four scenarios, adjusting for all significant predictors derived from the multivariable regression model (Fig. 1). The estimated second birth weight for low–low altitude mothers was 3567 g (95% CI: 3565, 3570). While for low–high altitude mothers, the second birth weight decreased to 3536 g (95% CI: 3523, 3548) by 32 g per 1000 m. For high–high altitude mothers, the estimated second birth weight was 3414 g (95% CI: 3412, 3418). However the estimated second birth weight increased to 3499 g (95% CI: 3480, 3517) for high–low altitude mothers by 84 g per 1000 m. The estimated second birth weight of high–low altitude mother is higher than of high–high altitude mothers, yet still lower than that of low–high altitude mothers’ second birth by 37 g per 1000 m. The estimated difference in second birth weight between low–low and high–high altitude mothers was 153 g per 1000 m.

Estimated means and 95% confidence intervals (CIs) of second born birth weight (g) depending on altitude of first and second born, adjusting for predictors derived from multivariable regression model (Table 3) (95% CI)
Discussion
Using longitudinal data, our population-based study shows a longitudinal effect of maternal altitude on birth weight. Our findings demonstrate the negative impact of high altitude on birth weight from first to second born siblings within the same mother living in Austria with low-to-moderate residential altitude. After taking consideration of maternal and infant characteristics, a 32-g decrease in birth weight was estimated per 1000 higher altitude (moving from an altitude of 200 m up to 1200 m). In contrast, a 84-g per 1000 increase in birth weight was estimated per 1000 m lower altitude (moving from 1200 m down to 200 m). Interestingly, among mothers who have moved between two births, the second birth weight was lower among those moved down and gave birth at a lower altitude compared to those moved up and gave second birth at a higher altitude.
To the best of our knowledge, this study is the first to report longitudinal associations between maternal altitude and birth weight, precluding a comparison with previous studies. Nevertheless, our finding on altitude-associated reduction in birth weight and the estimated effect size are consistent with that from cross-sectional studies. Previous studies have reported a 102–133 g decreased mean birth weight with 1000 m increased altitude in regions at medium-to-high altitude, with minimal model adjustments.17,23 Our group has previously demonstrated a crude estimate of 150 g decline in birth weight per 1000 m of altitude in Austrian mothers residing at low-to-medium (up to 1600 m) altitude.18 This is in line with the estimated difference in birth weight of 153 g per 1000 m between low–low and high–high mothers found in this study. Further, Wehby et al.21 reported a multivariable-adjusted estimation of 70–100 g decline in birth weight per 1000 m altitude ranging between 5 and 1280 m using “low-altitude” sample from South America. Taken together, the cross-sectional evidence on altitude-associated birth weight reduction is consistent in observations from very high altitude levels (2500 to 4500 m) to low and medium altitude (below 1500 m). Previous research has suggested a low birth weight paradox phenomenon, such that there is no impact on mortality from altitude-induced weight reduction among term babies.1 Nevertheless, the weight reduction might be detrimental among premature babies or negatively impact morbidity, which should be investigated in further studies.
The average duration between two births in our study was 33 months (IQR: 29 months). That is to say, in approximately 3 years of time, a relocation of a woman after the first birth may have a profound effect on the weight of her second birth. This effect is presented as 32 g weight reduction per 1000 m altitude ascending and 84 g weight gain per 1000 altitude descending of the second birth. Therefore, the impact of altitude on birth weight is a contingent process with a negative effect with elevating altitude.19 This finding has research and clinical and public health implications.
In the present study, we were able to estimate a smaller birth weight at lower altitude (high–low altitude mothers: 3499 g) compared to higher altitude (low–high altitude mothers: 3536 g), which depended on the altitude of first birth. This novel finding suggests that, although having lived in a low resident altitude area was not protective against weight reduction of a second birth at a higher altitude, these women remained having heavier second birth compared to those who moved from higher to lower residential altitude for the second birth. The mechanism of this phenomenon is not understood. We speculate a gene–environment interaction between altitude and birth weight, where the long-term genetic adaption to residential altitude is stronger than the short-term epigenetic adaption to altitude during the pregnancy. In addition, although a low birth weight paradox has been suggested, such that altitude affects birth weight but not infant mortality1 it is unclear whether this holds true for infants with smaller birth weight due to their mothers who moved from/to higher altitude. Further studies should use longitudinal design and robust measures of genetic and epigenetic markers to elucidate their associations.
This study has clinical and public health implications. Majority of previous studies have suggested a reduction in birth weight only after a certain threshold, ~2000 m, where the critical barometric pressure reaches a hypoxic effect. Clearly, previous cross-sectional studies (47) including ours18 and current longitudinal study have shown that reduction in fetal growth could occur at a moderate altitude of 1600 m. In the present time, global immigration is more than ever, with 1 billion people in the world today on the move.40 Therefore, the change in altitude alongside with migrations must be considered in maternal care for movers.
There are several strengths and limitations of this study. The main strength of this population-based study is the large sample size, gathering data on almost all live births in Austria over 33 years. We were able to adjust for a range of maternal characteristics (maternal age, education) and infant- and birth-related characteristics (sex, time to previous born, and gestational age and birth length of the second born). Although other specific maternal factors were not documented on birth certificates, data in the present analyses were analyzed longitudinally within each pair of siblings, ensuring that other mother-specific factors are automatically adjusted for. This approach mimicked a cross-over study design to address causal inference. Finally, Austria provides a free standardized national obstetrician-led pregnancy care. We do not expect much inequality of access to antenatal care or substantial differences in treatment. The limitation of our study is the lack of information between two births, including paternal biometric measures, gestational weight gain and nutrition, maternal hypertension, preeclampsia, cigarette smoking, alcohol consumption, and general morbidity of the mother. Such changes may occur in a small number of women.
Conclusion
In summary, our data demonstrate a clear longitudinal effect of altitude on birth weight within siblings of the same mother from first and second birth in a low-to-medium altitude European country. Further longitudinal studies should use robust measures of genetic and epigenetic markers to elucidate the gene–environmental interaction between altitude and birth weight. Finally, a profound effect of medium altitude on birth weight reduction should be noted in maternal care by taking consideration of women’s recent moving histories.
References
Wilcox, A. J. On the importance–and the unimportance–of birthweight. Int. J. Epidemiol. 30, 1233–1241 (2001).
Wilcox, A. J. & Russell, I. T. Birthweight and perinatal mortality: II. On weight-specific mortality. Int. J. Epidemiol. 12, 319–325 (1983).
Hack, M., Klein, N. K. & Taylor, H. G. Long-term developmental outcomes of low birth weight infants. Future Child 5, 176–196 (1995).
Richards, M., Hardy, R., Kuh, D. & Wadsworth, M. E. Birth weight and cognitive function in the British 1946 birth cohort: longitudinal population based study. BMJ 322, 199–203 (2001).
Steffensen, F. H. et al. Low birth weight and preterm delivery as risk factors for asthma and atopic dermatitis in young adult males. Epidemiology 11, 185–188 (2000).
Parkinson, J. R., Hyde, M. J., Gale, C., Santhakumaran, S. & Modi, N. Preterm birth and the metabolic syndrome in adult life: a systematic review and meta-analysis. Pediatrics 131, e1240–e1263 (2013).
Smith, C. J. et al. The impact of birth weight on cardiovascular disease risk in the Women’s Health Initiative. Nutr. Metab. Cardiovasc. Dis. 26, 239–245 (2016).
Calkins, K. & Devaskar, S. U. Fetal origins of adult disease. Curr. Probl. Pedia. Adolesc. Health Care 41, 158–176 (2011).
Crawford, M. A., Doyle, W. & Meadows, N. Gender differences at birth and differences in fetal growth. Hum. Reprod. 2, 517–520 (1987).
Kramer, M. S. Determinants of low birth weight: methodological assessment and meta-analysis. Bull. World Health Organ. 65, 663–737 (1987).
Khalil, A., Syngelaki, A., Maiz, N., Zinevich, Y. & Nicolaides, K. H. Maternal age and adverse pregnancy outcome: a cohort study. Ultrasound Obstet. Gynecol. 42, 634–643 (2013).
Fraser, A. M., Brockert, J. E. & Ward, R. H. Association of young maternal age with adverse reproductive outcomes. N. Engl. J. Med. 332, 1113–1117 (1995).
Spencer, N., Bambang, S., Logan, S. & Gill, L. Socioeconomic status and birth weight: comparison of an area-based measure with the Registrar General’s social class. J. Epidemiol. Community Health 53, 495–498 (1999).
Spracklen, C. N., Ryckman, K. K., Harland, K. & Saftlas, A. F. Effects of smoking and preeclampsia on birth weight for gestational age. J. Matern. Fetal Neonatal Med. 28, 679–684 (2015).
Hinkle, S. N. et al. The association between parity and birthweight in a longitudinal consecutive pregnancy cohort. Paediatr. Perinat. Epidemiol. 28, 106–115 (2014).
Stephenson, T. & Symonds, M. E. Maternal nutrition as a determinant of birth weight. Arch. Dis. Child Fetal Neonatal Ed. 86, F4–F6 (2002).
Jensen, G. M. & Moore, L. G. The effect of high altitude and other risk factors on birthweight: independent or interactive effects? Am. J. Public Health 87, 1003–1007 (1997).
Waldhoer, T. & Klebermass-Schrehof, K. The impact of altitude on birth weight depends on further mother- and infant-related factors: a population-based study in an altitude range up to 1600 m in Austria between 1984 and 2013. J. Perinatol. 35, 689–694 (2015).
Candelas, N. et al. Altitude effect on birth weight and prematurity in the Province of Catamarca (Argentina). Am. J. Hum. Biol. 27, 526–529 (2015).
Zahran, S., Breunig, I. M., Link, B. G., Snodgrass, J. G. & Weiler, S. A quasi-experimental analysis of maternal altitude exposure and infant birth weight. Am. J. Public Health 104(Suppl 1), S166–S174 (2014).
Wehby, G. L., Castilla, E. E. & Lopez-Camelo, J. The impact of altitude on infant health in South America. Econ. Hum. Biol. 8, 197–211 (2010).
Julian, C. G. et al. Augmented uterine artery blood flow and oxygen delivery protect Andeans from altitude-associated reductions in fetal growth. Am. J. Physiol. Regul. Integr. Comp. Physiol. 296, R1564–R1575 (2009).
Mortola, J. P., Frappell, P. B., Aguero, L. & Armstrong, K. Birth weight and altitude: a study in Peruvian communities. J. Pediatr. 136, 324–329 (2000).
Yip, R. Altitude and birth weight. J. Pediatr. 111, 869–876 (1987).
Lichty, J. A., Ting, R. Y., Bruns, P. D. & Dyar, E. Studies of babies born at high altitudes. I. Relation of altitude to birth weight. AMA J. Dis. Child 93, 666–669 (1957).
Howard, R. C., Lichty, J. A. & Bruns, P. D. Studies on babies born at high altitude. II. Measurement of birth weight, body length and head size. AMA J. Dis. Child 93, 670–674 (1957).
Lopez Camelo, J. S., Campana, H., Santos, R. & Poletta, F. A. Effect of the interaction between high altitude and socioeconomic factors on birth weight in a large sample from South America. Am. J. Phys. Anthropol. 129, 305–310 (2006).
Moore, L. G. Fetal growth restriction and maternal oxygen transport during high altitude pregnancy. High Alt. Med. Biol. 4, 141–156 (2003).
Moore, L. G. et al. Maternal adaptation to high-altitude pregnancy: an experiment of nature–a review. Placenta 25(Suppl A), S60–S71 (2004).
Julian, C. G. et al. Lower uterine artery blood flow and higher endothelin relative to nitric oxide metabolite levels are associated with reductions in birth weight at high altitude. Am. J. Physiol. Regul. Integr. Comp. Physiol. 295, R906–R915 (2008).
Wilson, M. J. et al. Greater uterine artery blood flow during pregnancy in multigenerational (Andean) than shorter-term (European) high-altitude residents. Am. J. Physiol. Regul. Integr. Comp. Physiol. 293, R1313–R1324 (2007).
Zamudio, S. et al. Maternal oxygen delivery is not related to altitude- and ancestry-associated differences in human fetal growth. J. Physiol. 582, 883–895 (2007).
Zamudio, S. et al. Hypoglycemia and the origin of hypoxia-induced reduction in human fetal growth. PLoS ONE 5, e8551 (2010).
Postigo, L. et al. Where the O2 goes to: preservation of human fetal oxygen delivery and consumption at high altitude. J. Physiol. 587, 693–708 (2009).
Julian, C. G. et al. High-altitude ancestry protects against hypoxia-associated reductions in fetal growth. Arch. Dis. Child Fetal Neonatal Ed. 92, F372–F377 (2007).
Julian, C. G. High altitude during pregnancy. Clin. Chest Med. 32, 21–31 (2011).
Aksoy, A. N., Batmaz, G., Dane, B., Kucur, S. K. & Gozukara, I. Effects of altitude changes on Doppler flow parameters for uterine, umbilical, and mid-cerebral arteries in term pregnancy: a pilot study. J. Turk. Ger. Gynecol. Assoc. 16, 237–240 (2015).
Krampl, E. et al. Fetal biometry at 4300 m compared to sea level in Peru. Ultrasound Obstet. Gynecol. 16, 9–18 (2000).
Statistik Austria Demographisches Jahrbuch (Statistik Austria, Vienna, 2012). http://wko.at/statistik/jahrbuch/2012_Deutsch.pdf. Accessed 22 Jul 2018.
The Lancet Public Health. No public health without migrant health. Lancet Public Health 3, e259 (2018).
Author information
Authors and Affiliations
Contributions
R.E. drafted the initial manuscript and reviewed the manuscript. T.W. designed the study, acquired and analysed the data, and reviewed the manuscript for important intellectual content. L.Y. designed the study, drafted the initial manuscript and reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Ertl, R., Waldhoer, T. & Yang, L. Moderate altitude impacts birth weight: 30 years retrospective sibling analyses using record linkage data. Pediatr Res 86, 403–407 (2019). https://doi.org/10.1038/s41390-019-0434-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-019-0434-4
