
Abstract
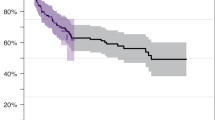
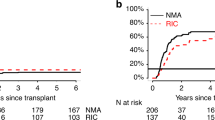
The optimal conditioning for patients with higher risk MDS receiving potentially curative allogeneic haematopoietic stem cell transplant(allo-HCT) remains to be defined. This is particularly the case for patients with excess of blasts at time of allo-HCT. Sequential (Seq) conditioning, whereby chemotherapy is followed rapidly by transplant conditioning, offers an opportunity to decrease disease burden, potentially improving outcomes allo-HCT outcomes. Herein we present the only analysis comparing Seq to myeloablative (MAC) and reduced intensity conditioning (RIC) specifically focussed on MDS patients with excess of blasts at allo-HCT. 303 patients were identified in the EBMT registry, receiving RIC (n = 158), Seq (n = 105), and MAC (n = 40). Median follow-up was 67.2 months and median age at allo-HCT was 59.5 years (IQR 53.5–65.6). For the entire cohort, 3 y overall survival (OS) was 50% (95% CI 45–56%) and relapse free survival (RFS) 45% (95% CI 40–51%). No significant differences in OS (log-rank p = 0.13) and RFS (log-rank p = 0.18) were observed between conditioning protocols. On multivariable analysis, lower performance status, worse IPSS-R cytogenetics, sibling donor (compared to 8/8 MUD) and ≥20% blasts at allo-HCT were associated with worse outcomes. In conclusion, the Seq protocol did little to influence the outcome in this high-risk group of patients, with outcomes mostly determined by baseline disease risk and patient characteristics such as performance status.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others
Data availability
The final analysis dataset will be available upon specific request to the working party chair.
References
Garcia‐Manero G, Chien KS, Montalban‐Bravo G. Myelodysplastic syndromes: 2021 update on diagnosis, risk stratification and management. Am J Hematol. 2020;95:1399–420.
Kröger N. Induction, bridging, or straight ahead: the ongoing dilemma of allografting in advanced myelodysplastic syndrome. Biol Blood Marrow Transpl. 2019;25:e247–9.
Saure C, Schroeder T, Zohren F, Groten A, Bruns I, Czibere A, et al. Upfront allogeneic blood stem cell transplantation for patients with high-risk myelodysplastic syndrome or secondary acute myeloid leukemia using a FLAMSA-based high-dose sequential conditioning regimen. Biol Blood Marrow Transpl. 2012;18:466–72.
Schmid C, Schleuning M, Ledderose G, Tischer J, Kolb H-J. Sequential regimen of chemotherapy, reduced-intensity conditioning for allogeneic stem-cell transplantation, and prophylactic donor lymphocyte transfusion in high-risk acute myeloid leukemia and myelodysplastic syndrome. J Clin Oncol. 2005;23:5675–87.
Greenberg P, Cox C, LeBeau MM, Fenaux P, Morel P, Sanz G, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood. 1997;89:2079–88.
Arber DA, Orazi A, Hasserjian R, Borowitz MJ, Beau MM, Bloomfield CD, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127:2391–406.
Greenberg PL, Tuechler H, Schanz J, Sanz G, Garcia-Manero G, Solé F, et al. Revised international prognostic scoring system for myelodysplastic syndromes. Blood. 2012;120:2454–65.
Bacigalupo A, Ballen K, Rizzo D, Giralt S, Lazarus H, Ho V, et al. Defining the intensity of conditioning regimens: working definitions. Biol Blood Marrow Transpl J Am Soc Blood Marrow Transpl. 2009;15:1628–33.
Schemper M, Smith TL. A note on quantifying follow-up in studies of failure time. Control Clin Trials. 1996;17:343–6.
Scott BL, Pasquini MC, Logan BR, Wu J, Devine SM, Porter DL, et al. Myeloablative versus reduced-intensity hematopoietic cell transplantation for acute myeloid leukemia and myelodysplastic syndromes. J Clin Oncol. 2017;35:1154–61.
Kröger N, Iacobelli S, Franke G-N, Platzbecker U, Uddin R, Hübel K, et al. Dose-reduced versus standard conditioning followed by allogeneic stem-cell transplantation for patients with myelodysplastic syndrome: a prospective randomized Phase III study of the EBMT (RICMAC Trial). J Clin Oncol. 2017;35:2157–64.
Craddock C, Jackson A, Loke J, Siddique S, Hodgkinson A, Mason J, et al. Augmented reduced-intensity regimen does not improve postallogeneic transplant outcomes in acute myeloid leukemia. J Clin Oncol. 2021;39:768–78.
Hourigan CS, Dillon LW, Gui G, Logan BR, Fei M, Ghannam J, et al. Impact of conditioning intensity of allogeneic transplantation for acute myeloid leukemia with genomic evidence of residual disease. J Clin Oncol. 2020;38:1273–83.
Christopeit M, Badbaran A, Alawi M, Zabelina T, Zeck G, Wolschke C, et al. Correlation of somatic mutations with outcome after FLAMSA-busulfan sequential conditioning and allogeneic stem cell transplantation in patients with myelodysplastic syndromes. Eur J Haematol. 2016;97:288–96.
Ciurea SO, Chilkulwar A, Saliba RM, Chen J, Rondon G, Patel KP, et al. Prognostic factors influencing survival after allogeneic transplantation for AML/MDS patients with TP53 mutations. Blood. 2018;131:2989–92.
Lindsley RC, Saber W, Mar BG, Redd R, Wang T, Haagenson MD, et al. Prognostic mutations in myelodysplastic syndrome after stem-cell transplantation. N. Engl J Med. 2017;376:536–47.
Forcade E, Chevret S, Finke J, Ehninger G, Beelen D, et al. Impact of in vivo T-cell depletion in patients with myelodysplastic syndromes undergoing allogeneic hematopoietic stem cell transplant: a registry study from the Chronic Malignancies Working Party of the EBMT. Bone Marrow Transpl. 2022;57:768–74.
Author information
Authors and Affiliations
Contributions
VP conceived and designed the study proposal, acquired data, interpreted results, drafted and revised manuscript, and approved final version. MR, DM, IYA conceived and designed the study proposal, interpreted results, revised manuscript, and approved final version. LG, LK, LdW acquired data, completed statistical analysis, interpreted results and approved final version. NK, KS, AG, JF, HLW, RPdL, YK, US, LSF, PJ, TS, JT, MA, MPC, PH, KR, JDS, CS acquired data, interpreted results and approved final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Potter, V., Gras, L., Koster, L. et al. Sequential vs myeloablative vs reduced intensity conditioning for patients with myelodysplastic syndromes with an excess of blasts at time of allogeneic haematopoietic cell transplantation: a retrospective study by the chronic malignancies working party of the EBMT. Bone Marrow Transplant 59, 224–231 (2024). https://doi.org/10.1038/s41409-023-02111-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41409-023-02111-3
