
Abstract
The aim of this study was to evaluate the effect of omega-3 fatty acid supplementation on female sexual function during pregnancy. The present study was a double-blind randomized controlled clinical trial performed on 124 pregnant women (62 people in each group) at 16–22 weeks of gestation who referred to health centers in Ilam in 2020 to receive prenatal care. The intervention group received 300 mg of omega-3 supplements and the control group received placebo once a day for 8 weeks. Data collection tools in this study included a demographic questionnaire, three 24-h dietary recall (24HR), female sexual function index (FSFI), and Van den Bergh Pregnancy-Related Anxiety Questionnaire (PRAQ). Before intervention, the total score of sexual function in the intervention group and control groups, showed no statistically significant difference (P = 0.123). However, 4 and 8 weeks after intervention, the mean total score of sexual function in the intervention group was significantly higher than that of the control group after intervention (P < 0.0001). Before intervention, the total score of gestational anxiety in the intervention and control groups, showed no statistically significant difference (P = 0.149). However, 4 and 8 weeks after intervention, the mean total score of gestational anxiety in the intervention group was significantly lower than that of the control group (P < 0.0001). Based on three 24-h dietary recall, regardless of daily intake of 300 mg of omega-3 supplement, the percentage of polyunsaturated fatty acid (PUFA) intake from daily energy intake was not statistically significant between the intervention and control groups from baseline to follow-up (P > 0.01). Based on the results of this study, omega-3 supplementation could improve sexual function in pregnant women by preventing increased pregnancy anxiety. However, more studies are needed to prove the effectiveness of omega-3s on female sexual function during pregnancy. This study was approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (Ref. ID: IR.AJUMS.REC.1398.935) and registered in Iranian Registry of Clinical Trials (Ref. ID: IRCT20200415047078N1).
Similar content being viewed by others


Introduction
Sexual dimension is one of the most inherent human emotions, which manifests in the deepest human relationships [1] and plays an important role in a person’s quality of life and well-being [2, 3]. Different periods of a woman’s life and the changes that occur therein can affect a woman’s sexual life [4]. Pregnancy is one of the most critical periods in women’s life characterized with profound changes that expose them to mental and physical changes and thus affecting the physical and emotional needs of the couple [5, 6].
In a systematic review conducted by Serati et al. The results showed that in most studies, sexual function was reduced during pregnancy [7]. Nearly half of women of the population experience sexual dysfunction during pregnancy, with the prevalence of this disorder varying according to gestational age [8]. In a study on pregnant women in Turkey, the prevalence of this disorder was 54.7% [9] while the rate reported for Egypt was 68.8% [10] and in Iran, results of different studies range from 33.3% [11] to 79% [12].
Numerous factors during pregnancy can be associated with changes in sexual function, including hormonal [13], psychological, relational and social factors [1, 14]. In this regard, the results of previous studies indicate that mental disorders such as anxiety play a prominent role in changing sexual function in women during pregnancy [15, 16].
Anxiety is a common symptom during pregnancy [17] for which no definitive treatment is often offered [18]. Numerous studies have examined the relationship between mental disorders and sexual function. Anxiety can be associated with inhibition of orgasm, sexual arousal, and increased risk of dyspareunia [19,20,21,22,23].
Because some sexual dysfunctions are caused by psychological factors, treatments aimed improving the mental health problems of pregnant women seem to be effective in promoting sexual function [24]. Currently, while no approved drug treatment for sexual dysfunction in pregnant women has been proposed [25].
Recent studies have dealt with the effect of omega-3 diets, supplements, and fish on sexual activity, and most of the studies in this area have evaluated sexual function in men [26, 27], with women being poorly represented in the literature [28, 29]. Gaskin et al., was reported a positive relationship between the consumption of seafood, fish and the sexual activity of couples [30].
Omega-3 is a type of dietary supplement [31] that is essential for the development and proper function of body tissues [32]. Omega-3 also increases serotonin and dopamine levels in the body [33] that play a significant role in the formation of sexual functions and the integrated functions of the central nervous system such as mood and anxiety [34]. Therefore, due to the high prevalence of stress, anxiety, and mood swings in pregnancy, it may be possible to use nutritional supplement therapy involving omega-3 to improve sexual function. The results of some studies indicate that diets low in omega 3 are associated with increased mood disorders whereas diets high in this essential fatty acid are associated with reduced anxiety [35,36,37]. The results reported in Alvarez et al. indicated that there was a moderate association between omega-3 intake and anxiety symptoms in pregnancy [38]. In some studies, omega-3 have been associated with increased uterine blood flow [39, 40], which may lead to improved sexual function [41].
Therefore, given the negative effects of sexual dysfunction in pregnant women and its complications on family and society, and paucity of research on the effect of omega-3 supplements on sexual function in pregnant women, the present study examined the effect of omega-3 fatty acid supplementation on sexual function and gestational anxiety of pregnant women. Such intervention could be used as a treatment option in improving female sexual dysfunction during pregnancy if effective results are achieved.
Method
The present study is a double-blind controlled randomized clinical trial conducted between June 2020 and November 2020. Participants in the study included pregnant women aged 18–42 who referred to health centers in Ilam, west of Iran to receive prenatal care.
Women eligible to participate in this study were those having the ability to read and write, having coitus, experiencing their first pregnancy, being at gestational age of 16–22 weeks, having a body mass index between 18.5–25 (Known as the normal range of body mass index). Eating fish less than twice a week, receive less than 6% polyunsaturated fatty acids (PUFA) of daily calories intake from food [42], obtaining a sexual function score of less than 26.55 (A total score less than or equal to 26.55 indicates sexual dysfunction [43]).
Exclusion criteria also included miscarriage threat, preterm delivery, placenta previa, multiple pregnancy, a history of anxiety or hospitalization in psychiatric wards, taking anxiety-reducing drugs, drugs that affect libido such as antihypertensive, and antidepressant drugs, experiencing an accident in the last three months, having a chronic physical or mental illness, taking omega-3 or other supplements out of routine (iron and folic acid), and unwillingness to participate in the study.
Sample size estimates
Based on a study by Jalali-Chimeh et al. [44], assuming a change in the mean (standard deviation) score of sexual function from 17.1 ± 4.9 to 25 ± 5.3 after 8 weeks of treatment in the intervention and placebo groups, respectively, with a α = 0.01, two-sided tast, a statistical power of 99 % and Effect size of 0.98, the sample size was calculated to be 52 women for each group using G-power software. Given the possible 20% attrition rate, 62 women were allocated to each of intervention and control groups.
Sampling
After approval of the study protocol by the ethics committee of Jundishapur Ahvaz University of Medical Sciences and obtaining permission to perform sampling, in a certain period of time, pregnant women with a gestational age of 16 to 22 weeks from all health centers with different socio-economic situations is picked. Then, according to the information entered in the medical record of each woman, the inclusion and exclusion criteria were applied. Eligible mothers were then called by phone, were briefed on the general objectives of the study and its method.
The initial samples who were willing to take part were invited to the center to complete the questionnaires and submit informed written consent at the first visit for pregnancy care. Then, in the first face-to-face meeting, the participants were given detailed explanations about the study objectives, duration and method of study, the confidentiality of information, and their right to withdraw from the study at any stage of the study if they were not willing to participate in it.
In the next stage, the following questionnaires were completed by the participants: Van den Bergh Pregnancy-Related Anxiety Questionnaire (to measure gestational anxiety), FSFI (to measure sexual function) and three 24-hour dietary recall (24HR) (to evaluate the participants’ diet). The 24-hour dietary recall was performed 3 days a week (on 2 weekdays and once a weekend). Women whose consumption of foods containing polyunsaturated fatty acids (PUFA) in their diet were less than 6% of daily caloric intake and their sexual function score was less than 26.55 were selected to participate in the study.
Randomization and blinding
Random allocation
In this study, after select of final sampling, random sequencing was performed by block generation method using a random sequence computer program. Participants were assigned to intervention and control groups using block randomization with four and six blocks and 1: 1 allocation ratio.
Allocation concealment
In order to conceal random allocation in this study, the central randomization method was used. In this method, a random sequence was provided to an individual in a specific center. The researcher contacted the relevant center and asked about the random assignment of the participant to a specific group.
Blinding
Blinding in this study involved preparing the drugs (omega-3 supplement and placebo) in identical shape and color and in the required number. They were then labelled A or B by a pharmacist, so that only the pharmacist knew which code represented the omega-3 supplement and which was for the placebo. In this study, neither the participants nor the researcher had any information about drug labeling until the end of the research and after analyzing the data.
Data collection tools
The 24-h dietary recall questionnaire: This questionnaire is one of the common questionnaires in the study of nutrition and type of food consumed that has been used in many studies on different populations of the world [45, 46] including Iran [47,48,49]. In this questionnaire, the individual records all the details of what they have eaten and drunk in the last 24 h.
In order to increase its accuracy and reliability, the 24-h dietary recall is performed 3 days a week (on 2 weekdays and once a weekend). The completed checklist are then provided to the nutritionist and the average percentages of food groups including carbohydrates, proteins, total fatty acid, saturated fatty acids, mono and polyunsaturated fatty acids included omega-6 (linolenic acid (LA)), and omega-3 (Alpha linolenic acid (ALA), Eicosa pentaenoic acid (EPA), Docosa hexaenoic acid (DHA)) are determined separately by the nutritionist using the computer software Nutrition4 (N4).
Van den bergh pregnancy-related anxiety questionnaire
This questionnaire includes 58 questions in the following five dimensions: fear of childbirth, fear of giving birth to a child with physical or mental problems, fear of change in marital relations, fear of changes in mood and its consequences on the child, and self-centered fears or the fear of changes in the mother’s personal life. Each item is scored from 0 to 7. The range of scores of the questionnaire is from zero to 406. The validity and reliability of this questionnaire have been evaluated in several studies. Acceptable Cronbach’s alphas for this questionnaire were obtained in Huizink et al. (0.76) [50] and Khanzad et al. (0.76) [51].
Female sexual function index (FSFI)
This questionnaire includes 19 questions that measure women’s sexual performance in six independent domains of sexual desire, arousal, lubrication, pain, and satisfaction. The scores of each domain are obtained by adding the scores of the questions of each domain and multiplying it by a coefficient. A higher score indicates better sexual function. Based on the weighting of the domains, the maximum score for each domain is 6 and the maximum total score is 36. A total score less than or equal to 26.55 indicates sexual dysfunction [42]. FSFI is a standard tool whose reliability and validity were confirmed by Rosen et al. in 2000 [52]. In Iran, the reliability and validity of the Persian version of this questionnaire was confirmed by Fakhri and his colleagues in 2012. The reliability coefficient of test and retest for each domain of the questionnaire was (0.73–0.86), and the internal consistency was in the acceptable range (0.72–0.90) [53].
Intervention
This study was approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (Ref. ID: IR.AJUMS.REC.1398.935) and registered in Iranian Registry of Clinical Trials (Ref. ID: IRCT20200415047087N1). After random allocation, the intervention group received omega-3 supplements made by Zahravi Pharmaceutical Company of Tabriz containing 300 mg of omega-3 (EPA: 180 mg, DHA: 120 mg) for 8 weeks daily (Numerous articles have stated that it is safe to receive 300 mg of omega3 per day during pregnancy [54, 55]). The control group received a placebo made of corn oil by Zahravi Pharmaceutical Company. The capsules were identical in terms of color, shape, size and packaging. The control group received placebo capsules (without effective ingredients) according to the instructions of the intervention group.
All participants also took their folic acid and iron routine supplements during the intervention. Participants were asked to write it down and inform the researcher if they had changed their usual eating habits during the study or had been recommended to use a special supplement by a doctor or health care provider. Participants were advised not to take any supplements other than those provided by the research team.
Assessment during Follow-up
Every 2 weeks, the researcher obtained a brief history of the participants in both study groups. Participants were also asked to inform the researcher if they developed any allergies or complications, did not take the drug for 3 days or more, or were not willing to continue participation.
Four and 8 weeks after the intervention, female sexual function index (FSFI), three 24-h dietary recall, and Pregnancy-Related Anxiety Questionnaire (PRAQ) were completed by the participants again.
Statistical analyses
In order to analyze the data, descriptive statistical methods including: frequency distribution tables, graphs and numerical indicators such as mean and standard deviation were used to describe the studied variables. The normal distribution of the data was assessed using the Kolmogorov–Smirnov test. Then, independent and repeated measures t-test were used to compare the two groups. Data were analyzed using SPSS version 22.
Results
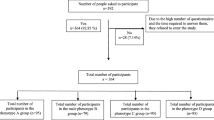
The initial participants of the study were 124 mothers. Three participants in the intervention group and two participant of control group were excluded due to unwillingness to cooperate. Finally, 59 mothers in the experimental group and 60 mothers in the control group were subjected to statistical analysis (Fig. 1).

CONSORT Flow Diagram of the progress through the phases of the trial.
The mean age of the participants and their gestational age were 29.93 ± 3.64 and 17.33 ± 1.43 in the intervention group and 26.96 ± 4.35 and 17.71 ± 1.42 in the control group, respectively.
Table 1 compares the intervention and control groups in terms of their qualitative and quantitative demographic variables. As shown in this table, the two groups were not significantly different in terms of these demographic variables.
The repeated measures t-test was used to compare the means of scores obtained in the two groups before the intervention, and 4 and 8 weeks after it. The results of this test indicate that over study period, the mean score of sexual function in the intervention group increased significantly in all dimensions except pain during intercourse (P < 0.0001), while this mean did not change significantly over this period in the control group (P = 0.082) (Table 2).
Before intervention, the total score of sexual function was 21.47 ± 2.03 in the intervention group and 22.09 ± 2.40 in the control group, which shows no statistically significant difference between the two groups (P = 0.133). However, 4 and 8 weeks after the intervention, this score rose to 25.49 ± 2.50 and 26.91 ± 2.34 in the intervention group and to 22.24 ± 1.81 and 22.93 ± 1.97 in the control group, respectively. Therefore, after the intervention, the mean total score of sexual function in the intervention group was significantly higher than that in the control group (P < 0.0001). (Table 2 and Fig. 2).

Changes in total sexual function score before and after the treatment in control and intervention groups.
Table 3 shows the desirability and undesirability of sexual function of the participants. In the intervention group, the mean score of sexual function of approximately 39% of the participants reached the desired level after 4 weeks of intervention while after 8 weeks of intervention, this was true for 54.2% of the participants. In the control group, on the other hand, after 4 and 8 weeks these rates were 3.3 and 10%, respectively, which indicates a significant difference between the two groups (P < 0.0001).
According to Table 4, the mean calorie consumption and the mean food group intake including proteins, carbohydrates, saturated and unsaturated fats were not statistically significant in the two groups of baselines to follow-up (P > 0.01).
The trend of changes in gestational anxiety before the intervention and 4 and 8 weeks after it indicates that over time, the mean score of gestational anxiety in the intervention group did not increase significantly (P = 0.071) while this score significantly increase over the study period in the control group (P < 0.0001) (Fig. 3).

Changes in total of gestational anxiety score before and after treatment in control and intervention groups.
Before intervention, the total score of gestational anxiety was 203.83 ± 14.54 in the intervention group and 207.60 ± 13.72 in the control group, which shows no statistically significant difference between the two groups (P = 0.149). However, 4 and 8 weeks after the intervention, this score was 205.10 ± 21.07 and 207.67 ± 14.24 in the intervention group and 226.15 ± 16.41 and 224.45 ± 14.55 in the control group, respectively. Therefore, after intervention, the mean total score of gestational anxiety in the intervention group was significantly lower than that in the control group (P < 0.0001) (Table 5).
Discussion
The aim of this study was to evaluate the effect of omega-3 fatty acid supplementation on female sexual function during pregnancy. According to the results obtained, daily consumption of 300 mg of omega 3 improved the overall score and dimensions of female sexual function during pregnancy. However, despite the improvement in the overall sexual function and most of its dimensions, omega-3s could not reduce pain during intercourse in women. In addition, omega-3 intake was associated with reduced gestational anxiety.
As mentioned earlier, at the time of writing this paper, no study was found on the effectiveness of omega-3 supplements in improving female sexual function during pregnancy. However, some studies have dealt with the effect of omega-3 containing diets on sexual function. Most of these studies have examined the effect of omega-3 on sexual function in men and on the quality and quantity of sperm [26, 56].
Of course, a few studies have addressed the efficacy of omega-3 in non-pregnant women. In a study, consumption of unsaturated fatty acids was associated with improved libido and a higher sexual intercourse frequency in couples planning pregnancy [30]. In another study, two-month consumption of fenugreek seeds containing unsaturated fatty acids was associated with positive and significant results in increasing female libido [57].
Various mechanisms have been proposed to explain the above findings, including improved blood flow in the body [39] especially in the pelvic organs, which can also lead to improved sexual function [41]. In a study on women with breast cancer, 6-month omega-3 intake significantly reduced vaginal atrophy and dryness by altering lactobacilli, cell maturation, and pH [58], which could be explained by increased pelvic blood flow.
Another mechanism that has recently attracted scholarly attention is the role of reducing inflammatory factors in improving sexual function [59]. In fact, omega-3 can have an anti-inflammatory role in improving sexual function. In two studies on women with diabetes, a Mediterranean diet rich in omega-3s improved sexual function, especially in the dimensions of desire and arousal [60, 61].
Improved mood induced by omega-3 consumption is another mechanism explaining improved sexual desire. The results presented in some studies indicate a significant relationship between consumption of omega-3 containing foods and reduced anxiety [35, 37]. Due to the fact that pregnancy and its changes increase the incidence of anxiety, and that Covid-19 pandemic has its own share of its limitations and complications leading to increased anxiety in pregnant women [62, 63], it can be argued that omega-3 supplementation could improve and increase women’s sexual desire during pregnancy by reducing their anxiety [64].
In one study, omega-3 supplementation along with exercise and yoga for 12 weeks did not significantly improve the sexual quality of life in postmenopausal women [65], which is not consistent with our results. This discrepancy in results could be explained by the many differences between postmenopausal women and pregnant women in terms of emotional, biological, and psychological changes.
The strengths of this study include the following: First, to the best of our knowledge, this was the first study to investigate the effect of omega-3 supplementation on female sexual function during pregnancy. Second, in this study, we tried to reduce the impact of the participants’ routine diet as an interfering factor by examining the type of food consumed. Despite these strengths, this study has a number of limitations. First: We did not measure omega-3 levels in the blood of pregnant mothers before and after the intervention, which if done, could have led to more accurate results. Second: The present study was conducted in a geographical area of Iran where people often have a traditional lifestyle and talking about sexual issues is a taboo, and this might have affected the genuineness of the responses provided by the participants in both study groups.
Conclusion
Based on the findings of this study, it can be concluded that omega-3 supplementation can be effective in improving anxiety and sexual function in women during pregnancy. However, taking supplements did not improve the pain of intercourse in our study. It is likely that this dimension of sexual function is influenced by other factors, which need further investigation. Future studies with larger sample sizes and studies comparing the effect of omega-3 as opposed to other treatments on sexual dysfunction are recommended.
Data availability
The datasets generated and/or analysed during the current research are not publicly available as individual privacy could be compromised but are available from the corresponding author on reasonable request.
References
Khajehei M, Doherty M. Women’s experience of their sexual function during pregnancy and after childbirth: a qualitative survey. Br J Midwifery. 2018;26:318–28.
Anderson RM. Positive sexuality and its impact on overall well-being. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz. 2013;56:208–14.
Ferreira DQ, Nakamura MU, Souza ED, Mariani Neto C, Ribeiro MC, Santana TD, et al. Sexual function and quality of life of low-risk pregnant women. Rev Brasileira de Ginecologia e Obstetrícia. 2012;34:409–13.
Anğın AD, Özkaya E, Çetin M, Gün I, Sakin O, Ertekin LT, et al. Comparison of female sexual function and sexual function of their partners between groups of pregnant and non-pregnant women. Ginekologia Pol. 2020;91:235–9.
Aydin M, Cayonu N, Kadihasanoglu M, Irkilata L, Atilla MK, Kendirci M. Comparison of sexual functions in pregnant and non-pregnant women. Urol J. 2015;12:2339–44.
Pauleta JR, Pereira NM, Graça LM. Sexuality during pregnancy. J Sex Med. 2010;7:136–42.
Serati M, Salvatore S, Siesto G, Cattoni E, Zanirato M, Khullar V, et al. Female sexual function during pregnancy and after childbirth. J Sex Med. 2010;7:2782–90.
Daud S, Zahid AZM, Mohamad M, Abdullah B, Mohamad NAN. Prevalence of sexual dysfunction in pregnancy. Arch Gynecol Obstet. 2019;300:1279–85.
Aksoy Derya Y, Gök Uğur H, Özşahin Z. Effects of demographic and obstetric variables with body image on sexual dysfunction in pregnancy: A cross-sectional and comparative study. Int J Nurs Pract. 2020;26:e12829.
Ahmed MR, Madny EH, Sayed, Ahmed WA. Prevalence of female sexual dysfunction during pregnancy among Egyptian women. J Obstet Gynaecol Res. 2014;40:1023–9.
Hajnasiri H, Moafi F, Nami M, Safaralinezhad A. Sexual dysfunction and its related factors among pregnant women referred to health centers in Qazvin, Iran. Soc Health Behav. 2020;3:27–34.
Nik-Azin A, Nainian MR, Zamani M, Bavojdan MR, Bavojdan MR, Motlagh MJ. Evaluation of sexual function, quality of life, and mental and physical health in pregnant women. J Fam Reprod health. 2013;7:171.
Sim L, Chopik WJ, Wardecker BM, Edelstein RS. Changes in prenatal testosterone and sexual desire in expectant couples. Hormones Behav. 2020;125:104823.
Hajnasiri H, Aslanbeygi N, Moafi F, Mafi M, Bajalan Z. Investigating the relationship between sexual function and mental health in pregnant females. IJPN. 2018;6:33–40.
Alidost F, Dolatian M, Shams J, Nasiri M, Sarkhoshpour E. The correlation of sexual dysfunction with prenatal stress and quality of life: a path analysis. Iran Red Crescent Med J. 2017;19:7.
Zubair U, Ali S, Shabana N, Kanwal R. Sexual dysfunction and depression in pregnancy. J Coll Physicians Surg–Pak: JCPSP. 2018;28:495.
Heydarpour S, Feli R, Yazdanbakhsh K, Heydarpour F. The impact of mindfulness-based counseling on the levels of anxiety during pregnancy and on newborns’ physiological parameters. Sci J Nurs, Midwifery Paramedical Fac. 2020;6:106–17.
Moafi F, Dolatian M, Keshavarz Z, Alavi Majd H. Association of depression and preeclampsia. Nurs Midwifery J. 2014;12:297–304.
Sepehrian F, Hosseinpoor L. Female sexual dysfunction and its related factors in Urmia. J Urmia Univ Med Sci. 2012;23:148–54.
Noury R, Karimi N, Mohammadi M. Relationship between prenatal depression with social support and marital satisfaction. Sarem J Reprod Med. 2017;2:153–7.
Arafa AE, Senosy SA. Female sexual dysfunction in Egyptian women with anxiety: prevalence and patterns. J Public Health. 2018;26:545–9.
Johnson SD, Phelps DL, Cottler LB. The association of sexual dysfunction and substance use among a community epidemiological sample. Arch Sex Behav. 2004;33:55–63.
Balon R. Mood, anxiety, and physical illness: body and mind, or mind and body? Depression Anxiety. 2006;23:377–87.
Nezamnia M, Iravani M, Sayyah Bargard M, Latifi M. Effectiveness of cognitive-behavioral therapy on sexual function and sexual self-efficacy in pregnant women: An RCT. Int J Reprod BioMedicine. 2020;18:625–36.
Nejati B, Kazemi F, Masoumi S, Parsa P, Karami M, Mortazavi A. Efficacy of sexual consultation based on PLISSIT model (permission, limited information, specific suggestions, intensive therapy) on sexual function among pregnant women: a randomized controlled clinical trial. J Isfahan Med Sch. 2017;35:739–48.
Estienne MJ, Harper AF, Crawford RJ. Dietary supplementation with a source of omega-3 fatty acids increases sperm number and the duration of ejaculation in boars. Theriogenology. 2008;70:70–6.
Silva T, Jesus M, Cagigal C, Silva C. Food with influence in the sexual and reproductive health. Curr Pharm Biotechnol. 2019;20:114–22.
Ebrahimi FA, Samimi M, Foroozanfard F, Jamilian M, Akbari H, Rahmani E, et al. The effects of omega-3 fatty acids and vitamin E co-supplementation on indices of insulin resistance and hormonal parameters in patients with polycystic ovary syndrome: a randomized, double-blind, placebo-controlled trial. Exp Clin Endocrinol Diabetes. 2017;125:353–9.
Pareek M, Boolchandani R. Effect of Omega–3 Supplementation on Hormone Profile in Women with Poly Cystic Ovarian Syndrome. IJASRM. 2020:5;21:21–6.
Gaskins AJ, Sundaram R, Buck Louis GM, Chavarro JE. Seafood intake, sexual activity, and time to pregnancy. J Clin Endocrinol Metab. 2018;103:2680–8.
Elian M. Is Flaxseed the new wonder food? Preliminary studies show that flaxseed may help fight everything from heart disease and diabetes to breast cancer. [Cited 2009 Des]. Available from: http://www.webmd.com/diet/features/benefits-of-flaxseed.
Innis SM. Dietary omega 3 fatty acids and the developing brain. Brain Res. 2008;1237:35–43.
Sublette ME, Galfalvy HC, Hibbeln JR, Keilp JG, Malone KM, Oquendo MA, et al. Polyunsaturated fatty acid associations with dopaminergic indices in major depressive disorder. Int J Neuropsychopharmacol. 2014;17:383–91.
Olivier B. Serotonin: A never-ending story. Eur J Pharmacol. 2015;753:2–18.
Rees A-M, Austin M-P, Parker GB. Omega-3 fatty acids as a treatment for perinatal depression: randomized double-blind placebo-controlled trial. Aust NZ J Psychiatry. 2008;42:199–205.
Su K-P, Huang S-Y, Chiu T-H, Huang K-C, Huang C-L, Chang H-C, et al. Omega-3 fatty acids for major depressive disorder during pregnancy: results from a randomized, double-blind, placebo-controlled trial. J Clin Psychiatry. 2008;69:644.
Jacka FN, Pasco JA, Williams LJ, Meyer BJ, Digger R, Berk M. Dietary intake of fish and PUFA, and clinical depressive and anxiety disorders in women. Br J Nutr. 2013;109:2059–66.
Álvarez-Ramírez M, Lara MA, Cervantes-Alfaro JM, Robinson-Fuentes VA, Alveano-Hernández J. Correlation between intake of omega-3 fatty acids and depressive and anxiety symptoms during pregnancy. Salud Ment. 2018;41:31–8.
Lazzarin N, Vaquero E, Exacoustos C, Bertonotti E, Romanini ME, Arduini D. Low-dose aspirin and omega-3 fatty acids improve uterine artery blood flow velocity in women with recurrent miscarriage due to impaired uterine perfusion. Fertil Steril. 2009;92:296–300.
Saldeen P, Saldeen T. Women and omega-3 fatty acids. Obstetrical Gynecol Surv. 2004;59:722–30.
Berman J. Physiology of female sexual function and dysfunction. Int J Impot Res. 2005;17:S44–S51.
AO/WHO. WHO: Fats and fatty acids in human nutrition. Report of an expert consultation. Food and Nutrition Paper. Rome: Food and Agriculture Organisation of the United Nations; 2010.
Neijenhuijs KI, Hooghiemstra N, Holtmaat K, Aaronson NK, Groenvold M, Holzner B, et al. The female sexual function index (FSFI)—a systematic review of measurement properties. J Sex Med. 2019;16:640–60.
Jalali-Chimeh F, Gholamrezaei A, Vafa MR, Nasiri M, Abiri B, Darooneh T, et al. Effect of vitamin D therapy on sexual function in women with sexual dysfunction and vitamin D deficiency: a randomized, double-blind, placebo controlled clinical trial. J Urol. 2019;201:987–93.
Foster E, Lee C, Imamura F, Hollidge SE, Westgate KL, Venables MC, et al. Validity and reliability of an online self-report 24-h dietary recall method (Intake24): a doubly labelled water study and repeated-measures analysis. J Nutr Sci. 2019;8:e29-e.
St George SM, Van Horn ML, Lawman HG, Wilson DK. Reliability of 24-hour dietary recalls as a measure of Diet in African-American youth. J Acad Nutr Diet. 2016;116:1551–9.
Taheri M, Irandoust K. The effect of Omega-3 supplementation and functional exercises on the psychomotor performance of aged women in Qazvin. Salmand: Iran J Ageing. 2019;14:2–13.
Taheri M, Irandoust K. The relationship between sleep quality and lifestyle of the elderly. Salmand: Iran J Ageing. 2020;15:188–99.
Barati Z, Iravani M, Karandish M, Haghighizadeh MH, Masihi S. The effect of oat bran consumption on gestational diabetes: a randomized controlled clinical trial. BMC Endocr Disord. 2021;21:1–8.
Huizink AC, Mulder EJ, de Medina PGR, Visser GH, Buitelaar JK. Is pregnancy anxiety a distinctive syndrome? Early Hum Dev. 2004;79:81–91.
Hossein Khanzadeh A, Rostampour A, Khosrojavid M, Nedaee N. Effectiveness of cognitive-behavioral education on anxiety during pregnancy and delivery method in primiparous women. 2. J Nurs Educ. 2017;5:24–32.
Rosen CB J, Heiman S, Leiblum C, Meston R, Shabsigh D, Ferguson R, et al. The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26:191–208.
Fakhri A, Pakpour AH, Burri A, Morshedi H, Zeidi IM. The Female Sexual Function Index: translation and validation of an Iranian version. J Sex Med. 2012;9:514–23.
Jordan RG. Prenatal omega-3 fatty acids: review and recommendations. J Midwifery Women’s Health. 2010;55:520–8.
Zhang Z, Fulgoni VL, Kris-Etherton PM, Mitmesser SH. Dietary intakes of EPA and DHA omega-3 fatty acids among US childbearing-age and pregnant women: an analysis of NHANES 2001–2014. Nutrients. 2018;10:416.
Abbott K, Burrows TL, Acharya S, Thota RN, Garg ML. Dietary supplementation with docosahexaenoic acid rich fish oil increases circulating levels of testosterone in overweight and obese men. Prostaglandins, Leukotrienes Essent Fat Acids. 2020;163:102204.
Rao A, Steels E, Beccaria G, Inder WJ, Vitetta L. Influence of a specialized trigonella foenum-graecum seed extract (Libifem), on testosterone, estradiol and sexual function in healthy menstruating women, a randomised placebo controlled study. Phytother Res. 2015;29:1123–30.
Jarvis C. The effect of omega 3 fatty acids on atrophic vaginitis in breast cancer survivors: the ohio state university; 2012.
Lorenz TK. Interactions between inflammation and female sexual desire and arousal function. Curr Sex Health Rep. 2019;11:287–99.
Giugliano F, Maiorino MI, Di Palo C, Autorino R, De Sio M, Giugliano D, et al. Women’s sexual health: adherence to mediterranean diet and sexual function in women with Type 2 diabetes. J Sex Med. 2010;7:1883–90.
Maiorino MI, Bellastella G, Chiodini P, Romano O, Scappaticcio L, Giugliano D, et al. Primary prevention of sexual dysfunction with Mediterranean diet in type 2 diabetes: the MÈDITA randomized trial. Diabetes Care. 2016;39:e143–e4.
Mutaqin ZZ. Impact of the Covid-19 pandemic on pregnant mother’s anxiety: a systematic review. Sci Midwifery. 2021;10:98–102.
Colli C, Penengo C, Garzitto M, Driul L, Sala A, Degano M, et al. Prenatal stress and psychiatric symptoms during early phases of the COVID-19 pandemic in Italy. Int J Women’s Health. 2021;13:653.
Makrides M, Gibson RA, McPhee AJ, Yelland L, Quinlivan J, Ryan P. Effect of DHA supplementation during pregnancy on maternal depression and neurodevelopment of young children: a randomized controlled trial. Jama. 2010;304:1675–83.
Reed SD, Guthrie KA, Newton KM, Anderson GL, Booth-LaForce C, Caan B, et al. Menopausal quality of life: RCT of yoga, exercise, and omega-3 supplements. Am J Obstet Gynecol. 2014;210:244.e1–11.
Acknowledgements
The authors would like to thank the Deputy of Research of AJUMS, Ahvaz, Iran for providing the opportunity to conduct this study. Hereby, all women who participated in this clinical trial are highly appreciated.
Funding
This article was extracted from a MSc. thesis conducted by Zeinab Khanjari in the Faculty of Nursing and Midwifery, AJUMS, Ahvaz, Iran, and was financially supported by the Deputy of Research at AJUMS, Ahvaz, Iran. This Deputy did not have any role in the design of the study, collection, analysis, and interpretation of the data as well as writing the manuscript. All of the costs of this research have been supplied by Ahvaz University of medical sciences.
Author information
Authors and Affiliations
Contributions
Zkh: responsible for design, data collection and writing manuscript in Persian. MI: responsible for design, data interpretation and writing manuscript in English. PA: involved in design and interpretation of data. SG: responsible for data analyzing and interpretation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was registered in the Iranian Registry of Clinical Trials (Ref. ID: IRCT20200415047087N1) and was also approved by the Ethics Committee of AJUMS (ID: IR.AJUMS.REC.1398.935).
Consent to publish
All participants were assured of confidentiality and anonymity and gave consent for direct quotes from their interviews to be used in this manuscript.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Khanjari, Z., Iravani, M., Abedi, P. et al. Effect of Omega-3 fatty acid supplementation on sexual function of pregnant women: a double blind randomized controlled trial. Int J Impot Res (2022). https://doi.org/10.1038/s41443-022-00598-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41443-022-00598-w
