
Abstract
Background
Early measures of cognitive function are of great public health interest. We aimed to estimate the association between head circumference at birth, a measure of cerebral size, and school performance.
Methods
We conducted a nationwide cohort study of all liveborn singletons in Denmark, 1997–2005. The association between birth head circumference z score and test scores in reading and mathematics from a nationwide mandatory computer-based school test program (7–16 years) was estimated by multivariable linear regression adjusted for potential confounders.
Results
The cohort included 536,921 children. Compared to normocephalic children, children with microcephaly [<−2 standard deviations (SD)] had lower mean reading scores: second grade: −0.08 SD (95% CI −0.10 to −0.06), eighth grade: −0.07 SD (95% CI −0.10 to −0.04). Macrocephaly (>+2 SD) was associated with higher scores. In normocephalic children, each SD increase in head circumference was associated with a 0.03 SD (95% CI 0.03 to 0.04) increase in mean reading scores. The results were similar across grades within both reading and mathematics.
Conclusion
Prenatal brain growth may be causally related to childhood school performance. The demonstrated differences are unlikely to be clinically relevant at the individual level but may be important at a public health level.
Similar content being viewed by others
Introduction
Understanding the determinants of childhood cognition and the factors underlying important abilities such as reading and mathematics is of great importance to both the individual and the society. Cognitive function is a result of complex genetic and environmental influences, and especially environmental factors may be targets for preventive strategies.1
Measures of prenatal brain growth and development, which are highly sensitive to a range of environmental factors,2 have gained interest as possible determinants of later cognitive function.3,4,5,6,7,8,9,10,11,12,13,14,15,16 Head circumference at birth is a widely available proxy measure reflecting fetal brain growth17,18,19 during the period with the most rapid growth of the developing human brain.2
Large studies have reported associations between small head circumference at birth and poorer intellectual performance in young adulthood.3,4,5,6,7 Some studies found no association in children between 8 and 10 years,8,9,10 whereas one study found an association at 4 but not at 8 years.11 Another study found an association with some cognitive abilities, but no association with others.12 Other studies reported associations between head circumference at birth, intelligence,13,14 and other measures of cognitive function in school-aged children.15,16 Many of these studies were limited by small sample sizes.8,9,10,11,12,14 The association with different aspects of school performance including skills in reading and mathematics, practical every day measures of cognitive function, remains widely unexplored.
We conducted a large nationwide, population-based cohort study to investigate the association between the full range of head circumference at birth, including head circumference relative to birth weight, and school performance in reading and mathematics.
Methods
Study cohort
We identified all live births in Denmark from 1 January 1997 to 31 December 2005 in the Danish Medical Birth Registry.20 In Denmark, unique personal identification numbers enable linkage of individual data from mothers and newborns to all nationwide Danish registries. To be eligible for the study, mothers and infants had to have valid personal identification numbers. We included singletons with no diagnoses of major malformations, congenital syndromes, or teratogenic conditions, with no record of maternal alcohol exposure during pregnancy, and a gestational age at birth between 22 and 45 weeks (for details, see Supplementary Methods and Supplementary Table S1).
Head circumference
Head circumference and gestational age at birth were identified in the Danish Medical Birth Registry. Occipitofrontal head circumference has been measured with a measuring tape and recorded immediately after birth by the attending midwife for all newborns since 1997. Based on the present dataset, head circumference z scores were calculated according to gender and gestational age at birth and categorized into three groups: microcephaly [<−2 standard deviations (SD)], normocephaly (−2 SD to 2 SD), and macrocephaly (>2 SD). Measurements <−5 or >5 SD were considered to be implausible and set to missing. In 2000, >93% of the recordings of gestational age at birth were based on ultrasound measurements during early pregnancy.21 We identified implausible values of gestational age using a recent United States algorithm22 and replaced them by estimates based on the last menstrual period if available. The remaining implausible values were considered missing.
School performance
In Denmark, school attendance is compulsory for all children between the ages of 6–7 years and 16 years.23 Approximately 81% of all children attend public schools free of charge.24 As an individual evaluation tool, a national test program was introduced in public schools in 2010. The program consists of ten mandatory tests carried out annually from the second through the eighth grade (8–15 years). Reading abilities are tested every second year (second to eighth grade) and mathematic abilities in the third and sixth grade. The tests are performed online and are adaptive, using questions of varying difficulty based on the answer to the previous questions.25
The raw test results are reported on a continuous logit scale. Descriptive statistics of the distribution of test results by reading/mathematics, test year, and grade (2010–2012) have been published.25 In accordance with the previous work,25 we calculated standardized mean test scores within each annual test of reading and mathematics. The test scores were standardized to a mean of 0 and a standard deviation (SD) of 1. The data were provided by the National Agency for IT and Learning.26 The use of the tests has previously been validated.25
Covariates
Covariates were obtained from several nationwide registries, including the Danish Medical Birth Registry [birth weight, birth year, sex of the child, parity, plurality, maternal age, smoking during pregnancy, and pre-pregnancy body mass index (BMI)]. The origin of the child was determined using data from the Danish Civil Registration System (see Supplementary Methods).27 Information on maternal morbidity and medication was obtained from the Danish National Patient Registry, the Danish National Prescription Registry, and the Danish Psychiatric Central Registry. Maternal morbidities were defined in accordance with previous studies and included chronic hypertension, diabetes mellitus, any psychiatric disease, and epilepsy treated with antiepileptic drugs (see Supplementary Methods for further details).27,28,29 Information on pre-pregnancy education, income, and parental cohabitation status was obtained from Statistics Denmark. The educational level was categorized into seven groups according to the parent with the highest achieved or ongoing level of education. Income was calculated as the equivalence weighted disposable income of the family corrected for inflation according to the Danish Consumer Price Index.30
Statistical analyses
The association between head circumference z score at birth and test scores of either reading or mathematics was analyzed using crude and adjusted multivariable linear regression, accounting for clusters of siblings within the mothers using robust standard errors. In the primary analysis, we estimated the standardized mean difference in test scores comparing microcephalic and macrocephalic children at birth to normocephalic children. In a secondary analysis, we depicted the association between the head circumference z scores and the absolute standardized mean test scores using restricted cubic splines. Further, we restricted the analyses to normocephalic children and estimated the linear association between head circumference z score and the standardized test scores. Finally, we calculated the difference between the head circumference and the birth weight z scores, a measure of the proportionality of the newborn,27 and estimated the association with the standardized test scores. Furthermore, in accordance with previous studies, we also conducted analyses stratified by preterm birth (<37 weeks). Moreover, for comparison, we repeated the analyses with birth weight z score as the independent variable.
Based on knowledge from previous studies, causal diagrams for observational research were used to identify potential confounders.31 The adjusted model included the following variables: Child: sex, birth year (restricted cubic spline), and origin (non-western, western, Danish); Maternal: smoking (yes/no), nulliparity (yes/no), age (restricted cubic spline), and pre-pregnancy medical diseases, including hypertension (yes/no), diabetes mellitus (yes/no), and psychiatric disorders (yes/no), antiepileptic drug use during pregnancy (yes/no); Parental: income (restricted cubic spline), cohabitation status (single/couple), and educational level (seven categories).
Missing values for head circumference, test scores, and covariates were handled by multiple imputation. Given the extensive information on variables predicting missing information including perinatal and socioeconomic factors as well as diagnoses of childhood developmental disorders, the assumption of missing at random was considered fulfilled. The highest proportion of missing values for any variable was 24% and most variables had <5% missing values (see Supplementary Methods and Supplementary Table S2).
We conducted several preplanned sensitivity analyses. To account for unmeasured family or maternal factors, we conducted sibling analyses restricting the population to mothers with at least two children subjected to similar tests. A fixed effects linear mixed model was applied to assess the association within the siblings. BMI, a potential confounder, was only recorded since 2004 and consequently missing in 80% of participants. To assess the impact of not including maternal BMI, analyses were repeated in observations with available BMI, adjusting for BMI in addition to the other covariates in the fully adjusted model. Further, we conducted sensitivity analyses adjusting for age at testing. To assess the impact of the applied definition of microcephaly and macrocephaly, a sensitivity analysis was carried out defining microcephaly and macrocephaly as <−3 SD and >3 SD, respectively. Finally, complete case analyses, only including children with complete data on all covariates, were conducted.
All analyses were conducted on a Statistics Denmark server using Stata version 14. The study was approved by the Danish Data Protection Agency (reference 1-16-02-385-16).
Results
The study included 536,921 children born alive in Denmark during the study period, of which 441,970 (82%) had at least one test result (see Fig. 1). Overall, 24% of the test results of any test were missing. Among children with a diagnostic code of developmental delay or intellectual disability, 55% (second grade) and 49% (eighth grade) had available test results, whereas 82% (second grade) and 83% (eighth grade) of children without these diagnoses had available test results. Supplementary Table S3 lists characteristics of mothers and infants according to the availability of test results. The characteristics of the mothers and infants according to the presence of microcephaly, normocephaly, and macrocephaly are listed in Table 1. Two hundred and sixty-three thousand five hundred and fifteen (49%) of the newborns were female. The mean head circumference at birth was 35.2 cm. According to gestational age, 10,325 children were microcephalic, 13,882 children were macrocephalic, and 493,848 were normocephalic.

Infants with a record of harmful maternal alcohol exposure during pregnancy or a diagnosis of fetal alcohol syndrome are included in the malformations/syndromes/teratogenicity group.
Microcephaly, macrocephaly, and school performance
After adjustment for potential confounders, the mean difference in standardized second and eighth grade reading scores for children born with microcephaly was −0.08 SD (95% confidence interval (CI) −0.10 to −0.06) and −0.07 SD (95% CI −0.10 to −0.04), respectively, compared to normocephalic children. The mean differences for macrocephalic children in standardized second and eighth grade reading scores was 0.06 SD (95% CI, 0.04 to 0.07) and 0.05 SD (95% CI 0.03 to 0.07), respectively. Similar results were found for the other tests in reading and mathematics (Fig. 2).

The comparison group was infants born with normocephaly. The estimates shown in the figure are adjusted for infant sex, birth year, origin, maternal smoking, parity, age, maternal diseases, parental income, educational level, and cohabitation status. No. indicates the number of individuals included in the analyses, CI confidence interval.
The association between all variables included in the model and the mean difference in second grade reading scores are depicted in Fig. 3. These associations were similar through the different grades and across reading and mathematics.

The estimates of all covariates were mutually adjusted for all the remaining covariates in the model. CI confidence interval.
The full range of head circumference and school performance
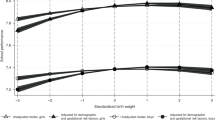
The association between head circumference z score at birth and the absolute standardized mean test score is illustrated in Fig. 4 using restricted cubic splines after adjustment for potential confounders. Overall, Fig. 4 indicates that larger head circumference is associated with higher mean test scores, although a tendency toward a decline in the higher end of the head circumference z score distribution cannot be ruled out, in particular for math test scores.

Restricted cubic splines adjusted for infant sex, birth year, origin, maternal smoking, parity, age, disease (diabetes mellitus, antiepileptic drug use during pregnancy, chronic hypertension, and psychiatric illness), parental income, educational level, and cohabitation status. The grey area depicts the predicted 95% confidence interval.
Head circumference and school performance in normocephalic children
In the normocephalic children, the mean test scores increased with increasing head circumference after adjustment for potential confounders (Supplementary Table S4). For reading in the second and eighth grade, the mean increase in test scores was similar: 0.03 SD (95% CI, 0.03–0.04) per SD increase in head circumference z score at birth. Similar results were found for the other tests in reading and mathematics.
Additional analyses
Head circumference z score at birth minus birth weight z score was not associated with any difference in standardized test scores (Supplementary Table S5). The results of the sibling analyses were similar to those of the primary analyses (Supplementary Table S6). Additional adjustment for BMI or age at testing did not substantially change the estimates. Using ±3 SD as a cut off for microcephaly and macrocephaly, the associations for microcephaly were somewhat stronger, whereas the associations for macrocephaly remained similar (Supplementary Table S7). Stratified by preterm birth, the results were similar regarding macrocephalic children (Supplementary Table S8). In microcephalic children, the results were similar in the lower grades. However, the mean difference in standardized eighth grade reading scores for children born at term was −0.07 SD (95% CI, −0.10 to −0.04), whereas the estimate for those born preterm was −0.20 SD (95% CI, −0.34 to −0.06) compared to normocephalic children. The same tendency was found for mathematics. The results of the analyses using birth weight z score as the independent variable were similar to the analyses of head circumference z score (Supplementary Table S9). The results of the complete case analyses were similar to the main analyses (Supplementary Table S10).
Discussion
In this population-based, nationwide cohort study, head circumference at birth, a measure of prenatal cerebral growth, was associated with school performance. Overall, microcephaly was associated with impaired school performance and macrocephaly was associated with improved school performance, even though a tendency toward a decline in math test scores in the higher end of the head circumference z score distribution cannot be ruled out (Fig. 4). In normocephalic children, larger head circumference was also associated with higher test scores. Similar results were found in reading and mathematics, from the second to the eighth grade.
Our findings are in accordance with results from other large studies investigating the association between head circumference at birth and measures of intellectual performance in young adulthood.3,4,5,6 These studies were conducted in partly overlapping cohorts of Swedish male conscripts and reported associations between small head circumference at birth and poorer intellectual performance. Furthermore, one of the studies reported increasingly poorer intellectual performance with decreasing head circumference z score in the lower range of the z score distribution, but no difference with increasing head circumference z score in the higher range.5 This is in line with our results defining microcephaly and macrocephaly at ±3 SD. Accordingly, the degree of microcephaly at birth may be important for the cognitive function during childhood, whereas the degree of macrocephaly may not be of major importance.
Few studies have investigated the association between head circumference at birth and school performance in children. A study from Western Australia in government schools among 8-year-old children showed an association between larger head circumference at birth and better literacy outcomes.15 Another study from the United Kingdom found that larger head circumference at birth was associated with an increased chance of attaining a college or university degree.32 Most other studies of the association between head circumference at birth and cognitive function in school-aged children measured the intelligence quotient (IQ). However, measurements of intelligence and education are known to be correlated.33 The association between head circumference at birth and childhood IQ has been less clear. Some studies found no association between head circumference at birth and cognitive function in 8–10-year-old children.8,9,10 However, these studies were likely underpowered to detect the associations we report. Other larger studies found associations between head circumference at birth and intelligence in 7–9-year-old children.13,16
One study investigated whether the association between head circumference at birth and intelligence at conscription was modified by preterm birth.5 Among preterm infants, the authors reported a stronger association compared to infants born at term. In our study, the mean difference in standardized test scores for microcephalic children compared to normocephalic children was similar in preterm and term births in the lower grades. However, in the higher grades, microcephaly was more strongly associated with poorer school performance in preterm children, potentially indicating that preterm birth has a more detrimental influence on cognitive function in children born with measures of impaired prenatal cerebral growth. Alternatively, this finding may be due to the fact that children born preterm are smaller than fetuses remaining in utero at the same gestational age, i.e., microcephaly in a child born preterm may indicate more severe prenatal cerebral growth impairment.34
Another study found head circumference at birth to be more strongly associated with IQ than with birth weight.14 Anthropometric measures at birth are highly correlated, and therefore accounting for the overall size of the newborn when studying the impact of head circumference is difficult. We found no association between the proportionality of the newborn (head circumference z score minus birth weight z score) and school performance. Further, we found no clear indications that head circumference z score was more strongly associated with cognitive function than with birth weight z score. Thus, based on the available data, we cannot exclude that the demonstrated associations between smaller head circumference and lower test scores might be due to smaller birth size in general.
Observational studies are always prone to unmeasured confounding. However, in the present study we were able to adjust for a number of potentially important confounders, and further, we were able to perform sibling analyses, which hold the potential to control for time-stable maternal, genetic, environmental, and intrauterine factors. In the sibling analyses, the estimates remained largely unchanged or were slightly attenuated, in accordance with the findings by Bergvall et al.5,6 who found the association between head circumference at birth and intellectual performance to be only partly explained by social and familial factors.6
We included a nationwide cohort of all singletons born alive, minimizing the possibility of selection bias at baseline. However, the inclusion of live births only may have attenuated our results due to live birth bias.35 Furthermore, children not attending public school were by definition lost to follow-up. To minimize the possibility of bias, missing data and loss to follow-up were handled by multiple imputation under the assumption of missing at random.36
Several studies have found head circumference at birth to correlate highly with brain size,17,18,19 and head circumference at birth is thought to serve as a good proxy of prenatal brain growth. Generally, head circumference at birth is considered to be an accurate measure,37,38,39 but some degree of non-differential measurement error is likely present.40 The results of reading and math tests are fully computerized, blinded to the exposure status. Regarding both head circumference and test outcomes, any measurement error is unlikely to be differential, and thus any measurement error would most likely have attenuated our results. The remaining variables included in the study relied on combinations of information from several high-quality nationwide Danish registries. Accordingly, the associations reported in the present study are unlikely to be explained by confounding, selection bias, or information bias.
Although head circumference at birth serves as a proxy of prenatal brain growth, it tells nothing about the timing of the intrauterine growth of the brain. Future studies should include head circumference measurements from different time periods during pregnancy to study whether specific prenatal periods may be more critical for later cognitive function.
Conclusion
In this large, population-based study, smaller head circumference was associated with poorer school performance, whereas larger head circumference was associated with improved school performance. This association was also seen in normocephalic children. These associations were present throughout the second to the eighth grade for both reading and mathematics. No degree of macrocephaly was found to be associated with poorer school performance. However, a tendency toward a decline in math test scores in the higher end of the head circumference z score cannot be ruled out. Associations between birth weight z score and cognitive function were similar to those demonstrated for head circumference z score.
Our results suggest that prenatal brain growth may be related to intellectual abilities, although only relatively small effect sizes were found. The association between head circumference z score at birth and school performance is unlikely to be clinically relevant. However, a cause of even small shifts in the intelligence distribution of the general population may be of overall public health concern.
References
Shenkin, S. D., Starr, J. M. & Deary, I. J. Birth weight and cognitive ability in childhood: a systematic review. Psychol. Bull. 130, 989–1013 (2004).
Stiles, J. & Jernigan, T. L. The basics of brain development. Neuropsychol. Rev. 20, 327–348 (2010).
Lundgren, E. M., Cnattingius, S., Jonsson, B. & Tuvemo, T. Intellectual and psychological performance in males born small for gestational age with and without catch-up growth. Pediatr. Res. 50, 91–96 (2001).
Lundgren, E. M., Cnattingius, S., Jonsson, B. & Tuvemo, T. Birth characteristics and different dimensions of intellectual performance in young males: a nationwide population-based study. Acta Paediatr. 92, 1138–1143 (2003).
Bergvall, N., Iliadou, A., Johansson, S., Tuvemo, T. & Cnattingius, S. Risks for low intellectual performance related to being born small for gestational age are modified by gestational age. Pediatrics 117, e460–e467 (2006).
Bergvall, N., Iliadou, A., Tuvemo, T. & Cnattingius, S. Birth characteristics and risk of low intellectual performance in early adulthood: are the associations confounded by socioeconomic factors in adolescence or familial effects? Pediatrics 117, 714–721 (2006).
Raikkonen, K. et al. Growth trajectories and intellectual abilities in young adulthood: the Helsinki Birth Cohort study. Am. J. Epidemiol. 170, 447–455 (2009).
Fattal-Valevski, A. et al. Growth patterns in children with intrauterine growth retardation and their correlation to neurocognitive development. J. Child Neurol. 24, 846–851 (2009).
Gale, C. R., OʼCallaghan, F. J., Godfrey, K. M., Law, C. M. & Martyn, C. N. Critical periods of brain growth and cognitive function in children. Brain 127(Pt 2), 321–329 (2004).
Lira, P. I. et al. Early head growth: relation with IQ at 8 years and determinants in term infants of low and appropriate birthweight. Dev. Med. Child Neurol. 52, 40–46 (2010).
Gale, C. R., OʼCallaghan, F. J., Bredow, M. & Martyn, C. N. The influence of head growth in fetal life, infancy, and childhood on intelligence at the ages of 4 and 8 years. Pediatrics 118, 1486–1492 (2006).
Veena, S. R. et al. Association of birthweight and head circumference at birth to cognitive performance in 9- to 10-year-old children in South India: prospective birth cohort study. Pediatr. Res. 67, 424–429 (2010).
Broekman, B. F. et al. The influence of birth size on intelligence in healthy children. Pediatrics 123, e1011–e1016 (2009).
Emond, A. M., Lira, P. I., Lima, M. C., Grantham-McGregor, S. M. & Ashworth, A. Development and behaviour of low-birthweight term infants at 8 years in northeast Brazil: a longitudinal study. Acta Paediatr. 95, 1249–1257 (2006).
Malacova, E. et al. Neighbourhood socioeconomic status and maternal factors at birth as moderators of the association between birth characteristics and school attainment: a population study of children attending government schools in Western Australia. J. Epidemiol. Community Health 63, 842–849 (2009).
Christian, P. et al. Associations between preterm birth, small-for-gestational age, and neonatal morbidity and cognitive function among school-age children in Nepal. BMC Pediatr. 14, 58 (2014).
Cooke, R. W., Lucas, A., Yudkin, P. L. & Pryse-Davies, J. Head circumference as an index of brain weight in the fetus and newborn. Early Hum. Dev. 1, 145–149 (1977).
Lemons, J. A., Schreiner, R. L. & Gresham, E. L. Relationship of brain weight to head circumference in early infancy. Hum. Biol. 53, 351–354 (1981).
Bray, P. F., Shields, W. D., Wolcott, G. J. & Madsen, J. A. Occipitofrontal head circumference–an accurate measure of intracranial volume. J. Pediatr. 75, 303–305 (1969).
Knudsen, L. B. & Olsen, J. The Danish Medical Birth Registry. Dan. Med. Bull. 45, 320–323 (1998).
Jorgensen, F. S. [Ultrasonography of pregnant women in Denmark 1999-2000. Description of the development since 1980–1990]. Ugeskr. Laeger 165, 4409–4415 (2003).
Talge, N. M., Mudd, L. M., Sikorskii, A. & Basso, O. United states birth weight reference corrected for implausible gestational age estimates. Pediatrics 133, 844–853 (2014).
Ministry for Children Education and Gender Equality. The Folkeskole http://eng.uvm.dk/Education/Primary-and-lower-secondary-education/The-Folkeskole (2016). Accessed 22 Jun 2016.
Ministry for Children Education and Gender Equality. Elevtal i folkeskolen og frie skoler. (https://www.uvm.dk/Service/Statistik/Statistik-om-folkeskolen-og-frie-skoler/Statistik-om-elever-i-folkeskolen-og-frie-skoler/Elevtal-i-folkeskolen-og-frie-skoler (2016). Accessed 22 Jun 2016.
Beuchert, L. V. & Nandrup, A. B. The Danish National Tests–A Practical Guide (Department of Economics, University of Aarhus, 2014).
National Agency for IT and Learning, Ministry of Education. http://eng.uvm.dk/the-ministry/the-ministry/national-agency-for-it-and-learning. Accessed 31 May 2018.
Matthiesen, N. B. et al. Congenital heart defects and indices of fetal cerebral growth in a nationwide cohort of 924 422 liveborn infants. Circulation 133, 566–575 (2016).
Olsen, M., Sorensen, H. T., Hjortdal, V. E., Christensen, T. D. & Pedersen, L. Congenital heart defects and developmental and other psychiatric disorders: a Danish nationwide cohort study. Circulation 124, 1706–1712 (2011).
Molgaard-Nielsen, D., Pasternak, B. & Hviid, A. Oral fluconazole during pregnancy and risk of birth defects. N. Engl. J. Med. 369, 2061–2062 (2013).
Statistics Denmark. Consumer Price Index. http://www.dst.dk/en/Statistik/dokumentation/documentationofstatistics/consumer-price-index. Accessed 27 Jun 2016.
Greenland, S., Pearl, J. & Robins, J. M. Causal diagrams for epidemiologic research. Epidemiology 10, 37–48 (1999).
Hagenaars, S. P. et al. Shared genetic aetiology between cognitive functions and physical and mental health in UK Biobank (N = 112 151) and 24 GWAS consortia. Mol. Psychiatry 21, 1624–1632 (2016).
Deary, I. J. & Johnson, W. Intelligence and education: causal perceptions drive analytic processes and therefore conclusions. Int. J. Epidemiol. 39, 1362–1369 (2010).
Wilcox, A. J., Weinberg, C. R. & Basso, O. On the pitfalls of adjusting for gestational age at birth. Am. J. Epidemiol. 174, 1062–1068 (2011).
Liew, Z., Olsen, J., Cui, X., Ritz, B. & Arah, O. A. Bias from conditioning on live birth in pregnancy cohorts: an illustration based on neurodevelopment in children after prenatal exposure to organic pollutants. Int. J. Epidemiol. 44, 345–354 (2015).
Sterne, J. A. et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ 338, b2393 (2009).
Cheikh Ismail, L., Knight, H. E., Ohuma, E. O., Hoch, L. & Chumlea, W. C. Anthropometric standardisation and quality control protocols for the construction of new, international, fetal and newborn growth standards: the INTERGROWTH-21st Project. BJOG 120(Suppl 2), 48–55, v (2013).
West, J., Manchester, B., Wright, J., Lawlor, D. A. & Waiblinger, D. Reliability of routine clinical measurements of neonatal circumferences and research measurements of neonatal skinfold thicknesses: findings from the Born in Bradford study. Paediatr. Perinat. Epidemiol. 25, 164–171 (2011).
WHO Multicentre Growth Reference Study Group. Reliability of anthropometric measurements in the WHO Multicentre Growth Reference Study. Acta Paediatr. Suppl. 450, 38–46 (2006).
Bhushan, V. & Paneth, N. The reliability of neonatal head circumference measurement. J. Clin. Epidemiol. 44, 1027–1035 (1991).
Acknowledgements
Financial support covering salaries and purchase of data was provided by the Perinatal Epidemiology Research Unit, Aarhus University Hospital and Department of Clinical Medicine, Aarhus University.
Author information
Authors and Affiliations
Contributions
N.B.M. was the main author responsible for the acquisition of the data, contributed to the conception and the design of the study, the implementation of epidemiological methods, the performance and the interpretation of data analyses, and drafted the initial manuscript and revised the manuscript. C.C.B. contributed to the conception and the design of the study, the implementation of epidemiological methods, the performance and the interpretation of data analyses, and drafted the initial manuscript and revised the manuscript. T.B.H. contributed to the conception of the study, the interpretation of the analyses, secured the funding for the study, and reviewed and revised the manuscript. R.T.L. contributed to the design of the study, the data analyses, and the interpretation of the results, drafted the initial manuscript, and revised the manuscript. K.A. contributed to the design of the study, the data analyses, the interpretation of the results, and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Bach, C.C., Henriksen, T.B., Larsen, R.T. et al. Head circumference at birth and school performance: a nationwide cohort study of 536,921 children. Pediatr Res 87, 1112–1118 (2020). https://doi.org/10.1038/s41390-019-0683-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-019-0683-2
This article is cited by
-
Kindergarten dust heavy metal(loid) exposure associates with growth retardation in children
Environmental Science and Pollution Research (2023)
-
Development of a nutritional risk screening tool for preterm children in outpatient settings during a complementary feeding period: a pilot study
BMC Pediatrics (2022)
-
Dynamics of human milk oligosaccharides in early lactation and relation with growth and appetitive traits of Filipino breastfed infants
Scientific Reports (2022)
-
Head circumference trajectories during the first two years of life and cognitive development, emotional, and behavior problems in adolescence: a cohort study
European Journal of Pediatrics (2022)
-
Decreased head circumference at birth associated with maternal tobacco smoke exposure during pregnancy on the Japanese prospective birth cohort study
Scientific Reports (2021)
