
Abstract
The β-lactams are the most widely used class of antibiotics due to their safety, effectiveness, and spectrum of activity. As a result of their ubiquitous usage, there has been a steady rise in β-lactam resistant Gram-negative bacteria, especially Pseudomonas aeruginosa, resulting in limited treatment options. P. aeruginosa can develop multidrug-resistant phenotypes using a multifaceted approach of β-lactamase expression, decreased porin production and increased efflux. Current β-lactamase inhibitors address drug hydrolyzing enzymes but may not be as effective in phenotypes with reduced permeability and/or overexpressed efflux pumps. Herein, we present the synthesis and biological evaluation of a nebramine-cyclam conjugate molecule that is able to potentiate β-lactam antibiotics, as well as other legacy antibiotics, against P. aeruginosa in vitro. Combination studies show that this adjuvant is able to synergize with β-lactams such as aztreonam and ceftazidime against multidrug-resistant and extremely drug-resistant clinical isolates through a hypothesized mechanism of outer membrane permeabilization. Importantly, the addition of low concentrations (8 µM) of the nontoxic nebramine-cyclam conjugate is able to further potentiate existing β-lactam/β-lactamase inhibitor combinations in β-lactamase-harboring P. aeruginosa strains. These data support a potential application of the nebramine-cyclam conjugate as an adjuvant for treating infections caused by P. aeruginosa strains that utilize multiple mechanisms of resistance.
Similar content being viewed by others


Introduction
Resistance to antibiotics has been rising among clinically relevant pathogens at an alarming rate and now poses a serious threat to public health. In particular, Gram-negative bacteria with low outer membrane (OM) permeability are often difficult to eradicate and are only treatable with small and hydrophilic antibiotics from certain drug classes [1, 2]. Acquired modifications to lipopolysaccharide of the OM has frequently been implicated in reduced antibacterial activity of antibiotics [3]. One such highly resistant organism is Pseudomonas aeruginosa, and clinical isolates resistant to all antibiotics have been observed [4]. Discovering new antibiotics or repurposing existing ones is therefore not only beneficial but may be necessary because these levels of resistance threaten modern medicine. Commonplace procedures (such as tooth extraction) to sophisticated medical interventions (such as organ transplant) all rely on the protection provided by antibiotics. Compounding this problem is the fact that no new antibiotic class has been discovered in the last few decades [5], and many new drugs are only active on Gram-positive bacteria [6]. New antibacterial chemotherapies are therefore desperately needed to address these issues.
β-Lactam antibiotics, which inhibit peptidoglycan synthesis by binding to penicillin binding proteins (transpeptidases), are the most widely prescribed antibiotic class globally [7,8,9]. The carbapenems are often used as drugs of last resort and therefore resistance to these β-lactams can culminate in infections with limited or no treatment options [9]. Resistance to β-lactam antibiotics is multifaceted but is often attributed to overproduction of β-lactamase enzymes (which hydrolyze the β-lactam ring) and efficient downregulation of porin proteins [10]. β-lactamase inhibitors have been developed as antibiotic adjuvants (compounds that are able to increase the activity of an existing antibiotic or rescue them from resistance [11]) to counteract β-lactamase mediated resistance. However, to the best of our knowledge, there is currently no approved combination therapy that holistically addresses the problem of reduced influx which affects not just β-lactam antibiotics but also β-lactamase inhibitors. Facilitating the diffusion of antibiotics through the OM is one of the most promising recent approaches to address OM impermeability. Polymyxins, surfactants, and antimicrobial peptides have been investigated for this role but there has been limited results showing strong efficacy with β-lactams [12]. Similar approaches using adjuvants have been explored previously with tobramycin-based conjugates [3]. These compounds are able to permeabilize the OM, increasing the net influx of antibiotics and rescuing many classes of antibiotics from resistance [13, 14]. Nevertheless, only a few of these compounds could potentiate select β-lactam antibiotics [3].
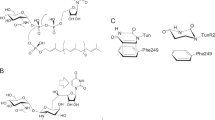
To address the problem of β-lactam penetrance across the OM due to porin loss, we have recently identified a tobramycin-cyclam scaffold that restores β-lactam (including carbapenems) activity against recalcitrant P. aeruginosa phenotypes [15]. The aim of this study was therefore to optimize this molecule by synthesizing a lower molecular weight nebramine-based conjugate, nebramine-cyclam (1) (Fig. 1) and investigate its adjuvant properties in combination with β-lactam antibiotics against clinical isolates. We hypothesized that an amphiphilic nebramine, an amphiphilic tobramycin derivative lacking one D-glucose sugar, may retain the OM destabilizing properties of amphiphilic tobramycin but with improved toxicity profile (due to reduction in cationicity [16]). Conjugation to cyclam (a nontoxic divalent metal chelator [17]) may augment this property by sequestering the divalent cations that are necessary to stabilize the OM of Gram-negative bacteria. Cyclam may also exhibit the additional effect of chelating divalent cations responsible for downregulation of porin proteins in P. aeruginosa [18]. An aliphatic tether length of eight carbons was chosen to link the nebramine and cyclam moieties in an attempt to retain membrane activity without imparting nonspecific toxicity [14, 19]. Moreover, previous studies showed that a tobramycin-cyclam conjugate with an 8-carbon tether had the most promising activity of the prepared series [15]. To investigate the exact role of nebramine, we prepared a ciprofloxacin-cyclam analog (2) (Fig. 1) for comparative studies with 1. Herein, we report that nebramine-cyclam conjugate 1, but not ciprofloxacin-cyclam conjugate 2, potentiates the activity of ceftazidime and aztreonam against multidrug-resistant P. aeruginosa clinical isolates.

Structure of tobramycin-cyclam and the newly synthesized nebramine-cyclam (1) and ciprofloxacin-cyclam (2) conjugates
Materials and methods
Chemistry
All chemicals used for synthesis were purchased from Sigma-Aldrich (Oakville, Canada) and used as is, except tobramycin which was purchased from AK Scientific, Inc. (Union City, USA). Intermediate compounds were purified using flash column chromatography packed with silica gel 60 (230–400 mesh) and eluted with the solvents indicated. The final compounds were purified using reverse-phase column chromatography packed with C18 silica gel. Compounds were characterized using 1D and 2D nuclear magnetic resonance experiments (1H, 13C, COSY, DEPT-135, HSQC, and HMBC) performed on either Bruker AMX-300 or AMX-500 spectrometers in deuterated solvents. Relative chemical shift (δ) is expressed as parts per million (ppm) relative to respective solvents. Multiplicities are reported as s, singlet; d, doublet; t, triplet; q, quartet; dt, doublet of triplets, coupling constants (J) are reported in Hertz (Hz) and integrations represent number of protons. Mass spectrometry (MS) was carried out by either electrospray ionization (ESI) on a Varian 500-MS ion trap mass spectrometer or matrix-assisted laser desorption ionization (MALDI) MS on a Bruker Daltonics Ultraflex MALDI TOF/TOF mass spectrometer. Full synthetic procedures for Schemes 1 and 2 and compound characterizations are presented in the Supplementary information.

Synthesis of nebramine-cyclam (1). (i) Boc2O, Et3N, MeOH/H2O (2:1), 55 °C, (98%). (ii) TBDMSCl, N-methyl imidazole, DMF, rt, (67%). (iii) 1,8-dibromooctane, TBAHS, KOH, toluene, rt, (51%). (iv) Cs2CO3, DMF/H2O (10:1), 70 °C, (30%). (v) PCC, NaOAc, DCM, rt, (94%). (vi) Boc2O, DCM, rt, (92%). (vii) AcOH, Na(OAc)3BH, DCE, 0 °C to rt, (52%). (viii) MeOH:HCl (4:3), 70 °C. (ix) Boc2O, Et3N, MeOH:H2O (2:1), 55 °C, (71%). (x) DCM/TFA (1:1), rt, subsequent conversion to HCl salt (86%)

Synthesis of ciprofloxacin-cyclam (2). (i) AcOH, Na(OAc)3BH, DCE, 0 °C to rt, (67%). (ii) p-TsOH, MeOH, 100 °C, (87%). (iii) AcOH, Na(OAc)3BH, DCE, 0 °C to rt, (78%). (iv) 2 N LiOH, MeOH, THF, rt, (50%). (v) DCM/TFA (1:1), rt, subsequent conversion to HCl salt (32%)
Microbiology
Bacterial strains and cultivation
Bacterial isolates were either isolated from clinically relevant and drug-resistant infections through the Canadian National Intensive Care Unit (CAN-ICU) study [20] and the Canadian Ward Surveillance (CANWARD) study [21, 22], or were strains from the American Type Culture Collection (ATCC). Drug-resistant P. aeruginosa isolates are characterized, where appropriate, as either multidrug-resistant (MDR; nonsusceptibility to at least one agent in three or more antimicrobial categories), extremely drug-resistant (XDR; nonsusceptibility to at least one agent in all but two or fewer antimicrobial categories) or pan drug-resistant (PDR; nonsusceptibility to all agents in all antimicrobial categories) [23]. Where applicable, visual reading of microbial growth was verified by measuring optical density (OD) at a wavelength of 595 nm on an EMax Plus microplate reader (Molecular Devices, San Jose, USA).
Antimicrobial sensitivity testing
The in vitro standalone antimicrobial activity of all compounds was determined using the broth microdilution method as described by Clinical and Laboratory Standards Institute (CLSI) guidelines [24].
Combination studies
Combination studies were performed using a checkerboard assay method as previously described [14, 25]. Interactions between compounds was determined from checkerboard plates by calculating the fractional inhibitory concentration (FIC) index, an established measure of synergy [26]. The FIC for each compound was calculated as FICantibiotic = MICantibiotic in combination/MICantibiotic alone and FICadjuvant = MICadjuvant in combination/MICadjuvant alone. FIC index = FICantibiotic + FICadjuvant and FIC index ≤0.5 is synergistic, FIC index > 0.5 but ≤ 4.0 is additive and FIC index > 4.0 is antagonistic. Triple combination studies were performed using standard checkerboard assays, as previously described [15], with the addition of a constant concentration of β-lactamase inhibitor as indicated.
Mammalian cell cytotoxicity
Cytotoxicity of conjugates 1 and 2 against human embryonic kidney (HEK293) cells and liver hepatocellular carcinoma (HepG2) cells was conducted and interpreted as previously described [19, 27]. Doxorubicin, an anticancer agent, served as the positive control.
Hemolysis assay
Quantification of eukaryotic erythrocyte hemolysis was performed by measuring the amount of hemoglobin released from porcine erythrocytes, as earlier described [13, 14]. Percent hemolysis was calculated for various concentrations of conjugate 1, relative to the positive control 0.1% Triton X-100 (set as 100%), as % hemolysis = (OD570 of sample − negative control)/(positive control − negative control).
Results
Chemistry
Chemical synthesis of nebramine-cyclam (1) was accomplished via a ten-step reaction pathway (Scheme 1). Conjugation at the C-5 position of tobramycin was carried out because modification at this position has been shown to afford molecules that retain membrane destabilizing effect but with no intrinsic ribosomal binding ability [3, 13], and the same effect was hypothesized for nebramine. Regioselective protection of tobramycin with a bulky di-tert-butyl dicarbonate and TBDMSCl yielded 3 with a free alcohol at the C-5 position. This position was alkylated with an 8-carbon aliphatic tether to give 4. Hydrolysis of the bromine to an alcohol under hydrous conditions yielded 5 and subsequent oxidation with PCC afforded aldehyde 7. Cyclam was tri-Boc-protected with di-tert-butyl dicarbonate forming 6 and reductive amination was used to ligate 6 to 7 yielding 8 which contains a tertiary amine bond, thus retaining the chelating capacity of cyclam. Regioselective cleavage of the α-D-glucopyranosyl bond [28] of 8 was achieved under strong acidic conditions (3:4 ratio of concentrated HCl:methanol) at 70 °C. The resulting compound was re-protected with di-tert-butyl dicarbonate giving 9, which was purified on flash chromatography, and finally deprotected with TFA to afford the desired compound as a TFA salt. This was then converted to final compound conjugate 1 as an HCl salt (used for biological testing) by treating the TFA compound with a stoichiometric amount of HCl.
Ciprofloxacin-cyclam (2) was synthesized as shown in Scheme 2. Protection of the carboxylic acid of ciprofloxacin was accomplished using MeOH in acidic conditions forming methyl-ester 11. Reductive amination of protected cyclam (6) and glutaraldehyde formed 10, which was purified and subjected to another reductive amination reaction with 11 to yield the protected ciprofloxacin-cyclam conjugate (12). Global deprotection of the methyl ester and Boc protecting groups using LiOH and TFA, respectively, yielded final conjugate 2 as a TFA salt which was then converted to HCl for biological testing.
Mammalian cell cytotoxicity and hemolysis
The toxicity of conjugate 1 was assessed in order to evaluate its potential for application as a drug. The viability of both HepG2 and HEK293 cells was maintained above 95% at a high concentration of 50 μM (~45 µg ml−1), a threefold higher concentration than the highest working concentrations (Fig. S1A). Cell viability remained >95% at the maximum concentration tested (100 µM; data not shown). In contrast, the well-known anticancer agent doxorubicin reduced cell viability to 12% and 7% at a concentration of 12.5 μM in HepG2 and HEK293 cells respectively (Fig. S1A). Hemolysis in porcine erythrocytes was also maintained at safe levels of <1% relative to Triton X-100 surfactant at concentrations up to 1024 µg ml−1 (Fig. S1B).
Antibacterial activity of nebramine-cyclam (1) and ciprofloxacin-cyclam (2) as stand-alone drugs
The MIC of conjugate 1 and 2 was tested in a panel of Gram-negative and Gram-positive bacteria and, as expected, 1 had minimal intrinsic activity (MIC ≥ 256 µg ml−1; Table S1). Considering that the molecular design of conjugate 1 was targeted at P. aeruginosa, the MIC was also tested against a wide range of drug-resistant P. aeruginosa clinical isolates. Again, the MIC was very high (≥256 µg ml−1 for all isolates). Conjugate 2 had an MIC of 32 µg ml−1 in PAO1 and MICs of 4 µg ml−1 and 1 µg ml−1 in efflux deficient mutants PAO200 and PAO750 respectively (Table S1). The MIC of 2 was also tested in other Gram-negative and Gram-positive organisms but the molecule displayed minimal activity (Table S1).
Combination studies of nebramine-cyclam (1) and ciprofloxacin-cyclam (2) with antibiotics against wild-type P. aeruginosa
Having designed conjugate 1 as an adjuvant, its ability to act synergistically with existing antibiotics was explored. The compound was tested in combination with 20 different antibiotics (which covered all major antibiotic classes) against wild type P. aeruginosa strain PAO1 (Table 1 and Fig. S2). A combination concentration cut-off of 16 µg ml−1 (~18 µM) was used for conjugate 1 in order to remain within achievable aminoglycoside plasma concentrations (~200 µM) [29]. Synergistic interactions were seen in 9 out of the 20 tested antibiotics showing that 1 exhibited adjuvant properties (Table 1). The strongest potentiation was seen with aztreonam and doxycycline (FIC index = 0.13), reducing MICs from 8 µg ml−1 to 1 µg ml−1 and 16 µg ml−1 to 2 µg ml−1 respectively (Fig. S2 and Table 1) when used in combination with 16 µg ml−1 of conjugate 1. β-lactams other than aztreonam (e.g., ceftazidime and piperacillin) were also synergistic with 1 (Fig. S2). Outer membrane impermeable antibiotics such as rifampicin and novobiocin were potentiated by conjugate 1 with FIC indexes of ~0.25 for both. A dose dependent effect was seen, with increasing concentrations of conjugate 1 leading to higher levels of potentiation up to the maximum tested concentration of 16 µg ml−1. Aztreonam and doxycycline were selected for further studies due to their high level of potentiation while ceftazidime was further investigated due to its clinical importance [7, 8]. To investigate the role of the nebramine moiety, conjugate 2 (nebramine replaced with ciprofloxacin) was tested in combination with select antibiotics against PAO1 but none were seen to be synergistic (Table S2). FIC indices of >0.5 were seen for all tested antibiotics, including aztreonam, doxycycline, rifampicin and novobiocin, all of which were potentiated by 1. It is interesting to note that the parent molecule tobramycin and cyclam did not show any synergy with aztreonam, ceftazidime and doxycycline against PAO1 [15], suggesting that the molecular fusion of both domains is critical for their adjuvant properties.
Combination studies of nebramine-cyclam (1) against other Gram-negative and Gram-positive isolates
The synergy seen between 1 and aztreonam, ceftazidime and doxycycline in PAO1 led us to wonder if the same activity could be seen in other species of bacteria. Conjugate 1 was tested in combination with aztreonam, ceftazidime and doxycycline against a panel of both Gram-positive and Gram-negative bacteria. The resulting FIC index values indicated that conjugate 1 was unable to potentiate most of these antibiotics in the strains tested (Table S3).
Potentiation of aztreonam, ceftazidime, and doxycycline in drug-resistant clinical isolates of P. aeruginosa
Having observed potentiation of a wide range of antibiotics in wild type P. aeruginosa strain PAO1, it was investigated whether the same affect would be seen in drug-resistant clinical isolates. Conjugate 1 was tested in combination with aztreonam, ceftazidime and doxycycline which were selected as the most promising from results in PAO1. All three combinations were tested against eight P. aeruginosa clinical isolates obtained from CAN-ICU and CANWARD studies [20, 22]. Intriguingly, much of the potentiation seen in PAO1 was retained in the resistant isolates (Fig. 2). A synergistic effect was seen between conjugate 1 (≤16 µg ml−1) and aztreonam, ceftazidime and doxycycline in four out of eight isolates, three out of eight isolates and six out of eight isolates, respectively (Fig. 2). FIC indexes for all synergistic combinations ranged from ≤0.19 to ≤0.31. An antagonistic effect (FIC index > 4, meaning decreased antibiotic activity) was not seen in any combination. Out of the six aztreonam resistant isolates (MIC ≥ 32 µg ml−1), four isolates were made intermediate or susceptible to aztreonam (MIC ≤ 16 µg ml−1) (Table S4). For ceftazidime, an intermediate resistant level (MIC = 16 µg ml−1) was attained in one of four ceftazidime-resistant (MIC ≥ 32 µg ml−1) isolates (Table S4). Doxycycline is not a typical antipseudomonal agent due to intrinsic resistance, hence the CLSI susceptibility breakpoint for Acinetobacter baumannii was used as interpretive standard [24]. This estimate indicated that in combination with conjugate 1, the MIC of doxycycline was brought to intermediate (MIC = 8 µg ml−1) or susceptible (MIC ≤ 4 µg ml−1) levels in four out of eight doxycycline resistant (MIC ≥ 16 µg ml−1) strains (Table S4). Again, a dose-dependent effect of conjugate 1 was seen with increased effect at higher concentrations up to the maximum reported concentration of 16 µg ml−1.

Synergistic effect of nebramine-cyclam (1) in combination with antibiotics against clinically relevant MDR and XDR P. aeruginosa isolates. FIC index values calculated for combinations with concentrations of conjugate 1 at ≤16 µg ml−1. ND = not determined
Potentiation of aztreonam, ceftazidime, and doxycycline in efflux deficient P. aeruginosa
To investigate whether conjugate 1 was interacting with efflux proteins to enhance susceptibility of P. aeruginosa to β-lactam antibiotics, synergistic interactions were assessed in two efflux-deficient P. aeruginosa strains: PAO200 (MexAB-OprM mutant) and PAO750 (knockout of MexAB-OprM, MexCD-OprJ, MexEF-OprN, MexJK, MexXY, and OmpH). Synergy between conjugate 1 and both β-lactam antibiotics was maintained in both efflux deficient strains (FIC indexes between 0.19 and 0.31), whereas potentiation was lost for doxycycline (Table 2). This result is consistent with previous studies that showed that potentiation of β-lactam antibiotics by tobramycin-based conjugates is efflux-independent [15] while potentiation of doxycycline is dependent on efflux pumps [30].
Triple combinations of nebramine-cyclam (1) with β-lactam antibiotics and a β-lactamase inhibitor
The ability of conjugate 1 to act synergistically with β-lactam antibiotics in clinical isolates led us to explore whether it was able to further potentate β-lactam/β-lactamase inhibitor combinations which are currently essential in clinics [7]. Five P. aeruginosa β-lactamase-producing clinical isolates, which were resistant to all β-lactam antibiotics, were used in this study (Table S5). Avibactam (AVI) was used as a β-lactamase inhibitor because of its clinical relevance [31] to inhibit class A, C and some class D β-lactamases in P. aeruginosa [32]. Checkerboard assays of double combinations (β-lactam antibiotic + AVI, β-lactam antibiotic+conjugate 1 and AVI + conjugate 1) were carried out as well as a triple combination (β-lactam antibiotic+ AVI + conjugate 1) for three β-lactam antibiotics including ceftazidime, aztreonam, and meropenem. All data for these combinations are reported at a concentration of 8 µM for both avibactam (AVI) (~2 µg ml−1) and conjugate 1 (~7 µg ml−1). As expected, a double combination of AVI+conjugate 1 did not show any meaningful activity in any of the five strains (data not shown). Double combinations of either ceftazidime, aztreonam, or meropenem along with conjugate 1 often show a modest level of potentiation. At most, conjugate 1 was able to reduce the MIC of the antibiotic by fourfold at the tested concentration of 8 µM (~7 µg ml−1) (Fig. 3). Once all three compounds were in combination however, very significant reductions in MIC was seen. In five out of five strains, the addition of conjugate 1 was able to further decrease the MIC of both ceftazidime and aztreonam past what was seen in the double combination of avibactam/β-lactam antibiotic (Fig. 3). For meropenem, the addition of conjugate 1 was able to further decrease the MIC over double combination therapy in four out of five strains (Fig. 3). The additional potentiation due to conjugate 1 varied from twofold to eightfold in all combinations where a further lowering of MIC was seen over double combination therapy. In all cases, the triple combinations of conjugate 1 and avibactam and either ceftazidime, aztreonam, or meropenem was able to reduce the MIC of the antibiotic by between 16–32-fold, 8–64-fold and 2–16-fold respectively, relative to the MIC of the antibiotic alone (Fig. 3).

Triple combinations of nebramine-cyclam (1), avibactam and various β-lactam antibiotics against β-lactam resistant, β-lactamase harboring P. aeruginosa strains. a Ceftazidime + avibactam + conjugate 1. b Aztreonam + avibactam + conjugate 1. c Meropenem + avibactam + conjugate 1. All MICs shown were determined at 8 µM (~7 µg ml−1) of conjugate 1 and 8 µM (~2 µg ml−1) avibactam where relevant. AVI = avibactam, CAZ = ceftazidime, AZT = aztreonam and MER = meropenem
Discussion
Antimicrobial resistance has become more prevalent and multifaceted in recent years and this has spurred the use of more complex therapies such as combinations of existing antibiotics. A true synergistic or beneficial effect between them however, is not often documented [33]. Currently, the only major use of these combinations is to cover a wider pathogen spectrum during empirical therapy [34]. In recent years the most promising approach has proven to be the use of adjuvant molecules which may not be intrinsically active on their own [11]. For example, the use of fixed-dose β-lactam/β-lactamase inhibitor combinations has become a common therapy [35]. Even still, the ability of β-lactamase inhibitors to rescue β-lactam antibiotics from resistance can fail in Gram-negative bacteria with decreased OM permeability through mechanisms such as downregulated porin (OprD or OprF in P. aeruginosa) expression or increased efflux [10].
Consequently, a nebramine-cyclam (1) molecule was developed (Scheme 1) to specifically target P. aeruginosa, a difficult-to-treat Gram-negative pathogen. Studies were carried out to determine the ability of conjugate 1 to potentiate existing antibiotics, particularly β-lactams, as well as assess its applicability to combination therapies. Through multiple combination studies conjugate 1 was identified to be an effective adjuvant when used with many antibiotics including efflux-prone doxycycline, but more importantly β-lactams such as aztreonam and ceftazidime in P. aeruginosa.
The effects of the conjugate 1 molecule were not likely due to intrinsic activity, because the MIC alone was very high (≥256 µg ml−1) in all tested species and strains of bacteria (Tables S1 and S4). This is consistent with previous reports that modifications of tobramycin at the C-5 position diminishes ribosomal binding activity [13]. Despite the inability to inhibit bacteria by binding the ribosome, multiple lines of evidence suggest that conjugate 1 is able to affect the OM of P. aeruginosa. Permeabilization of the OM would affect multiple classes of antibiotics and potentiation was indeed observed across a broad spectrum of antibiotics (Fig. S2). A general lack of potentiation in Gram-positive bacteria (Table S3), which do not have an OM permeability barrier, along with the observed potentiation of hydrophobic drugs that are normally impeded by the OM, such as rifampicin and novobiocin (Fig. S2), corroborate a hypothesis of outer membrane permeabilization. Numerous reports have shown a similar pattern in molecules that permeabilize the outer membrane such as polymyxins, surfactants and antimicrobial peptides [12]. It is however, interesting that the same level of potentiation seen in P. aeruginosa (Fig. S2) was not translated into most other Gram-negative bacteria (Table S3) all of which have an OM. This is likely due to the extreme impermeability caused by variation in lipid A of lipopolysaccharide and altered porin regulation in the P. aeruginosa membrane, leading to estimates of 1–8% of the relative permeability seen in Escherichia coli [2]. A. baumannii is also known for a lower vulnerability to β-lactams due to an impermeable OM [36,37,38] and was the only species other than P. aeruginosa in which synergy was seen between conjugate 1 and the tested antibiotics (Table S3). A similar trend has been seen with known cationic OM permeabilizers, such as polymyxins, where a greater synergistic effect was observed in P. aeruginosa as compared to E. coli [39].
As with any hybrid or conjugate molecule, there is always a question as to whether the direct connection of the individual moieties is truly necessary or if one of them individually is responsible for the activity. The activity of conjugate 1 however, was shown to be most likely unique to the molecule because neither cyclam nor the parent molecule tobramycin (used as a substitute for nebramine) are able to potentiate any of the tested antibiotics in PAO1 [15]. This suggests that molecular fusion of the two moieties is necessary for the synergistic effects seen with conjugate 1. These results also support the likelihood of an OM effect because if chelation or ribosomal activity alone was at play then potentiation would likely have been seen using cyclam or tobramycin respectively. Conjugate 2 which contained cyclam, but the nebramine portion was substituted by ciprofloxacin, also did not show any synergistic effect in any tested combinations (Table S2) indicating the importance and necessity of the cationic nebramine moiety for the activity of conjugate 1.
Efflux disruption was another potential target for the action of conjugate 1. Although PAO1 does express a basal level of efflux [40], solely inhibiting efflux was not suspected due to the broad range of potentiation including with OM impermeable antibiotics. In addition, many molecules which affect efflux exhibit lesser potentiation in efflux deficient strains [41]. In accordance with the idea that conjugate 1’s action was not limited to efflux inhibition, a synergistic relationship (FIC index < 0.5) was seen in both PAO1 (Table 1, Fig. S2) and the efflux deficient strains PAO200 and PAO750 (Table 2). From efflux studies it is also evident that efflux is not responsible for the low intrinsic activity (high MIC) of conjugate 1 because the molecule has a very high MIC in wild type PAO1, but also in efflux deficient PAO200 and PAO750 (Table S1). Conjugate 2 on the other hand was seen to be significantly affected by efflux. The MIC of 32 µg ml−1 in PAO1 was drastically reduced to 4 µg ml−1 and 1 µg ml−1 in PAO200 and PAO750 respectively (Table S1).
The potentiating effect of conjugate 1 seen in P. aeruginosa was very promising because of the general robust nature of this organism. Specifically, a triple combination of conjugate 1 with existing β-lactam/β-lactamase inhibitor showed promising results and was seen to be superior to the β-lactam/β-lactamase inhibitor mixture alone in 14 out of 15 combinations (Fig. 3). Since the discovery of penicillin, the β-lactam antibiotics including multiple generations of cephalosporins, monobactams and carbapenems have become cornerstone agents in antibiotic chemotherapy. This is majorly due to their efficacy and tolerability, however bacteria can and have developed multimodal resistance. The major mechanism is producing β-lactamase enzymes including classes A, C, and D serine β-lactamase enzymes as well class B metallo-β-lactamases that are able to hydrolyze and render β-lactams ineffective [42]. In addition, Gram-negative bacteria can modify the outer membrane or upregulate efflux [8, 9]. To counter the enzyme component, medicinal chemists have developed β-lactamase inhibitors such as avibactam (in combination with ceftazidime), tazobactam (with piperacillin or ceftolozane) and vaborbactam (with meropenem) [7, 35]. In these studies, avibactam was used as a β-lactamase inhibitor because of its clinical relevance [31] to inhibit class A, C, and some class D β-lactamases in P. aeruginosa [32]. To date, no commonly used combination has addressed both the enzymatic and permeability mechanisms of resistance to β-lactams together. Our studies however, show that an OM permeabilizer may be able to further augment β-lactam/β-lactamase combinations (Fig. 3), thereby increasing the effectiveness of these mainstay therapies. A triple combination of conjugate 1 (8 µM), avibactam (8 µM), and one of ceftazidime, aztreonam, or meropenem seems to be very effective because of its ability to address multimodal resistance through complementing drug activities. In general, resistance development to ceftazidime/avibactam combination in P. aeruginosa can be acquired by various mechanisms, including mutations in the active site of AmpC β-lactamases and penicillin binding proteins, expression of metallo-β-lactamases, suppression of porin expression, reduced outer membrane permeability, and overexpression or structural modification of efflux pumps [43, 44]. The same resistance development mechanisms, except for the expression of metallo-β-lactamases, can affect aztreonam/avibactam combinations [43, 44]. Based on our previous studies with related tobramycin-based conjugates, we anticipate that conjugate 1 may interfere with bacterial defense mechanisms related to OM impermeability, efflux, and/or porin suppression [3, 13, 15]. However, resistance development due to loss in β-lactamase inhibitory function of avibactam is not expected to be covered by adjuvant 1 and will be a potential pseudomonal resistance mechanism when exposed to the investigated triple component combination.
Multiple lines of evidence validate the potential application of a molecule with properties similar to conjugate 1. The compound has very low in vitro toxicity in mammalian cells and insignificant hemolysis of erythrocytes (Fig. S1). This suggests a mechanism of activity specific to bacterial membranes which is necessary for a candidate drug molecule. Combinations of aminoglycosides similar in structure to nebramine and β-lactams have also shown some synergy [45] however these combinations are dependent on the activity of both molecules and therefore are not as likely effective in highly resistant isolates. In addition, the reported slight OM destabilizing effect of aminoglycosides would not be sufficient in place of conjugate 1 because the concentration of tobramycin required to provide OM destabilization is much higher than safely achievable in the body [46]. Understandably, clinical use of these combinations is not normally aimed at highly resistant organisms and also often leads to limited advantage [47]. In contrast, the potentiation due to conjugate 1 in our triple combination therapy is relevant to clinical isolates showing high resistance to most β-lactams (Table S5, Fig. 3). Together, these data show that the conjugate 1 molecule may be a fitting combination with β-lactam/β-lactamase inhibitors.
In conclusion, the current study demonstrates that nebramine-cyclam conjugate 1 has compelling adjuvant properties when given in combination with existing antibiotics. Of major importance is its ability to potentiate β-lactams including ceftazidime and aztreonam in MDR and XDR P. aeruginosa. The addition of conjugate 1 to existing β-lactam/β-lactamase inhibitor combinations was shown to have a significant in vitro benefit in strains harboring β-lactamase enzymes and that were resistant to the tested β-lactam monotherapies. The hypothesized outer membrane disruption provided by conjugate 1 is important in suggesting a potential application against P. aeruginosa strains exhibiting multimodal resistance and where β-lactamase inhibitors are consequently losing effectiveness.
References
Fair RJ, Tor Y. Antibiotics and bacterial resistance in the 21st century. Perspect Med Chem. 2014;6:25–64.
Zgurskaya HI, Lopez CA, Gnanakaran S. Permeability barrier of gram-negative cell envelopes and approaches to bypass it. ACS Infect Dis. 2015;1:512–22.
Domalaon R, Idowu T, Zhanel GG, Schweizer F. Antibiotic hybrids: the next generation of agents and adjuvants against gram-negative pathogens? Clin Microbiol Rev. 2018;31:e00077–17.
Wang CY, et al. Pandrug-resistant Pseudomonas aeruginosa among hospitalised patients: clinical features, risk-factors and outcomes. Clin Microbiol Infect. 2006;12:63–8.
Brown ED, Wright GD. Antibacterial drug discovery in the resistance era. Nature . 2016;529:336–43.
Ling LL, et al. A new antibiotic kills pathogens without detectable resistance. Nature . 2015;517:455–9.
Bush K, Bradford PA. β-lactams and β-lactamase inhibitors: an overview. Cold Spring Harb Perspect Med. 2016;6:a025247.
Thakuria B, Lahon K. The beta lactam antibiotics as an empirical therapy in a developing country: an update on their current status and recommendations to counter the resistance against them. J Clin Diagn Res. 2013;7:1207–14.
Meletis G. Carbapenem resistance: overview of the problem and future perspectives. Ther Adv Infect Dis. 2016;3:15–21.
Fernández L, Hancock REW. Adaptive and mutational resistance: role of porins and efflux pumps in drug resistance. Clin Microbiol Rev. 2012;25:661–81.
Wright GD. Antibiotic adjuvants: rescuing antibiotics from resistance. Trends Microbiol. 2016;24:862–71.
Bolla J-M, et al. Strategies for bypassing the membrane barrier in multidrug resistant gram-negative bacteria. FEBS Lett. 2011;585:1682–90.
Gorityala BK, et al. Adjuvants based on hybrid antibiotics overcome resistance in pseudomonas aeruginosa and enhance fluoroquinolone efficacy. Angew Chem—Int Ed. 2016;55:555–9.
Lyu Y, et al. Amphiphilic tobramycin–lysine conjugates sensitize multidrug resistant gram-negative bacteria to rifampicin and minocycline. J Med Chem. 2017;60:3684–702.
Idowu T, Ammeter D, Arthur G, Zhanel GG, Schweizer F. Potentiation of β-lactam antibiotics and β-lactam/β-lactamase inhibitor combinations against multidrug and extensively drug-resistant pseudomonas aeruginosa using non-ribosomal tobramycin-cyclam conjugates. J Antimicrob Chemother. In press 2019; https://doi.org/10.1093/jac/dkz228.
Chiu PJ, Miller GH, Long JF, Waitz JA. Renal uptake and nephrotoxicity of gentamicin during urinary alkalinization in rats. Clin Exp Pharm Physiol. 1979;6:317–26.
Yu M, et al. Nontoxic metal–cyclam complexes, a new class of compounds with potency against drug-resistant Mycobacterium tuberculosis. J Med Chem. 2016;59:5917–21.
Perron K, et al. CzcR-CzcS, a two-component system involved in heavy metal and carbapenem resistance in Pseudomonas aeruginosa. J Biol Chem. 2004;279:8761–8.
Idowu T, Samadder P, Arthur G, Schweizer F. Amphiphilic modulation of glycosylated antitumor ether lipids results in a potent triamino scaffold against epithelial cancer cell lines and BT474 cancer stem cells. J Med Chem. 2017;60:9724–38.
Zhanel GG, et al. Antimicrobial-resistant pathogens in intensive care units in Canada: results of the Canadian National Intensive Care Unit (CAN-ICU) study, 2005-2006. Antimicrob Agents Chemother. 2008;52:1430–7.
Zhanel GG, et al. Prevalence of antimicrobial-resistant pathogens in Canadian hospitals: results of the Canadian Ward Surveillance Study (CANWARD 2008). Antimicrob Agents Chemother. 2010;54:4684–93.
Zhanel GG, et al. Antimicrobial susceptibility of 22746 pathogens from Canadian hospitals: results of the CANWARD 2007-11 study. J Antimicrob Chemother. 2013;68:i7–22.
Magiorakos AP, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18:268–81.
Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. In: CLSI Supplement M100. 27th Ed. Wayne, PA: Clinical and Laboratory Standards Institute; 2017.
Orhan G, Bayram A, Zer Y, Balci I. Synergy tests by e test and checkerboard methods of antimicrobial combinations against Brucella melitensis. J Clin Microbiol. 2005;43:140–3.
Meletiadis J, Pournaras S, Roilides E, Walsh TJ. Defining fractional inhibitory concentration index cutoffs for additive interactions based on self-drug additive combinations, monte carlo simulation analysis, and in vitro-in vivo correlation data for antifungal drug combinations against Aspergillus fumigatus. Antimicrob Agents Chemother. 2010;54:602–9.
Idowu T, Samadder P, Arthur G, Schweizer F. Design, synthesis and antitumor properties of glycosylated antitumor ether lipid (GAEL)-chlorambucil-hybrids. Chem Phys Lipids. 2016;194:139–48.
Berkov-Zrihen Y, et al. Tobramycin and nebramine as pseudo-oligosaccharide scaffolds for the development of antimicrobial cationic amphiphiles. Chem—Eur J. 2015;21:4340–9.
Zhanel GG, et al. Comparison of the next-generation aminoglycoside plazomicin to gentamicin, tobramycin and amikacin. Exp Rev Anti Infect Ther. 2012;10:459–73.
Idowu T, Arthur G, Zhanel GG, Schweizer F. Heterodimeric rifampicin–tobramycin conjugates break intrinsic resistance of Pseudomonas aeruginosa to doxycycline and chloramphenicol in vitro and in a Galleria mellonella in vivo model. Eur J Med Chem. 2019;174:16–32.
Sader HS, Castanheira M, Shortridge D, Mendes RE, Flamm RK. Antimicrobial activity of ceftazidime-avibactam tested against multidrug-resistant enterobacteriaceae and Pseudomonas aeruginosa isolates from U.S. medical centers, 2013 to 2016. Antimicrob Agents Chemother. 2017;61:e01045–17.
Wong D, van Duin D. Novel beta-lactamase inhibitors: unlocking their potential in therapy. Drugs . 2017;77:615–28.
Tängdén T. Combination antibiotic therapy for multidrug-resistant gram-negative bacteria. UPS J Med Sci. 2014;119:149–53.
Tamma PD, Cosgrove SE, Maragakis LL. Combination therapy for treatment of infections with gram-negative bacteria. Clin Microbiol Rev. 2012;25:450–70.
Tyers M, Wright GD. Drug combinations: a strategy to extend the life of antibiotics in the 21st century. Nat Rev Microbiol. 2019;17:141–55.
Nikaido H. Molecular basis of bacterial outer membrane permeability revisited. Microbiol Mol Biol Rev. 2003;67:593–656.
Singh H, Thangaraj P, Chakrabarti A. Acinetobacter baumannii: a brief account of mechanisms of multidrug resistance and current and future therapeutic management. J Clin Diagn Res. 2013;7:2602–5.
Nikaido H. Role of permeability barriers in resistance to β-lactam antibiotics. Pharm Ther. 1985;27:197–231.
Berditsch M, et al. Synergistic effect of membrane-active peptides polymyxin B and gramicidin S on multidrug-resistant strains and biofilms of Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2015;59:5288–96.
Rampioni G, et al. Effect of efflux pump inhibition on Pseudomonas aeruginosa transcriptome and virulence. Sci Rep. 2017;7:11392.
Yang X, et al. A tobramycin vector enhances synergy and efficacy of efflux pump inhibitors against multidrug-resistant gram-negative bacteria. J Med Chem. 2017;60:3913–32.
Bush K, Jacoby GA. Updated functional classification of beta-lactamases. Antimicrob Agents Chemother. 2010;54:969–76.
Lahiri SD, et al. Selection and molecular characterization of ceftazidime/avibactam-resistant mutants in Pseudomonas aeruginosa strains containing derepressed AmpC. J Antimicrob Chemother. 2015;70:1650–8.
Cabot G, Florit-Mendoza L, Sánchez-Diener I, Zamorano L, Oliver A. Deciphering β-lactamase-independent β-lactam resistance evolution trajectories in Pseudomonas aeruginosa. J Antimicrob Chemother. 2018;73:3322–31.
Ferrara A, Grassi FA, Grassi G, Piccioni PD, Grassi GG. Bactericidal activity of meropenem and interactions with other antibiotics. J Antimicrob Chemother. 1989;24:239–50.
Coulthard KP, et al. Therapeutic drug monitoring of once daily tobramycin in cystic fibrosis—caution with trough concentrations. J Cyst Fibros. 2007;6:125–30.
Leibovici L, Paul M. Aminoglycoside/B-lactam combinations in clinical practice. J Antimicrob Chemother. 2007;60:911–2.
Acknowledgements
The authors would like to thank the University of Manitoba and the Natural Sciences and Engineering Research Council of Canada (NSERC) for financial support in the form of a discovery grant (2018-06047). We would also like to thank Prof. Ayush Kumar (University of Manitoba) for providing us with the efflux deficient strains.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Ammeter, D., Idowu, T., Zhanel, G.G. et al. Development of a nebramine-cyclam conjugate as an antibacterial adjuvant to potentiate β-lactam antibiotics against multidrug-resistant P. aeruginosa. J Antibiot 72, 816–826 (2019). https://doi.org/10.1038/s41429-019-0221-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41429-019-0221-9
