
Abstract
Purpose
We studied microRNAs as potential biomarkers for Pompe disease.
Methods
We analyzed microRNA expression by small RNA-seq in tissues from the disease murine model at two different ages (3 and 9 months), and in plasma from Pompe patients.
Results
In the mouse model we found 211 microRNAs that were differentially expressed in gastrocnemii and 66 in heart, with a different pattern of expression at different ages. In a preliminary analysis in plasma from six patients 55 microRNAs were differentially expressed. Sixteen of these microRNAs were common to those dysregulated in mouse tissues. These microRNAs are known to modulate the expression of genes involved in relevant pathways for Pompe disease pathophysiology (autophagy, muscle regeneration, muscle atrophy). One of these microRNAs, miR-133a, was selected for further quantitative real-time polymerase chain reaction analysis in plasma samples from 52 patients, obtained from seven Italian and Dutch biobanks. miR-133a levels were significantly higher in Pompe disease patients than in controls and correlated with phenotype severity, with higher levels in infantile compared with late-onset patients. In three infantile patients miR-133a decreased after start of enzyme replacement therapy and evidence of clinical improvement.
Conclusion
Circulating microRNAs may represent additional biomarkers of Pompe disease severity and of response to therapy.
Similar content being viewed by others


Introduction
Pompe disease (glycogenosis type 2, OMIM 232300, ORPHA365, ICD-10 E74.0) is a metabolic myopathy caused by pathogenic variants of the GAA gene and deficiency of acid α-glucosidase (GAA), an enzyme involved in the lysosomal breakdown of glycogen.1 The primary pathological hallmarks of Pompe disease are generalized glycogen storage, most prominent in heart and skeletal muscles, and accumulation of autophagic material in skeletal muscle fibers.2
Pompe disease is typically characterized by broad clinical variability, with a phenotypic continuum that ranges from infantile-onset forms, characterized by cardiomyopathy and rapidly progressive course, to late-onset phenotypes associated with attenuated course and predominant involvement of skeletal muscles. Central nervous system involvement and motor neuron dysfunction are emerging as additional features of Pompe disease that may contribute to cognitive decline in infantile-onset forms3 and to respiratory insufficiency.4
Also patients’ response to enzyme replacement therapy (ERT) with recombinant human GAA (rhGAA) is highly variable. Although extraordinarily effective in some patients and on some aspects of the disease (most notably survival and cardiomyopathy in infantile patients; motor and respiratory function in late-onset forms), in other patients ERT results in minor effects in specific muscles with signs of continuing disease progression.5
Due to this variability, assessing patient status and response to ERT is a critical issue in the management of Pompe disease. In this respect, a major challenge is the need for reliable, measurable, and objective disease markers that are not influenced by inter- and intrainvestigator variance. Particularly, the degree of muscle involvement remains difficult to assess. Currently, clinical tests (muscle strength, muscle function, patient-reported outcomes) are in common use to this purpose.6 Although several of these tests have been specifically validated for Pompe disease,7,8,9 they still present some caveats. In particular, some of them appear to be specific for subsets of patients and require specific medical skills and collaboration by patients. Key factors in evaluating the reliability of tests to assess muscular involvement in Pompe disease are their clinical relevance and the minimal clinically important difference,9 which for some of these tests needs to be further established. Biochemical or imaging-based tests include the evaluation of the glucose tetrasaccharide (GLC4)10 in plasma and urine, muscle ultrasound,11 muscle nuclear magnetic resonance .12 However, the clinical relevance of the latter tests also requires further assessment.
We explored the possibility to use microRNAs (miRNAs) as disease markers in Pompe disease. miRNAs are small noncoding RNAs that regulate gene expression by targeting messenger RNAs. miRNAs are able to concurrently target multiple effectors of pathways in the context of a functional gene network, thereby finely regulating multiple cellular functions involved in disease development and progression.13,14,15 In several other disease conditions, including muscular dystrophies,16 the analysis of miRNA expression has led to the discovery of altered pathways in response to disease,17 and has highlighted potential targets of therapeutic intervention. Because miRNAs are variably dysregulated in these disorders, their expression profile may represent a potential biomarker in diagnostic and prognostic applications.
In this study, we comprehensively analyzed by next-generation sequencing (NGS)-based procedures the expression of miRNAs in muscle and heart of a Pompe disease murine model, and in patients’ plasma, with the aim to identify tools to assess patient clinical conditions and response to treatments.
Materials and methods
A Gaa-/- knockout Pompe disease mouse model obtained by insertion of neo into the Gaa gene exon 6 (ref. 18) was purchased from Charles River Laboratories (Wilmington, MA), and was maintained at the Cardarelli Hospital’s Animal Facility (Naples, Italy).
Animal studies were performed according to the EU Directive 86/609, regarding the protection of animals used for experimental purposes, and according to Institutional Animal Care and Use Committee (IACUC) guidelines for the care and use of animals in research. The study was approved by the Italian Ministry of Health, IACUC n. 523/2015-PR (06/11/2015). Every procedure on the mice was performed with the aim of ensuring that discomfort, distress, pain, and injury would be minimal. Mice were euthanized following ketamine xylazine anesthesia.
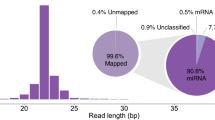
miRNAs expression profiles were analyzed by small RNA-seq in the Pompe disease mouse model (Gaa-/-)18 in comparison with wild-type animals. We analyzed two of the main disease target tissues, i.e., heart and gastrocnemius muscle, from Pompe disease and age-matched wild-type mice. The tissues were collected at different time-points (3 and 9 months) that reflect different stages of disease progression. After small-RNA sequencing, a bioinformatic analysis was carried out to assess the reliability and statistical relevance of data (Supplementary Fig. S1). The threshold value for significance used to define up-regulation or down-regulation of miRNAs was a false discovery rate (FDR) lower than 0.05.
Plasma samples from 52 Pompe disease patients were already available and stored at −80 °C at the biobanks of the seven collaborating centers (Department of Translational Medical Sciences Federico II University, Naples; Department of Neurosciences, Federico II University, Naples; Department of Neurosciences, University of Messina; Bambino Gesù Hospital in Rome; Centre for Rare Disease, Udine; Department of Neurosciences, University of Turin; Center for Lysosomal and Metabolic Diseases; and Department of Pediatrics, Erasmus University Medical Center, Rotterdam). In all patients the diagnosis was confirmed by enzymatic analysis and GAA gene sequencing. Plasma had been obtained according to standard procedures during periodic follow-up admissions to the respective hospitals. Patients (or their legal guardians) had signed an informed consent agreeing that the samples would be stored and used for possible future research purposes.
Samples from age-matched controls were analyzed for comparison. Pediatric control samples derived from residual and unused amounts of plasma collected for routine chemistry in patients undergoing minor urologic surgical procedures (phimosis, hypospadias), and did not require additional medical procedures. Patients or their legal guardians consented to the use of these samples for research purposes. Juvenile and adult control samples were obtained by healthy volunteers, who consented to the use of their blood for research.
Each patient code is composed of a two-letter code identifying the city of the collaborating center, and a progressive number assigned at the time of arrival at our lab.
Total RNA extraction preserving miRNA fraction
Total RNA, including small RNAs, was extracted using the miRNeasy Kit (Qiagen) according to the manufacturer′s instructions. RNA was quantified using a NanoDrop ND-8000 spectrophotometer (NanoDrop Technologies) and the integrity was evaluated using an RNA 6000 Nano chip on a Bioanalyzer (Agilent Technologies). Only samples with an RNA integrity number (RIN) >8.0 were used for library preparation.
Small RNA-seq analysis in tissues
Small RNA libraries were constructed using a Truseq small RNA sample preparation kit (Illumina) following the manufacturer′s protocol. Using multiplexing, we combined up to 12 samples into a single lane to obtain sufficient coverage. Equal volumes of the samples that constituted each library were pooled together immediately prior to gel purification and the 147–157 bp products from the pooled indexes were purified from a 6% polyacrylamide gel (Invitrogen). Libraries have been quality-checked using a DNA 1000 chip on a Bioanalyzer (Agilent Technologies) and quantified using the Qubit® 2.0 Fluorometer (Invitrogen). The sequencing was carried out by the NGS Core Facility at TIGEM, Naples. Cluster generation was performed on a Flow Cell v3 (TruSeq SR Cluster Kit v3; Illumina) using cBOT and sequencing was performed on the Illumina HiSeq1000 platform, according to the manufacturer’s protocol. Each library was loaded at a concentration of 10 pM, which we had previously established as optimal.
Small RNA-seq analysis in plasma
For plasma preparation EDTA was used as anticoagulant, both in patients and in mouse samples. Processing of samples from Pompe disease and control sets were conducted simultaneously to minimize batch effect. Prior to RNA extraction, a C. elegans-specific synthetic exogenous miRNA (ce-miR-39) was spiked in the samples as control for the extraction efficiency. RNA was isolated using the miRNeasy Kit (Qiagen) and reverse-transcription polymerase chain reaction (RT-PCR) was performed using miScript System (Qiagen). RNA recovery was assessed by comparing the Ct values (obtained with the assay targeting the synthetic miRNA) with a standard curve of the synthetic miRNA generated independently of the RNA purification procedure. After assessment of RNA recovery, equal amounts based on starting volume (3 μl) were used for the preparation of small RNA libraries, as described for tissues. NextSeq 500/550 High Output Kit v2 (75 cycles) Cd. FC-404-2005 was used and sequencing was performed on the Illumina NextSeq 500 platform, according to the manufacturer’s protocol. Each library was loaded at a concentration of 1.8 pM, previously established as optimal.
Bioinformatics analysis
To identify differentially expressed miRNAs (DE-miRNAs) across samples, the reads were trimmed to remove adapter sequences and low-quality ends, and reads mapping to contaminating sequences (e.g., ribosomal RNA, phIX control) were filtered out. The filtered reads of tissue samples were aligned to mouse mature miRNAs (miRBase Release 20), while filtered reads of plasma samples were aligned to human mature miRNAs using CASAVA software (Illumina). The comparative analysis of miRNA levels across samples was performed with edgeR,19 a statistical package based on generalized linear models, suitable for multifactorial experiments.
Gene Ontology and KEGG pathway enrichment analysis of miRNA targets, predicted by TargetsScan,20 was performed using the goana and kegga functions of Limma,21 with FDR <0.05 as threshold for significant enrichment.
Quantitative real-time polymerase chain reaction (qRT-PCR) of miRNA
Expression of mature miRNAs was assayed using Taqman Advanced MicroRNA Assay (Applied Biosystems) specific for miRNA selected for validation. qRT-PCR was performed by using an Applied Biosystems 7900 Fast-Real-time PCR System and a TaqMan Fast Advanced Master Mix. Primers for selected miRNAs were obtained from the TaqMan Advanced miRNA Assays. Samples were run in duplicate. Single TaqMan microRNA assays were performed according to manufacturer’s instructions (Applied Biosystems). Differences in miRNAs expression, expressed as fold changes, were calculated using the 2-∆∆Ct method. In plasma samples, to calculate ∆Cts values, the average of two normalizers was used: spike in ce-miR-39 and endogenous stable miRNA miR-93 (ref. 22). Next, to calculate ∆∆Ct values an average of five controls, each of them analyzed in three independent experiments, was used. miR-16 was used as endogenous normalizer in tissue samples.
In vivo experiments in the Pompe disease mouse model
Pompe disease mice received a single high-dose (100 mg/kg) injection of Myozyme into the retroorbital vein. Tissues (heart, gastrocnemius) were collected 48 h after the injection and miR-133 was analyzed by qRT-PCR as indicated.
The results obtained were compared with those obtained in control animals injected with equivalent volumes of saline. Four animals for each group were analyzed.
Statistical analysis
Group-wise comparisons (Fig. 4a) were performed by two-way analysis of variance (ANOVA) with Tukey post hoc test. A Student’s t test was used for the statistical analysis of the data shown in Fig. 4d and Supplementary Fig. S2.
Results
Global analysis of miRNA expression profiles in the skeletal muscle and heart of the Pompe disease mouse model
The small RNA-seq analysis in tissues from the Pompe disease mouse model generated a list of 277 miRNAs that were differentially expressed (DE-miRNA) in the two tissues examined (gastrocnemius and heart) with statistical significance, compared with control mice. The complete list and the results of the sequencing are provided in Supplementary Table S1. Figure 1 provides a summary of the results obtained in the two tissues examined and at the different time-points. The patterns of miRNA dysregulation varied depending on age, indicating changes related to disease progression, and tissues, suggesting tissue-specific involvement of different pathways. The DE-miRNA were either up-regulated or down-regulated.

a Summary of number of the differentially expressed microRNA (DE-miRNA) up- and down-regulated in gastrocnemius and heart at 3 and 9 months. b Heatmap of the DE-miRNAs identified in mice gastrocnemius at 3 and 9 months or common in both ages. c Heatmap of the DE-miRNAs identified in mice heart at 3 and 9 months or common in both ages. The colors indicate up-regulation (red) or down-regulation (green) of each DE-miRNA. KO knockout, WT wild-type
Pompe disease patients show differential expression of circulating miRNAs
We then looked at plasma samples from patients affected by Pompe disease. We decided to perform a small RNA-seq analysis on a representative subgroup of patients covering both infantile-onset (IOPD) and late-onset (LOPD) cases. We first ran a pilot small RNA-seq analysis in plasma samples from 6 patients (NA1, NA3, NA4, NA8, RD2, TO1) (3 IOPD, 3 LOPD), selected from 52 patients (information on the patients is provided in Supplementary Table S2) whose plasma samples were already available at the biobanks of the clinical centers involved in this study. Patients, all under ERT treatment, were selected for this preliminary analysis based on their phenotypes, current clinical condition, and age to have relatively homogeneous groups representative of both Pompe disease forms, and based on blood sampling time with respect to therapy (at least 10 days after the previous enzyme replacement infusion). The results obtained in IOPD patients were compared with control samples obtained from age-matched pediatric patients, while the results obtained in LOPD were compared with those of age-matched healthy volunteers.
We found 55 miRNAs that were differentially expressed with an FDR <0.05 (the complete list is provided in Supplementary Table 3) and that were either up- or down-regulated (Fig. 2). Sixteen miRNAs were differentially expressed both in tissues from Pompe disease mice and in patient plasma (Table 1). For the majority of these miRNAs the pattern of expression was different in the two species. However, this was not surprising, considering the different sources of biological samples and patient clinical heterogeneity.

(a) Summary of the number of differentially expressed microRNA (DE-miRNA) up- and down-regulated. (b) Heatmap of the 55 DE-miRNAs up-regulated (red) or down-regulated (green)
The DE-miRNAs in Pompe disease are involved in pathways that are potentially relevant for the disease pathophysiology
A literature analysis indicates that the 16 DE-miRNAs that are dysregulated both in mouse tissues and in patients’ plasma have been linked, as expected, to multiple function and pathways. The majority of them are reported to be involved in cancer-related processes, likely due to the preponderant number of studies in the literature that are focused on the role of miRNAs in cancer.
Interestingly, some DE-miRNAs are involved in pathways that are of potential relevance for Pompe disease pathophysiology, such as muscle cell proliferation, regeneration and differentiation (miR-127, miR-133, miR-136, miR-142, miR-329), autophagy (miR-26, miR-29c, miR-142, miR-183), apoptosis (miR15b, miR-26, miR-29c, miR-136, miR-144, miR-410), endoplasmic reticulum/oxidative stress (miR15b, miR-99, miR-133, miR-155, miR-144, miR-329), muscle metabolism and insulin response (miR-26, miR-29c, miR-182), inflammation (miR-142, miR-155, miR-410), fibrosis (miR-29c, miR-410), cardiomyopathies (miR-26, miR-133, miR-182, miR-410), and atrophy (miR-182). The finding of dysregulation of miRNAs involved in the process of atrophy may also be compatible both with primary muscle atrophy and with denervation atrophy.
To gather more information on the processes in which the DE-miRNAs can be functionally involved, we carried out Gene Ontology and KEGG pathway enrichment analysis using as queries the list of their predicted targets identified through TargetScan.20 The most recurrent target genes in the most frequently enriched KEGG pathways (genes that are predicted target of at least four DE-miRNAs) are shown in Fig. 3.

Circos plots of the most frequent pathways (right from top to bottom) and most frequent genes (left from bottom to top) predicted to be targeted by the 16 common DE-miRNAs
As a result, we found that a number of DE-miRNAs and their target genes are involved in processes that are potentially relevant for Pompe disease pathophysiology (Fig. 3), like MAPK, FoxO, mTOR, AMPK and insulin signaling pathways, ubiquitin-mediated proteolysis, cardiac hypertrophy, fibrosis, muscle atrophy and regeneration, autophagy, regulation of stem cells pluripotency, and myogenesis. We also found some DE-miRNAs that are implicated in other pathways, such as oxidative stress and inflammation, that have occasionally been associated with Pompe disease.23, 24 Some DE-miRNAs are involved in more than one of these pathways, which suggests that they play a significant role in Pompe disease pathophysiology, and in an intricate interplay between secondary cellular events triggered in response to glycogen storage.
miR-133a levels correlate with Pompe disease clinical forms
We selected one of the miRNAs, miR-133a, that were differentially expressed both in Pompe disease mice and in patients for further validation and confirmation by qRT-PCR. The analysis was performed in patients’ plasma from all 52 patients. Information on these patients is provided in Supplementary Table S2. Ten of the patients were affected by IOPD, whereas 42 had LOPD.
miR-133a has been reported to be a member of the myogenic miRNAs (so-called Myo-miRs);25 is expressed in the skeletal and cardiac muscles of mammals, birds and zebrafish; and is dysregulated in cardiac hypertrophy and other cardiac disorders,26 and in muscular dystrophies.16, 27
qRT-PCR analysis showed minor variations of miR-133a levels with respect to age in controls (Fig. 4a), with slightly higher levels in younger individuals. Conversely, quantitative analysis confirmed that miR-133a is up-regulated in Pompe disease patients (Fig. 4a), as already observed by small RNA-seq. In IOPD patients miR-133a levels were significantly (p = 0.000005) higher (12.44 to 414.96-fold) than those of age-matched controls and did not overlap with controls. IOPD patients had the highest levels of miR-133a, which were significantly higher than those observed in LOPD patients (p = 0.000441). In LOPD patients miR-133a was also significantly increased (p = 0.005908) compared with age-matched controls, but with lower levels, with a broader distribution of values, and with some overlap between controls and LOPD patients.

a In infantile-onset Pompe disease (IOPD) patients miR-133a levels were significantly (p = 0.000005) higher (12.44- to 414.96-fold) than those of age-matched controls. IOPD patients had significantly higher levels compared with late-onset Pompe disease (LOPD) patients (p = 0.000441). In LOPD patients miR-133a was also significantly increased (p = 0.005908) compared with age-matched controls. P analysis of variance (ANOVA) = 0.03662. miR-133a was also elevated in patients with other myopathies, including Becker muscular dystrophy (BMD, gray triangles), Steinert myotonic dystrophy (MD, gray circles), McArdle muscle (McA, gray diamonds). b Expression level of miR-133a in plasma from 3 IOPD. For each patient, miR-133a was analyzed before first enzyme replacement therapy (ERT) infusion (T0) and after 3 years of treatment (NA3), 7 months (NA5), and 3 years and 3 months (RD8) (T1), and after near-complete correction of clinical manifestations. c Expression level of miR-133a in plasma from 10 PD patients pre-ERT infusion and 24 h post-ERT. d Effect of a single high-dose infusion of rhGAA (100 mg/kg). Expression of miR-133a was analyzed in gastrocnemii from 9-month-old Pompe disease mice, compared with wild-type age-matched animals and 48 h after rhGAA infusion. KO knockout, WT wild-type
As positive control, we performed the analysis in samples from two patients affected by Becker muscular dystrophy. In addition, we analyzed samples from patients with other myopathies, including three patients with McArdle glycogenosis and two patients with Steinert myotonic dystrophy. Compared with age-matched controls all these patients showed increased miR-133a levels (Fig. 4a).
We also measured miR-133a levels in plasma from the murine Pompe disease model. MiR-133a was modestly elevated only in older mice (15 months of age) (Supplementary Fig. S2). Considering that the phenotype observed in the knockout mouse is relatively mild (with the exception of the presence of cardiomyopathy) and allows for near normal survival and fertility, these data are not surprising.
ERT affects circulating miR-133a levels in Pompe disease
We then tested whether miR-133a levels are influenced by ERT with rhGAA. Only for 3 IOPD patients (NA3, NA5, RD8) were stored plasma samples available, which had been obtained before starting ERT (T0), at the age of 9, 2 and 3 months respectively. Before starting ERT all patients showed the full clinical picture of IOPD, with hypertrophic cardiomyopathy and severe hypotonia. In the pre-ERT samples miR-133a levels were high. After 3 years of treatment (NA3), 7 months (NA5), and 3 years and 3 months (RD8), respectively, a good clinical response to ERT had already been achieved in all patients, with near-complete correction of cardiac hypertrophy as assessed by cardiac ultrasound scan, and adequate motor function for age. At that time plasma miR-133a levels were substantially decreased in all patients (Fig. 4b), suggesting a correlation between miRNA levels and the effects of treatment.
We also analyzed the effects of single ERT infusions in ten patients, for which samples before and 24 h after an ERT infusion were available in our laboratories (Fig. 4c). One of these samples (NA3) had been obtained after the first ERT infusion and pretreatment levels corresponded to those shown in Fig. 4b. All other patients had already been treated for variable periods. All patients displayed up-regulation of miR-133a before ERT with respect to the mean of control samples. In seven patients the level of miR-133a decreased after ERT, with most evident decreases in the patients with the highest miR-133a preinfusion levels.
We also tested the effect of a single infusion of rhGAA in the Pompe disease mouse model. As previously shown, in the Pompe mouse miR-133a is down-regulated in gastrocnemius, while in heart it is normally expressed. We gave a single injection of rhGAA at a high dose (100 mg/kg) to obtain detectable changes in miR-133a expression. Forty-eight hours after the injection, tissues were collected and analyzed by qRT-PCR. In gastrocnemius miR-133a levels returned to values that are close to those measured in wild-type animals (Fig. 4d), while no changes were observed in heart (not shown).
Discussion
In this study we have evaluated whether miRNA profiles may represent potential biomarkers for Pompe disease. Small RNA-seq was selected as a tool to analyze miRNA expression because this approach is well suited for large-scale quantitative analysis of nucleotide sequences.
The design of the study, with an initial step in which we first performed the small RNA-seq analysis in the Pompe disease mouse model and subsequently in a selected number of patients, represented a compromise between the potential of NGS and the costs of this methodology. An advantage of using the animal model was the possibility to run our preliminary analysis in a homogenous sample, with a common genetic background and uniform disease progression, and to look at the tissues that are most affected by disease pathology. This initial approach allowed us to identify and select a restricted number of miRNAs that are dysregulated in Pompe disease. These miRNAs were subjected to a bioinformatic analysis to gather information on their possible role in Pompe disease pathophysiology.
The DE-miRNAs that we selected in this way were (1) dysregulated in Pompe disease (both in mice tissues and in patients’ plasma); (2) potentially relevant for the disease pathophysiology according to the bioinformatic and literature analysis; and (3) measurable in samples, like plasma, that are readily available in Pompe disease patients and in general require minimally invasive procedures.
One of these miRNAs was further validated in the whole cohort of our patients by qRT-PCR. miR-133a was particularly attractive, because it had already been proposed as a biomarker for Duchenne/Becker muscular dystrophy,16 and because it has been shown to be involved in processes including muscle regeneration, atrophy, and inflammation.
Both in IOPD and in LOPD patients miR-133a was significantly elevated. However, the levels observed in IOPD were significantly higher compared with those measured in patients with attenuated phenotypes, suggesting a correlation between miR-133a levels and the clinical forms of the disease. This difference was not due to an age-related effect, because in age-matched controls miR-133a levels were only modestly higher than those obtained at later ages.
While in IOPD patients, who show a more homogeneous phenotype,28,29,30 we consistently found increased miR-133a levels, the results in LOPD showed marked variability. It was thus impossible, in a relatively limited number of patients, to establish clear correlations between individual parameters (such as age, diseases stage, clinical scores, motor performance, need for ventilator support). It is reasonable to think that in LOPD patients, who show an extremely broad rage of phenotypes,31 several factors (muscle mass, fibrosis, in addition to age, disease severity, etc.) concomitantly contribute to the expression of miR-133a and to its plasma levels. We believe that studies in larger cohorts of patients, based on the concerted effort of international consortia and on the collaboration of the leading centers in the follow-up of Pompe disease patients, may further validate the results of our study, and address possible correlations between miRNA levels and LOPD patient status, response to therapy, or outcome.
An important finding of our study is that miR-133a levels showed a trend toward decrease in response to ERT. Samples before the start of treatment were only available for three patients. In all of them we found a clear decrease of miR-133a, concomitant to overt clinical improvement. miR-133a levels also decreased in seven of ten patients even after a single injection after ERT treatment. In addition, we found normalization of miR-133a in gastrocnemii from Pompe disease animals after single injection of high-dose rhGAA. Our results suggest that miR-133a may represent an adjunct marker of ERT effects, to be used in combination with clinical and biochemical measures.
The availability of a broad range of reliable tests appears particularly important for the development of guidelines for patient monitoring, for ERT inclusion and exclusion criteria that are currently being defined in some countries,32 to correlate different ERT regimens and patient response to treatment, and to optimize and personalize treatment protocols. In addition, disease markers that provide information on Pompe disease pathophysiology may allow for identification of dysregulated pathways, new therapeutic targets, and, possibly, for development of novel therapeutic strategies.
We chose to use one DE-miRNA as a measurable marker in our cohort of Pompe disease patients. However, should the costs of NGS become more affordable (as is indeed expected in the coming years, thanks to the development of second-generation technologies and more flexible instruments), this approach may be proposed to collect a large body of data that may be even more informative in patient follow-up and allow for the identification of a specific “signature” of Pompe disease, and of disease progression, outcome, or response to therapies.
References
van der Ploeg AT, Reuser AJ. Pompe’s disease. Lancet. 2008;372:1342–1353.
Shea L, Raben N. Autophagy in skeletal muscle: implications for Pompe disease. Int J Clin Pharmacol Ther. 2009;47(suppl 1):S42–47.
Ebbink BJ, Poelman E, Classic infantile Pompe patients approaching adulthood: a cohort study on consequences for the brain. Dev Med Child Neurol. 2018;60:579–586.
Fuller DD, ElMallah MK. The respiratory neuromuscular system in Pompe disease. Respir Physiol Neurobiol. 2013;189:241–249.
Prater SN, Banugaria SG, DeArmey SM, et al. The emerging phenotype of long-term survivors with infantile Pompe disease. Genet Med. 2012;14:800–810.
Schoser B, Laforet P, Kruijshaar ME, et al. 208th ENMC International Workshop: formation of a European Network to develop a European data sharing model and treatment guidelines for Pompe disease Naarden, The Netherlands, 26-28 September 2014. Neuromuscul Disord. 2015;25:674–678.
Angelini C, Semplicini C, Ravaglia S, et al. New motor outcome function measures in evaluation of late-onset Pompe disease before and after enzyme replacement therapy. Muscle Nerve. 2012;45:831–834.
van der Beek NA, Hagemans ML, van der Ploeg AT, van Doorn PA, Merkies IS. The Rasch-built Pompe-specific activity (R-PAct) scale. Neuromuscul Disord. 2013;23:256–264.
Lachmann R, Schoser B. The clinical relevance of outcomes used in late-onset Pompe disease: can we do better? Orphanet J Rare Dis. 2013;8:160.
Young SP, Zhang H, Corzo D, et al. Long-term monitoring of patients with infantile-onset Pompe disease on enzyme replacement therapy using a urinary glucose tetrasaccharide biomarker. Genet Med. 2009;11:536–541.
Vill K, Schessl J, Teusch V, et al. Muscle ultrasound in classic infantile and adult Pompe disease: a useful screening tool in adults but not in infants. Neuromuscul Disord. 2015;25:120–126.
Pichiecchio A, Uggetti C, Ravaglia S, et al. Muscle MRI in adult-onset acid maltase deficiency. Neuromuscul Disord . 2004;14:51–55.
Bushati N, Cohen SM. microRNA functions. Annu Rev Cell Dev Biol . 2007;23:175–205.
Bartel DP. MicroRNAs: target recognition and regulatory functions. Cell. 2009;136:215–233.
Pasquinelli AE. MicroRNAs and their targets: recognition, regulation and an emerging reciprocal relationship. Nat Rev Genet . 2012;13:271–282.
Cacchiarelli D, Legnini I, Martone J, et al. miRNAs as serum biomarkers for Duchenne muscular dystrophy. EMBO Mol Med. 2011;3:258–265.
Allegra A, Alonci A, Campo S, et al. Circulating microRNAs: new biomarkers in diagnosis, prognosis and treatment of cancer (review). Int J Oncol . 2012;41:1897–1912.
Raben N, Nagaraju K, Lee E, et al. Targeted disruption of the acid alpha-glucosidase gene in mice causes an illness with critical features of both infantile and adult human glycogen storage disease type II. J Biol Chem. 1998;273:19086–19092.
Robinson MD, McCarthy DJ, Smyth GK. edgeR: a Bioconductor package for differential expression analysis of digital gene expression data. Bioinformatics. 2010;26:139–140.
Chiang HR, Schoenfeld LW, Ruby JG, et al. Mammalian microRNAs: experimental evaluation of novel and previously annotated genes. Genes Dev. 2010;24:992–1009.
Ritchie ME, Phipson B, Wu D, et al. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015;43:e47.
Perfetti A, Greco S, Cardani R, et al. Validation of plasma microRNAs as biomarkers for myotonic dystrophy type 1. Sci Rep. 2016;6:38174.
Palermo AT, Palmer RE, So KS, et al. Transcriptional response to GAA deficiency (Pompe disease) in infantile-onset patients. Mol Genet Metab. 2012;106:287–300.
Lim JA, Li L, Shirihai OS, Trudeau KM, Puertollano R, Raben N. Modulation of mTOR signaling as a strategy for the treatment of Pompe disease. EMBO Mol Med. 2017;9:353–370.
Lagos-Quintana M, Rauhut R, Meyer J, Borkhardt A, Tuschl T. New microRNAs from mouse and human. RNA. 2003;9:175–179.
Liu Y, Liang Y, Zhang JF, Fu WM. MicroRNA-133 mediates cardiac diseases: mechanisms and clinical implications. Exp Cell Res. 2017;354:65–70.
Zaharieva IT, Calissano M, Scoto M, et al. Dystromirs as serum biomarkers for monitoring the disease severity in Duchenne muscular dystrophy. PLoS ONE. 2013;8:e80263.
van den Hout HM, Hop W, van Diggelen OP, et al. The natural course of infantile Pompe’s disease: 20 original cases compared with 133 cases from the literature. Pediatrics. 2003;112:332–340.
Kishnani PS, Corzo D, Nicolino M, et al. Recombinant human acid [alpha]-glucosidase: major clinical benefits in infantile-onset Pompe disease. Neurology. 2007;68:99–109.
Kishnani PS, Hwu WL, Mandel H, et al. A retrospective, multinational, multicenter study on the natural history of infantile-onset Pompe disease. J Pediatr. 2006;148:671–676.
Kroos M, Hoogeveen-Westerveld M, Michelakakis H, et al. Update of the Pompe disease mutation database with 60 novel GAA sequence variants and additional studies on the functional effect of 34 previously reported variants. Hum Mutat. 2012;33:1161–1165.
van der Ploeg AT, Kruijshaar ME, Toscano A, et al. European consensus for starting and stopping enzyme replacement therapy in adult patients with Pompe disease: a 10-year experience. Eur J Neurol . 2017;24:768–e731.
Acknowledgements
This study would have never been possible without the support of the Acid Maltase Deficiency Association (AMDA, Helen Walker Research Grant, 2014 to GP). This work was supported in part by the Italian Agency of Medicines (AIFA-2016-02364305 grant to GP). We thank the TIGEM NGS and Bioinformatic cores for their work, Roberta Tarallo, Laura Marra, Giovanni Nassa, and Giorgio Giurato for helpful suggestions. We thank Graciana Diez-Roux for manuscript revision.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
The authors declare that they have no conflicts of interest.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Tarallo, A., Carissimo, A., Gatto, F. et al. microRNAs as biomarkers in Pompe disease. Genet Med 21, 591–600 (2019). https://doi.org/10.1038/s41436-018-0103-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41436-018-0103-8
