
Abstract
Triplet-drug regimen bortezomib–thalidomide–dexamethasone (VTD) and bortezomib–lenalidomide–dexamethasone (VRD) are considered as standard of care induction prior autologous stem-cell transplantation (ASCT) in myeloma. In addition to improve response rate, induction therapy should preserve an adequate stem-cell collection. In the present retrospective study, we analyzed stem-cell collection in 325 newly diagnosed myeloma patients who received either VTD or VRD induction before ASCT. Stem-cell mobilization consisted of intravenous cyclophosphamide plus G-CSF. Plerixafor was administered preemptively to rescue mobilization. In comparison with VTD, VRD induction was associated with a more frequent use of plerixafor (19.3% versus 5.4%, p = 0.004) and with an increased number of apheresis to reach adequate collection (>2 apheresis required in 42.3% versus 30.2%, p = 0.05). Moreover, more patients experienced collection failure in the VRD group (6% versus 1.8%, p = 0.004). The median number of CD34-positive cells (×106/kg) was lower in the VRD group: 8.5 versus 9.3 (p = 0.05) in the VTD group. The vast majority of patients underwent ASCT (93% versus 98%, in VRD and VTD group, respectively). These data highlight the need of optimal stem-cell collection strategy, especially in the context of tandem transplantation and incorporation of anti-CD38 monoclonal antibody into induction.
Similar content being viewed by others

Introduction
Autologous stem-cell transplantation (ASCT) is considered as the standard of care for transplant-eligible patients with newly diagnosed multiple myeloma (NDMM) [1]. In the past years, the efficacy of induction therapy prior ASCT has been strongly improved, and triplet combination containing both proteasome inhibitor and immunomodulatory agent is now considered as the standard of care [2]. The triplet combination bortezomib, thalidomide, and dexamethasone (VTD) demonstrated strong efficacy and is approved for the treatment of transplant-eligible NDMM patients [3, 4]. The induction regimen bortezomib, lenalidomide, and dexamethasone (VRD) resulted in high response rate with favorable safety profile and is also considered as a standard of care prior ASCT for de novo MM patients [1, 5, 6]. In addition to improve response rate, induction therapy should preserve an adequate stem-cell collection in order to ensure the feasibility of ASCT. In the present study, we retrospectively analyzed stem-cell collection performed in our institution for newly diagnosed myeloma patients who received either VTD or VRD induction therapy between 2009 and 2019.
Material and methods
Patients and induction therapy
We conducted a retrospective institutional review board-approved analysis of all consecutive patients who fulfilled the following criteria: (i) diagnosis of symptomatic multiple myeloma according to international criteria [7], (ii) eligible for high-dose melphalan followed by ASCT, (iii) treated with at least three cycles of VTD or VRD induction, and (iv) received stem-cell mobilization. Patients treated in the context of clinical trials were excluded from the study. VTD induction consisted of bortezomib 1.3 mg/m2 SC (day 1, 4, 8,and 11), thalidomide 100 mg/day, and dexamethasone 20 mg (day 1–2, 8–9, J15–16, and 22–23) (28-day cycle). VRD induction consisted of bortezomib 1.3 mg/m2 SC (day 1, 4, 8, and 11), lenalidomide 25 mg (day 1–14), and dexamethasone 20 mg (day 1–2, 4–5, 8–9, and 11–12) (21-day cycle).
Stem-cell mobilization and harvesting
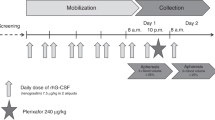
Stem-cell mobilization consisted of intravenous cyclophosphamide (3 g/m2) followed by G-CSF administered at a dose of 10 μg/kg/day subcutaneously starting 24 h after cyclophosphamide administration until peripheral blood stem-cell collection (planned at day 10 post cyclophosphamide). Apheresis was performed at least 3 weeks after the last dose of lenalidomide. Apheresis for peripheral blood stem-cell harvesting was performed until an optimal harvest of ≥5.106 CD34/kg [8]. Plerixafor (0.24 mg/kg) was administered preemptively to rescue mobilization in patients with blood CD34-positive cells <15/mm3 at time of apheresis. Collection failure was defined by stem-cell harvest <2.106 CD34/kg. Stem-cell harvesting was performed at Etablissement Français du Sang, Nantes, France.
Statistical analysis
The Fisher test was used to compare parameters between VTD and VRD groups. All p values were two-tailed. The significance level was set at 5% and statistical analyses were carried out using R Software version 3.0 R Development Core Team (2015). R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria, ISBN 3-900051-07-0, http://www.R-project.org/.
Results
Patient characteristics
From January 2009 to December 2019, 325 patients with previously untreated symptomatic MM who received at least three cycles of VTD or VRD before stem-cell mobilization were identified. The characteristics of patients are summarized in Table 1. Two hundred and forty-two (74.5%) patients received VTD induction and 83 (25.5%) patients received VRD induction. The median age (61, range 25–71) was similar in both groups. Reflecting the change of practice over the past years, VTD was the predominant induction regimen before 2018 and VRD induction was used instead of VTD. Patients received a median number of four cycles before stem-cell collection.
Plerixafor use and apheresis
All patients received stem-cell mobilization with cyclophosphamide (3 g/m2) plus G-CSF. Apheresis was planned 10 days after cyclophosphamide. Plerixafor was added to rescue the mobilization failure in 29 (8.9%) patients (Table 1). The plerixafor use was more frequent in patients receiving VRD induction (n = 16/83, 19.3%) in comparison with patients receiving VTD (n = 13/242, 5.4%), p = 0.0004) (Fig. 1). Moreover, 33/83 (42.3%) patients needed at least two apheresis to reach adequate stem-cell collection after VRD induction, versus 73/242 (30.2%) patients after VTD induction (p = 0.05).

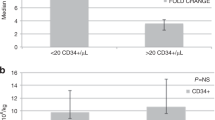
a Impact of VTD or VRD induction on Plerixafor use and number of apheresis. b Impact of VTD or VRD induction on stem-cell yield. VTD bortezomib, thalidomide, dexamethasone, VRD bortezomib, lenalidomide, dexamethasone.
Stem-cell collection failure and stem-cell yield
Six (1.8%) patients experienced stem-cell collection failure, 5/83 patients (6%) in the VRD group, and 1/242 patient (0.4%) in the VTD group (p = 0.004). The median number of CD34-positive cells was slightly higher in the VTD group: 9.3 versus 8.5 × 106 in the VRD group (p = 0.05). Among patients with autologous stem-cell harvest >2.106 CD34/kg (n = 319), stem-cell harvest was insufficient for tandem transplantation (>4 × 106 CD34/kg) in two patients (2.6%) in the VRD arm versus six patients (2.5%). Ninety-eight percent and ninety-three percent of patients actually underwent ASCT in the VTD and VRD group, respectively.
Discussion
To the best of our knowledge, the present real-life single-center retrospective study is the first to compare autologous stem-cell collection following either VTD or VRD induction therapy in patients with de novo MM. Despite the biases inherent to the retrospective design of the study, all patients received homogenous mobilization using cyclophosphamide (3 g/m2) plus G-CSF, which is considered as a standard of care [9, 10]. Plerixafor has been shown to improve stem-cell mobilization in patients with multiple myeloma [11]. Stem-cell mobilization with cyclophosphamide (1.5 g/m2) plus G-CSF versus plerixafor plus G-CSF in the era of novel agents has been recently compared [12]. In this study from Chaudhary and colleagues, mobilization with plerixafor plus G-CSF was found to be more effective in terms of CD34-positive cells collection. In our institution, a preemptive use of plerixafor in addition with Cyclophosphamide + G-CSF was performed. The efficacy of such an approach has been reported [13]. Our study confirmed that stem-cell collection following both VTD and VRD induction allowed the completion of ASCT in the vast majority of patients (98% and 93%, respectively). The feasibility of stem-cell collection after VTD or VRD induction has been confirmed in the context of phase-3 studies [1, 4]. However, our study revealed that VRD induction was associated with a higher plerixafor use with a 4:1 ratio in comparison with VTD, which imply a cost increase for the procedure, as recently published [14, 15]. Moreover, stem-cell collection after VRD induction required a higher number of apheresis to reach adequate stem-cell collection. The median number of CD34-positive cells obtained in the VRD group was also found to be inferior in comparison with the VTD group. Importantly, stem-cell mobilization failure was more frequent in patients who received VRD induction. The triplet bortezomib, cyclophosphamide and dexamethasone (VCD) is considered as a standard of care prior ASCT [6]. Recently, Skerget and colleagues demonstrated similar stem-cell collection following VCD or VTD induction, in terms of CD34-positive cell yields and rate of mobilization failure [16]. Stem-cell collection impairment following lenalidomide-based induction has been previously reported [17,18,19]. In addition with its myelotoxicity, lenalidomide exposure has been associated with suppression of myeloid progenitors in collected graft [20]. The triplet combination carfilzomib–lenalidomide–dexamethasone (KRD) demonstrated strong efficacy as induction therapy prior ASCT [21]. Interestingly, Bal and colleagues recently showed that KRD induction resulted in a higher rate of collection failure and lower rate of stem-cell yields in comparison with VRD [22]. Recently, the anti-CD38 monoclonal antibody daratumumab has been approved in combination with VTD in newly diagnosed myeloma patients who are eligible for ASCT, based on the results of the phase-3 trial Cassiopeia [23]. In a phase-2 randomized study, the addition of daratumumab to VRD induction has been shown to significantly improve response rate [24]. However, the addition of daratumumab to VRD also resulted in lower rate of CD34-positive cells collection [24]. The phase-3 randomized trial EMN-02 recently demonstrated a progression-free and overall survival benefit favoring tandem ASCT versus single ASCT, especially for patients with high-risk cytogenetic [25]. This survival advantage following a tandem-transplant approach for selected MM patients reinforces the need of an optimal stem-cell collection. In the future context of lenalidomide and/or anti-CD38-based induction, attention should be paid to the optimal timing of stem-cell collection. Indeed, stem-cell harvesting should ideally be planned after 3– 4 cycles of induction, as suggested by the recent data issued from the German CONCEPT trial (NCT03104842) [26]. Moreover, mobilization with cyclophosphamide + G-CSF should be systematically considered [27].
To conclude, this real-life study confirms the possibility to obtain adequate autologous stem-cell collection for the vast majority of MM patients after VRD induction, even if more patients experienced collection failure in comparison with VTD. Moreover, VRD induction required a more frequent use of plerixafor and a higher number of apheresis, implying time, and cost-consuming consequences. The use of tandem transplantation for selected patients and the increasing addition of anti-CD38 monoclonal antibody during induction highlight the need of an optimal stem-cell collection strategy.
References
Attal M, Lauwers-Cances V, Hulin C, Leleu X, Caillot D, Escoffre M, et al. Lenalidomide, bortezomib, and dexamethasone with transplantation for myeloma. N Engl J Med. 2017;376:1311–20.
Moreau P, Touzeau C, Vij R, Goldsmith SR, Rosko AE. Newly diagnosed myeloma in 2020. Am Soc Clin Oncol Educ Book. 2020;40:1–15.
Rosiñol L, Oriol A, Teruel AI, Hernández D, López-Jiménez J, de la Rubia J, et al. Superiority of bortezomib, thalidomide, and dexamethasone (VTD) as induction pretransplantation therapy in multiple myeloma: a randomized phase 3 PETHEMA/GEM study. Blood. 2012;120:1589–96.
Moreau P, Hulin C, Macro M, Caillot D, Chaleteix C, Roussel M, et al. VTD is superior to VCD prior to intensive therapy in multiple myeloma: results of the prospective IFM2013-04 trial. Blood. 2016;127:2569–74.
Rosiñol L, Oriol A, Rios R, Sureda A, Blanchard M-J, Hernández MT, et al. Bortezomib, lenalidomide, and dexamethasone as induction therapy prior to autologous transplantation in multiple myeloma. Blood. 2019. https://doi.org/10.1182/blood.2019000241.
Moreau P, San Miguel J, Sonneveld P, Mateos MV, Zamagni E, Avet-Loiseau H, et al. Multiple myeloma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28:iv52–61.
Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, Mateos M-V, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15:e538–548.
Weaver CH, Hazelton B, Birch R, Palmer P, Allen C, Schwartzberg L, et al. An analysis of engraftment kinetics as a function of the CD34 content of peripheral blood progenitor cell collections in 692 patients after the administration of myeloablative chemotherapy. Blood. 1995;86:3961–9.
Gertz MA, Kumar SK, Lacy MQ, Dispenzieri A, Hayman SR, Buadi FK, et al. Comparison of high-dose CY and growth factor with growth factor alone for mobilization of stem cells for transplantation in patients with multiple myeloma. Bone Marrow Transplant. 2009;43:619–25.
Giralt S, Stadtmauer EA, Harousseau JL, Palumbo A, Bensinger W, Comenzo RL, et al. International myeloma working group (IMWG) consensus statement and guidelines regarding the current status of stem cell collection and high-dose therapy for multiple myeloma and the role of plerixafor (AMD 3100). Leukemia. 2009;23:1904–12.
DiPersio JF, Stadtmauer EA, Nademanee A, Micallef INM, Stiff PJ, Kaufman JL, et al. Plerixafor and G-CSF versus placebo and G-CSF to mobilize hematopoietic stem cells for autologous stem cell transplantation in patients with multiple myeloma. Blood. 2009;113:5720–6.
Chaudhary L, Awan F, Cumpston A, Leadmon S, Watkins K, Tse W, et al. Peripheral blood stem cell mobilization in multiple myeloma patients treat in the novel therapy-era with plerixafor and G-CSF has superior efficacy but significantly higher costs compared to mobilization with low-dose cyclophosphamide and G-CSF. J Clin Apher. 2013;28:359–67.
Sánchez-Ortega I, Querol S, Encuentra M, Ortega S, Serra A, Sanchez-Villegas JM, et al. Plerixafor in patients with lymphoma and multiple myeloma: effectiveness in cases with very low circulating CD34+ cell levels and preemptive intervention vs remobilization. Bone Marrow Transplant. 2015;50:34–39.
Van de Wyngaert Z, Nerich V, Fouquet G, Chrétien M-L, Caillot D, Azar N, et al. Cost and efficacy of peripheral stem cell mobilization strategies in multiple myeloma. Bone Marrow Transplant. 2020. https://doi.org/10.1038/s41409-020-0940-3.
Laszlo D, Marcacci GP, Martino M, Radice D, Rabascio C, Lucchetti B, et al. A comparison of chemo-free strategy with G-CSF plus plerixafor on demand versus intermediate-dose cyclophosphamide and G-CSF as PBSC mobilization in newly diagnosed multiple myeloma patients: an Italian explorative cost analysis. Transfus Apher Sci. 2020:102819. https://doi.org/10.1016/j.transci.2020.102819.
Skerget M, Skopec B, Sever M. VTD in comparison with VCD does not affect stem cell yields with G-CSF only mobilization. Acta Haematologica Polonica. 2020;51:42–46.
Kumar S, Dispenzieri A, Lacy MQ, Hayman SR, Buadi FK, Gastineau DA, et al. Impact of lenalidomide therapy on stem cell mobilization and engraftment post-peripheral blood stem cell transplantation in patients with newly diagnosed myeloma. Leukemia. 2007;21:2035–42.
Paripati H, Stewart AK, Cabou S, Dueck A, Zepeda VJ, Pirooz N, et al. Compromised stem cell mobilization following induction therapy with lenalidomide in myeloma. Leukemia. 2008;22:1282–4.
Popat U, Saliba R, Thandi R, Hosing C, Qazilbash M, Anderlini P, et al. Impairment of filgrastim-induced stem cell mobilization after prior lenalidomide in patients with multiple myeloma. Biol Blood Marrow Transplant. 2009;15:718–23.
Dosani T, Covut F, Pinto R, Kim B-G, Ali N, Beck R, et al. Impact of lenalidomide on collected hematopoietic myeloid and erythroid progenitors: peripheral stem cell collection may not be affected. Leuk Lymphoma. 2019;60:2199–206.
Kazandjian D, Korde N, Mailankody S, Hill E, Figg WD, Roschewski M, et al. Remission and progression-free survival in patients with newly diagnosed multiple myeloma treated with carfilzomib, lenalidomide, and dexamethasone: five-year follow-up of a Phase 2 Clinical Trial. JAMA Oncol. 2018;4:1781–3.
Bal S, Landau HJ, Shah GL, Scordo M, Dahi P, Lahoud OB, et al. Stem cell mobilization and autograft minimal residual disease negativity 1 with novel induction regimens in multiple myeloma. Biol Blood Marrow Transplant. 2020. https://doi.org/10.1016/j.bbmt.2020.04.011.
Moreau P, Attal M, Hulin C, Arnulf B, Belhadj K, Benboubker L, et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab before and after autologous stem-cell transplantation for newly diagnosed multiple myeloma (CASSIOPEIA): a randomised, open-label, phase 3 study. Lancet. 2019;394:29–38.
Voorhees PM, Kaufman JL, Laubach JP, Sborov DW, Reeves B, Rodriguez C, et al. Daratumumab, lenalidomide, bortezomib, & dexamethasone for transplant-eligible newly diagnosed multiple myeloma: GRIFFIN. Blood. https://doi.org/10.1182/blood.2020005288.
Cavo M, Gay F, Beksac M, Pantani L, Petrucci MT, Dimopoulos MA, et al. Autologous haematopoietic stem-cell transplantation versus bortezomib–melphalan–prednisone, with or without bortezomib–lenalidomide–dexamethasone consolidation therapy, and lenalidomide maintenance for newly diagnosed multiple myeloma (EMN02/HO95): a multicentre, randomised, open-label, phase 3 study. Lancet Haematol. 2020. https://doi.org/10.1016/S2352-3026(20)30099-5.
Weisel K, Asemissen AM, Besemer B, Haenel M, Blau IW, Goerner M. et al. Depth of response to isatuximab, carfilzomib, lenalidomide, and dexamethasone (Isa-KRd) in front-line treatment of high-risk multiple myeloma: Interim analysis of the GMMG-CONCEPT trial. JCO. 2020;38:8508.
Nazha A, Cook R, Vogl DT, Mangan PA, Gardler M, Hummel K, et al. Stem cell collection in patients with multiple myeloma: impact of induction therapy and mobilization regimen. Bone Marrow Transplant. 2011;46:59–63.
Acknowledgements
CT, PM, and SLG, are members of Site de Recherche Intégrée sur le Cancer (SIRIC) ILIAD, (INCA-DGOS-Inserm_12558).
Author information
Authors and Affiliations
Contributions
VL, CF, and CT, designed the study. VL, CF, CA, and CT, collected data. BT, performed statistical analysis. PD, performed stem-cell harvesting. CT, and VL, wrote the manuscript. All authors treated patients and critically reviewed the manuscript, and gave final approval.
Corresponding author
Ethics declarations
Conflict of interest
CT and PM are advisory board member and received honoraria from Sanofi.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Laurent, V., Fronteau, C., Antier, C. et al. Autologous stem-cell collection following VTD or VRD induction therapy in multiple myeloma: a single-center experience. Bone Marrow Transplant 56, 395–399 (2021). https://doi.org/10.1038/s41409-020-01033-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41409-020-01033-8
This article is cited by
-
Effect of prior lenalidomide or daratumumab exposure on hematopoietic stem cell collection and reconstitution in multiple myeloma
Annals of Hematology (2024)
-
Stem cell collection after lenalidomide, bortezomib and dexamethasone plus elotuzumab or isatuximab in newly diagnosed multiple myeloma patients: a single centre experience from the GMMG-HD6 and -HD7 trials
BMC Cancer (2023)
