
Abstract
The aim of this study was to evaluate the clinical outcomes of patients in acute phase of Peyronie’s disease (PD) treated with daily low-dose of Tadalafil. An observational retrospective study involving patients in acute phase of PD with erectile dysfunction (ED) was designed. All subjects were offered Tadalafil 5 mg one tablet a day. Men who accepted treatment were compared to patients who refused Tadalafil. Penile curvature progression was chosen as the primary outcome. PD Questionnaire (PDQ) and IIEF-5 scores were selected as secondary outcomes. A total of 191 patients were included in the study (108 intervention vs. 83 control). Penile curvature progression rate was significantly lower in subjects taking Tadalafil at 12 weeks (25.9% vs. 39.7%, p = 0.042). Mean IIEF-5 score improved in the intervention group, becoming significantly higher compared to the observation group at 12 weeks (19.3 vs. 11.2 points, p < 0.001). Mean PDQ-Overall and PDQ-Penile Pain scores only improved in the intervention group and the statistically significant differences at baseline between groups became not statistically significant at 12 weeks (p = 0.001 vs. p = 0.232 and p < 0.001 vs. p = 0.078, respectively). Daily low-dose Tadalafil in patients with acute phase of PD seems to significantly reduce the penile curvature progression rate compared to observation, especially when it is administrated early. It also appears to improve erectile function and PD-related symptoms.
Similar content being viewed by others


Introduction
Peyronie’s disease (PD) is an acquired disorder involving the connective tissue of the tunica albuginea of the corpora cavernosa characterized by the formation of fibrous plaques that alter penile anatomy [1]. PD consists of two successive phases. The first is an acute inflammatory phase typically, but not invariably, characterized by palpable fibrous plaque, progressive penile curvature and pain during erection. This stage can last up to 12–18 months. The second is a chronic stable phase in which the penile curvature stabilizes, the pain disappears, and the plaque calcifies [2] PD is associated with a high rate of depression [3]. Moreover, a significant proportion of untreated PD patients complain of some degree of erectile dysfunction (ED) [4, 5]. Currently, an etiological therapy for PD is not available. Conservative and surgical treatments can be distinguished [6, 7]. Conservative therapy should be offered to patients in the acute phase and men in the chronic phase who are unwilling or unable to undergo surgery [6]. During the acute phase nonsteroidal anti-inflammatory drugs (NSAIDs) and extracorporeal shockwave treatment (ESWT) may be administrated to relieve penile pain, while the evidence supporting conservative treatments capable of acting on the progression of penile curvature is still limited [6, 8]. Phosphodiesterase 5 inhibitors (PDE5Is) represent a viable option in the treatment of ED [9] Interestingly, some preclinical evidence demonstrated the antifibrotic effects of PDE5Is in PD models [10]. Besides, some preliminary studies highlighted the potential antifibrotic and analgesic effects of PDE5Is in men with PD [11, 12]. Accordingly, long-term treatment with PDE5Is could represent an emerging strategy for conservative treatment of PD [13]. However, current European Association of Urology (EAU) Guidelines still recommend the use of PDE5Is only to improve the erectile function of PD patients [6]. In fact, although the use of these drugs in patients with PD is progressively increasing, there is still little clinical evidence demonstrating their effectiveness in reducing symptoms and disease progression [14].
The aim of this study was to evaluate the clinical outcomes of patients in acute phase of PD treated with daily low-dose of Tadalafil.
Materials and methods
Study design and ethical aspects
We designed an observational retrospective study involving consecutive patients referring to the outpatient clinic of our tertiary center (Urology Unit, University of Naples “Federico II”, Naples, Italy) from September 2018 to March 2020. The research was conducted in accordance with the Declaration of Helsinki on ethical principles for medical research involving human subjects [15]. All patients gave a written informed consent for collection and publication of their clinical data. Due to purely observational retrospective nature of the study, after consultation with the Ethics Committee it was exempted from specific approval.
Patient enrollment and treatment protocol
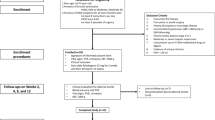
Male patients, over 18 years old, in acute phase of PD, with a penile curvature <30 degrees, complaining of ED were included in the study. Acute phase of PD was defined as progressive worsening of penile curvature associated with penile pain during erection, regardless of the time from the onset of symptoms. ED was defined as five-item version of International Index of Erectile Function (IIEF-5) score <22 [16]. All patients were sexually active (at least 1 sexual intercourse per month in the past 3 months) and had a stable partner (single sexual partner in the past 3 months). The followings were considered exclusion criteria: previous treatments specifically targeted to PD, previous daily use of PED5Is or intracavernous vasoactive agents for ED, concomitant penile disorders, complex penile deformities (hinge or hourglass), history of pelvic surgery or radiotherapy. Intake of nitrates, severe heart diseases, non-arteritic anterior ischemic optic neuropathy, and other conditions that contraindicated the intake of PDE5Is were further reasons for exclusion.
All patients who met the above criteria were offered Tadalafil 5 mg one tablet a day at the same time regardless of meals for 12 weeks. Men who accepted treatment (intervention group) were compared to patients who refused PDE5Is for personal reasons (observational group). More specifically, PDEIs were refused mainly due to the fear of side effects or interactions (44.6%), the embarrassment in purchasing or using the drug (27.7%), and the fear of drug addiction (12.0%). Patients in both groups underwent no other conservative treatment for PD (including supplements, NSAIDs, ESWT, and penile traction therapy) or on demand PDE5Is for ED. Only subjects with a complete 12-week follow-up and who did not discontinue Tadalafil treatment were included in the analysis.
Patient evaluation and selected outcomes
The following data were collected for each patient at baseline: age, body mass index (BMI), diabetes mellitus, smoking, hypertension, dyslipidemia, total serum testosterone, time from onset of symptoms, plaque features, penile curvature, PD Questionnaire (PDQ) [17], and IIEF-5.
Penile curvature assessment was performed by a single experienced urologist following intracavernous injection of 10 micrograms of alprostadil and using a goniometer. Only patients who achieved sufficient erection (Erection Hardness Score: 3–4) [18] with this injection were included. The study of penile plaques was performed with ultrasonography. IIEF-5 and PDQ were self-administrated to patients.
Penile curvature, PDQ, and IIEF-5 were reassessed after 12 weeks in both groups. Penile curvature progression was chosen as the primary outcome and was arbitrarily defined as worsening of curvature after 12 weeks ≥10 degrees. In the case of multiplanar penile curvatures, the greater one was taken into account. PDQ and IIEF-5 scores were selected as secondary outcomes. All adverse events (AEs) were recorded in the follow-up period.
Statistics
The categorical variables were described as frequencies and percentages. The continuous variables were expressed as mean ± standard deviation (SD). The Kolmogorov–Smirnov test was applied as normality test [19]. The Student’s t test and the Chi-squared test were used to compare continuous and categorical variables, respectively [20]. Statistical significance was set a priori at p ≤ 0.05. A sub-analysis was performed according to the duration of the disease based on an arbitrary cut-off (≤9 months vs. >9 months). The IBM Statistical Package for the Social Sciences (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.) was used for the statistical analyses.
Results
A total of 191 patients were included in the study, 108 received Tadalafil and 83 underwent observation. Mean (SD) age was 59.0 (9.0) years in the intervention group and 57.7 (9.2) years in the observation group (p = 0.442). Mean (SD) time from onset of PD was 9.8 (5.5) and 10.9 (6.7) months (p = 0.232), for the intervention and observation group, respectively. Most penile curvatures were dorsal in both groups (46.2% vs. 48.2%). Mean (SD) penile curvature at baseline was 19.0 (7.8) degrees in patients treated with Tadalafil and 18.0 (7.5) degrees in controls (p = 0.265). Baseline demographic and clinical characteristics of both groups were detailed in Table 1.
Penile curvature progression rate was significantly lower in subjects taking Tadalafil than men under observation at 12 weeks (25.9% vs. 39.7%, p = 0.042). This statistically significant difference was maintained in patients with a time from onset of PD ≤ 9 months (p = 0.003), in contrast to the subgroup characterized by time from onset >9 months (p = 0.059). Penile curvature angle and progression rate according to treatment and duration of disease were reported in Table 2 and Fig. 1, respectively.

Progression was defined as worsening of curvature after 12 weeks ≥10 degrees. PD: Peyronie’s Disease.
Mean IIEF-5 score significantly improved (p = 0.001) in the intervention group, becoming significantly higher compared to the observation group at 12 weeks (19.3 vs. 11.2 points, p < 0.001). IIEF-5 score was described in Table 3. Mean PDQ-Overall and PDQ-Penile Pain (PDQ-PP) scores significantly improved (p < 0.001) at 12 weeks only in the intervention group, consequently the statistically significant differences in favor of the observation group at baseline became not significant at 12 weeks (p = 0.001 vs. p = 0.232 and p < 0.001 vs. p = 0.078, respectively). PDQ-Overall and PDQ-PP scores were summarized in Table 4.
Only mild AEs (e.g., headache, flushing, dyspepsia, nasal congestion) were recorded in a minority of cases (19, 17.6%) belonging to the Tadalafil group.
Discussion
A conservative therapy is frequently advocated in the acute phase of PD to relieve the penile pain or prevent the progression of penile curvature, but the evidence on the topic is still limited [21]. PDE5Is are part of the conservative management of patients with PD, however, they are traditionally used to improve erection in this population [22]. In recent years, preliminary evidence, first in animal models and in vitro and subsequently in humans, have highlighted the antifibrotic and analgesic potential of long-term administration of PDE5Is in PD [12, 23, 24].
Clinical evidence on PDE5Is in PD patients
A recent survey of 401 sexual medicine experts across Europe found that the most common oral medication prescribed for the treatment of PD was Tadalafil 5 mg once daily (57.4%) [13]. Palmieri et al. showed in a randomized controlled trial (RCT) on PD patients complaining of ED that ESWT plus Tadalafil 5 mg once daily significantly improved IIEF-5 and quality of life compared to ESWT alone at 6 months [25]. Dell’Atti compared intralesional verapamil injection (IVI), Tadalafil 5 mg daily, and IVI plus Tadalafil 5 mg daily in a 3-month RCT on PD patients. Penile pain resolved completely or partially in 57%, 61%, and 76% of cases, respectively. A slight reduction in penile curvature was recorded in all groups with no significant differences compared to baseline. Plaque size remained stable in IVI alone and Tadalafil alone groups, significantly decreasing in the combination group. IIEF-5 significantly improved in Tadalafil alone and combination groups, with a statistically significant difference in favor of the latter [26]. Hatampour et al. compared intraplaque injection of dexamethasone plus Tadalafil 5 mg once daily and IVI in another 3-month RCT on chordee patients with PD. Degree of penile curvature, plaque count, and plaque size decreased significantly in both groups from baseline, with no significant difference between the groups [27]. Chung et al. evaluated PD patients with septal scars undergoing Tadalafil 2.5 mg daily over a 6-month period in a retrospective controlled study. The Tadalafil group reported a significantly higher IIEF-5 score and significantly more frequent septal scar resolution than the control group. Besides, 5 patients in the control group and only 1 subject in the Tadalafil group showed worsening or penile curvature during the follow-up [11]. Ozturk et al. compared Sildenafil 50 mg daily and Vitamin E 400 IU daily in a RCT with 3 months of follow-up. IIEF-5, penile curvature, plaque volume, and pain score were significantly improved from baseline in the Sildenafil group. Moreover, the improvements in IIEF-5 score and pain score were statistically significant in Sildenafil group compared with Vitamin E group [12].
Molecular mechanisms of PDE5Is in PD
Several studies on fibrosing diseases (e.g., idiopathic pulmonary fibrosis, Duchenne muscular dystrophy, cardiac and renal fibrosis) showed that PDE5Is have antifibrotic properties [28]. Growing evidence is showing that continuous therapy with PDE5Is may block or reverse fibrosis of the corpora cavernosa and tunica albuginea, with antifibrotic mechanisms independent of the well-known effect of vasodilation and increased blood flow associated with these drugs. Continuous PDE5Is administration induces a sustained elevation of nitric oxide (NO) and cyclic guanosine monophosphate (cGMP) in the penile tissues. This pathway, probably by activating protein kinase G, leads to decrease profibrotic factor secretion (e.g., TGF-β1), myofibroblasts count, and collagen deposition [10]. Myofibroblasts are “the most intensive collagen factory”. Oxidative stress and inflammation typical of the acute phase of PD promote local fibroblast-to-myofibroblast conversion. Sustained levels of NO and cGMP seems hinder this differentiation and promote myofibroblast apoptosis. The timing for the administration of PDE5Is could be essential, a recent study suggests that these drugs can prevent but not reverse myofibroblast transformation, therefore, they should only be used in the early stage of PD for antifibrotic purposes [29]. However, the antifibrotic mechanisms of PDE5Is in the penile tissues are probably still largely unknown and some of them could be partially or totally independent from the NO/cGMP pathway. Finally, we hypothesize that an anti-inflammatory and antioxidant effect of continuous PDE5Is may contribute to the reduction of penile pain in patients with PD, however this statement is not currently supported by solid biomolecular evidence [23, 24, 30].
Our main findings
In this study we compared the clinical outcomes of PD patients receiving Tadalafil 5 mg daily or observation. Interestingly, we found that the penile curvature progression rate was significantly lower in patients taking Tadalafil than men under observation (p = 0.042). This finding supports the hypothesis that PDE5Is may interfere with the pathogenesis of fibrosis in PD patients [31]. Moreover, the difference between the two groups was significant (p = 0.002) only when considering patients with short duration of the disease (≤9 months). This result suggests a substantial benefit especially when therapy with PDE5Is is started early.
Furthermore, in patients receiving Tadalafil we observed a predictable significant improvement in the IIEF-5 score and statistically significant higher scores compared to subjects in the observation group. This finding aligns with the recommendation of the EAU guidelines to offer PDE5Is to PD patients to improve erection and optimize penetration [6].
Finally, we found a significant improvement in the PDQ-Overall and PDQ-PP scores of men treated with Tadalafil and stable scores in observed patients. Consequently, despite a statistically significant difference at baseline in favor of the observation group, no statistically significant differences were recorded between the two groups at 12 weeks. This result supports previous evidence on the analgesic effect of PDE5Is in PD patients [12].
Strengths and limitations
To the best of our knowledge this is the first study specifically designed to evaluate the clinical outcomes of patients in acute phase of PD treated with Tadalafil 5 mg daily alone. Furthermore, despite the relatively small sample size, this is to date the clinical study on the topic with the largest cohort of patients evaluated. Other significant strengths of this paper are the presence of a comparative group and the use of a validated tool (PDQ) for measuring outcomes of PD patients. However, our research should be read and interpreted considering various issues. The main limitation is the retrospective design. Another weakness, caused by the lack of randomization, is the presence of some significant differences at baseline between the intervention and observation group. In this regard, the placement of patients in one group over the other depending on their choice of whether or not to take Tadalafil it may have favored the selection bias. Some subjects may have refused daily Tadalafil because they were dissatisfied with the effect of PDE5Is taken sporadically for DE before the study period, this could be a sign of an overall lower efficacy of this class of drugs in a part of the observation group with consequent impact on the results; however, we do not know the exact percentage of patients who refused Tadalafil for this reason and the lower efficacy in this small subgroup remains only a hypothesis. We did not perform an a priori power analysis. There is no univocal definition of penile curvature progression, therefore it was decided arbitrarily, this may have influenced the direction of the results. The assessment of plaques with ultrasonography is not a reliable method and it is not recommended by the guidelines [6]. The IIEF-5 and PDQ questionnaires have not yet been validated in Italian. The course of PD is unpredictable and especially for patients with time from onset >9 months the improvement in clinical outcomes could be due in part to spontaneous disease stabilization rather than PDE5Is [31]. Only men with penile pain and progressive worsening of the penile curvature were included in the study, but it is known that a significant proportion of subjects in the acute phase of PD may have no pain or progression of the curvature [32]. In addition, the selected patients had overall a mild penile curvature and all complained of ED. Finally, only men who had not discontinued Tadalafil treatment were included, although it is known that not negligible percentage of patients treated with PDE5Is may discontinue therapy for various reasons [20, 33]. These last three issues could hinder the generalizability of our results.
Conclusions
Daily low-dose Tadalafil in patients with acute phase of PD seems to significantly reduce the penile curvature progression rate compared to observation, especially when it is administrated early. Besides, it appears to improve erectile function and PD-related symptoms. However, the results of the present study should be considered preliminary due to its significant limitations. Further well-designed RCTs are needed to confirm our promising findings.
Data availability
Raw data is available if requested.
References
Miner MM, Seftel AD. Peyronie’s disease: epidemiology, diagnosis, and management. Curr Med Res Opin. 2014;30:113–20.
Piraino J, Chaudhary H, Ames K, Okoye F 3rd, Sterling M, Clavell-Hernandez J, et al. A consistent lack of consistency in defining the acute and chronic phases of Peyronie’s disease: a review of the contemporary literature. Sex Med Rev. 2022;10:698–713.
Punjani N, Nascimento B, Salter C, Miranda E, Terrier J, Taniguchi H, et al. Predictors of Depression in Men With Peyronie’s Disease Seeking Evaluation. J Sex Med. 2021;18:783–8.
Mulhall JP, Schiff J, Guhring P. An Analysis of the Natural History of Peyronie’s Disease. J Urol. 2006;175:2115–8.
Weidner W, Schroeder-Printzen I, Weiske WH, Vosshenrich R. Sexual Dysfunction in Peyronie’s Disease: An Analysis of 222 Patients Without Previous Local Plaque Therapy. J Urol. 1997;157:325–8.
Salonia A, Bettocchi C, Boeri L, Capogrosso P, Carvalho J, Cilesiz NC, et al. European Association of Urology Guidelines on Sexual and Reproductive Health—2021 Update: Male Sexual Dysfunction. Eur Urol. 2021;80:333–57.
Fernández-Pascual E, Manfredi C, Cocci A, Quintana Franco LM, Egui Rojo MA, Carballido Rodríguez J, et al. A Novel Penile Splint as Early Traction Therapy After Grafting Techniques for Peyronie’s Disease. J Sex Med. 2020;17:1819–24.
Manfredi C, Arcaniolo D, Amicuzi U, Spirito L, Napolitano L, Crocerossa F, et al. Impact of extracorporeal shockwave therapy for erectile dysfunction and Peyronie’s disease on reproductive and hormonal testicular function. Andrology. 2022; https://doi.org/10.1111/andr.13240.
Ferguson JE 3rd, Carson CC 3rd. Phosphodiesterase type 5 inhibitors as a treatment for erectile dysfunction: Current information and new horizons. Arab J Urol. 2013;11:222–9.
Gonzalez-Cadavid NF, Rajfer J. Laboratory Forum: Experimental Models of Peyronie’s Disease. Implications for New Therapies. J Sex Med. 2009;6:303–13.
Chung E, DeYoung L, Brock GB. The Role of PDE5 Inhibitors in Penile Septal Scar Remodeling: Assessment of Clinical and Radiological Outcomes. J Sex Med. 2011;8:1472–7.
Ozturk U, Yesil S, Goktug HNG, Gucuk A, Tuygun C, Sener NC, et al. Effects of sildena fil treatment on patients with Peyronie’s disease and erectile dysfunction. Ir J Med Sci. 2014;183:449–53.
Porst H, Burri A. Current Strategies in the Management of Peyronie’s Disease (PD)—Results of a Survey of 401 Sexual Medicine Experts Across Europe. J Sex Med. 2019;16:901–8.
Teloken K. Medical Management of Peyronie’s Disease: Review of the Clinical Evidence. Med Sci. 2019;7:96.
World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA.2013;310:2191.
Rhoden EL, Telöken C, Sogari PR, Vargas Souto CA. The use of the simplified International Index of Erectile Function (IIEF-5) as a diagnostic tool to study the prevalence of erectile dysfunction. Int J Impot Res. 2002;14:245–50.
Hellstrom WJ, Feldman R, Rosen RC, Smith T, Kaufman G, Tursi J. Bother and distress associated with Peyronie’s disease: validation of the Peyronie’s disease questionnaire. J Urol. 2013;190:627–34.
Mulhall JP, Goldstein I, Bushmakin AG, Cappelleri JC, Hvidsten K. Validation of the erection hardness score. J Sex Med. 2007;4:1626–34.
Aslam M. Introducing Kolmogorov–Smirnov Tests under Uncertainty: An Application to Radioactive Data. ACS Omega. 2020;5:914–7.
Kim HY. Statistical notes for clinical researchers: Chi-squared test and Fisher’s exact test. Restor Dent Endod. 2017;42:152.
Vardi Y, Levine LA, Chen J, Hatzimouratidis K, Sohn M. Is there a place for conservative treatment in Peyronie’s disease? J Sex Med. 2009;6:903–9.
Levine LA, Latchamsetty KC. Treatment of erectile dysfunction in patients with Peyronie’s disease using sildenafil citrate. Int J Impot Res. 2002;14:478–82.
Ferrini MG, Vernet D, Magee TR, Shahed A, Qian A, Rajfer J, et al. Antifibrotic Role of Inducible Nitric Oxide Synthase. Nitric Oxide. 2002;6:283–94.
Valente EGA, Vernet D, Ferrini MG, Qian A, Rajfer J, Gonzalez-Cadavid NF. l-Arginine and phosphodiesterase (PDE) inhibitors counteract fibrosis in the Peyronie’s fibrotic plaque and related fibroblast cultures. Nitric Oxide. 2003;9:229–44.
Palmieri A, Imbimbo C, Creta M, Verze P, Fusco F, Mirone V. Tadalafil once daily and extracorporeal shock wave therapy in the management of patients with Peyronie’s disease and erectile dysfunction: results from a prospective randomized trial: ESWT and Tadalafil in PD patients. Int J Androl. 2012;35:190–5.
Dell′Atti L. Tadalafil once daily and intralesional verapamil injection: A new therapeutic direction in Peyronie′s disease. Urol Ann. 2015;7:345.
Hatampour M, Sohrabi K, Mazdak H, Ghadimi K, Salehi H, Kazemi R. Evaluating the efficacy of intraplaque injection of dexamethasone with oral tadalafil in the chordee patients with Peyronie disease. Am J Clin Exp Urol. 2022;10:25–30.
Gong W, Yan M, Chen J, Chaugai S, Chen C, Wang D. Chronic inhibition of cyclic guanosine monophosphate-specific phosphodiesterase 5 prevented cardiac fibrosis through inhibition of transforming growth factor β-induced Smad signaling. Front Med. 2014;8:445–55.
Ilg MM, Stafford SJ, Mateus M, Bustin SA, Carpenter MJ, Muneer A, et al. Phosphodiesterase Type 5 Inhibitors and Selective Estrogen Receptor Modulators Can Prevent But Not Reverse Myofibroblast Transformation in Peyronie’s Disease. J Sex Med. 2020;17:1848–64.
Gonzalez-Cadavid NF, Rajfer J. The two phases of the clinical validation of preclinical translational mechanistic research on PDE5 inhibitors since Viagra’s advent. A personal perspective. Int J Impot Res. 2019;31:57–60.
Garaffa G, Trost LW, Serefoglu EC, Ralph D, Hellstrom WJG. Understanding the course of Peyronie’s disease. Int J Clin Pr. 2013;67:781–8.
Pryor JP, Ralph DJ. Clinical presentations of Peyronie’s disease. Int J Impot Res. 2002;14:414–7.
Verze P, Capece M, Creta M, La Rocca R, Persico F, Spirito L, et al. Efficacy and safety of low-intensity shockwave therapy plus tadalafil 5 mg once daily in men with type 2 diabetes mellitus and erectile dysfunction: a matched-pair comparison study. Asian J Androl. 2020;22:379.
Author information
Authors and Affiliations
Contributions
Conceptualization: LS, CM; Data Collection: RLR, LN, ADA, MC; Data analysis: FT, CS; Writing-original draft: LS, CM; Scientific review: IS; Supervision: MC, DA.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Spirito, L., Manfredi, C., La Rocca, R. et al. Daily low-dose tadalafil may reduce the penile curvature progression rate in patients with acute Peyronie’s disease: a retrospective comparative analysis. Int J Impot Res 36, 129–134 (2024). https://doi.org/10.1038/s41443-022-00651-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41443-022-00651-8
This article is cited by
-
Response to: “Commentary on: phosphodiesterase type 5 inhibitors do not prevent curvature progression but shorten pain duration in the active phase of Peyronie’s disease: a retrospective cohort study”
International Journal of Impotence Research (2024)
-
Is there a new role for oral therapy to treat peyronie’s disease? Commentary on Daily low-dose tadalafil may reduce the penile curvature progression rate in patients with acute Peyronie’s Disease: a retrospective comparative analysis
International Journal of Impotence Research (2024)
-
Phosphodiesterase type 5 inhibitors do not prevent curvature progression but shorten pain duration in the active phase of Peyronie’s Disease: A retrospective cohort study
International Journal of Impotence Research (2024)
-
Unveiling treatment horizons and contemporary perspectives in Peyronie’s disease – take home messages from Laurance A. Levine special issue
International Journal of Impotence Research (2024)
-
Long-term outcomes of extracorporeal shock wave therapy for acute Peyronie’s disease: a 10-year retrospective analysis
International Journal of Impotence Research (2024)
