
Abstract
Small cell lung cancer (SCLC) is an exceptionally lethal malignancy for which more effective therapies are urgently needed. Several lines of evidence, from SCLC primary human tumours, patient-derived xenografts, cancer cell lines and genetically engineered mouse models, appear to be converging on a new model of SCLC subtypes defined by differential expression of four key transcription regulators: achaete-scute homologue 1 (ASCL1; also known as ASH1), neurogenic differentiation factor 1 (NeuroD1), yes-associated protein 1 (YAP1) and POU class 2 homeobox 3 (POU2F3). In this Perspectives article, we review and synthesize these recent lines of evidence and propose a working nomenclature for SCLC subtypes defined by relative expression of these four factors. Defining the unique therapeutic vulnerabilities of these subtypes of SCLC should help to focus and accelerate therapeutic research, leading to rationally targeted approaches that may ultimately improve clinical outcomes for patients with this disease.
Similar content being viewed by others

Introduction
Small cell lung cancer (SCLC) is a particularly aggressive and deadly form of lung cancer characterized by a predilection for rapid growth, early metastasis and acquired therapeutic resistance1,2. In the majority of cases, SCLC has metastasized to sites outside the chest at the time of initial diagnosis. Although a small minority of patients with localized early-stage disease can be cured with surgery or concomitant cytotoxic chemotherapy and radiation, the large majority of patients diagnosed with SCLC are destined to die of their disease. The standard chemotherapy regimen for SCLC, consisting of a platinum agent (cisplatin or carboplatin) combined with etoposide, was defined several decades ago3. Recent incorporation of the anti-PDL1 antibody atezolizumab into first-line therapy for advanced SCLC has improved median survival from 10.3 to 12.3 months, but only 12.6% of patients remain progression-free at 1 year3,4. Two therapies are approved by the US Food and Drug Administration (FDA) for recurrent SCLC: topotecan, a topoisomerase I poison approved for second-line use, has substantial toxicities and produces transient responses in approximately 25% of patients5, and nivolumab, a PD1 antagonist approved for third-line use that can provide durable benefit in less than 15% of patients6. Clearly, more effective therapies are needed for patients with SCLC.
The notably minimal armamentarium of molecularly targeted drugs for SCLC stands in sharp contrast to the remarkable progress that has been made in identifying and selectively targeting driver oncogenes in lung adenocarcinoma7. Underpinning this progress has been a better understanding of the biology of lung adenocarcinoma, and in particular a recognition of mutually exclusive subtypes of disease defined by mutant or translocated oncogenic drivers. There are now multiple highly effective targeted inhibitors available with impressive activity against tumour-specific somatic mutant forms of EGFR, ALK, ROS1, RET, BRAF, MET, NTRK and other driver oncogenes. Unlike the increasingly personalized approach to clinical care of patients with lung adenocarcinoma, SCLC is approached clinically as a single disease entity. Current clinical research protocols for SCLC, representing the cutting edge of clinical care, are generally constructed on the basis of stage of disease, and in some cases number of prior therapies, with no attempt to predefine specific patient populations that might be most amenable to the novel treatment being tested.
We believe it is time to revise this approach to therapeutic research in SCLC. Studies by our research groups and others over the past decade have begun to identify and characterize biologically distinct subtypes of SCLC. Complementary data from human tumours, cell lines and mouse models of SCLC have implicated the same predominant subtypes and some of the same subtype-specific therapeutic vulnerabilities. Our teams have historically approached the subclassification of SCLC in different ways using different terminology. In this Perspectives article, we review recent progress towards a classification of SCLC tumours based on differential expression of transcription regulators and propose a consensus nomenclature for molecular subtypes of SCLC. This is an evolving area of investigation, and further refinement or improvement of the proposed classification scheme is likely to be needed. Nonetheless, we believe that this is an opportune time to review the existing data and that having a common understanding of the major subtypes will provide a framework for focused progress in the field.
Histological categorization
The essential histological characteristics used by pathologists to establish a diagnosis of SCLC have been described elsewhere and are summarized in Box 1. Our goal in this Perspectives article is not to revise the pathological definition of the disease but rather to emphasize commonalities among mouse and human gene expression data, emerging from our research groups and others, suggesting biologically distinct subtypes of disease.
Many of the existing SCLC cell lines were generated from human tumours by research teams led by two of the authors (J.D.M. and A.F.G.) working at the US National Cancer Institute–Navy Medical Oncology Branch in the late 1970s and 1980s8,9. Analysis of the morphological characteristics of 50 SCLC lines suggested that these could be grouped into two primary subtypes: a more common ‘classic’ subtype, which grew predominantly as spherical aggregates of floating cells, with or without central necrosis; and a ‘variant’ subtype, which grew as either loosely adherent aggregates or as a more tightly adherent monolayer in cell culture10. These subtypes were also noted to differ in expression of neuroendocrine markers, including l-DOPA decarboxylase and neuron-specific enolase; both proteins were expressed in most classic and absent or low in most variant cell lines, suggesting a loss of neuroendocrine features in variant cell lines10. These characteristics were also noted in primary SCLC tumours from patients, including autopsy specimens10.
‘Omic’ profiling
Genomics
Key genomic profiling studies of human SCLC, including comprehensive whole-exome and whole-genome analyses, were published in 2012 and 2015 (refs11,12,13); the key findings of these are summarized in Box 2. Although characterizing for the first time the global landscape of SCLC genomic alterations, these sequencing efforts did not lead to a classification of SCLC subtypes, in part because specific recurrent mutations do not demonstrate consistent co-occurrence or mutual exclusivity. The relative genetic homogeneity of SCLC, notable for nearly universal inactivation of TP53 (which encodes p53) and RB1 (which encodes RB), did not substantially influence the prevailing model of SCLC as a single, monolithic entity.
Epigenetics and transcriptomics
By contrast, epigenetic and gene expression studies have revealed a new and previously unappreciated molecular diversity among SCLC cell lines and primary tumours. A first clue for possible drivers of discrete subtypes of SCLC emerged from an analysis of a panel of cell lines for susceptibility to an oncolytic picornavirus, called Seneca Valley virus (SVV), that had selective tropism for a subtype of SCLC14. Susceptibility to SVV infection proved to be closely correlated with variant versus classic morphology. Gene expression profiling of these lines demonstrated an even tighter correlation between susceptibility to infection and the relative expression of two lineage transcription factors, achaete-scute homologue 1 (ASCL1; also known as ASH1) and neurogenic differentiation factor 1 (NeuroD1), each of which had been previously implicated as a key determinant of developmental maturation of neuroendocrine cells of the lung15,16,17. Notably, ASCL1 was observed to be expressed to a variable extent in NeuroD1-high SCLC, but a low ratio of ASCL1 to NEUROD1 was a strong correlate of permissivity14.
This initial dichotomy between classic SCLC, demonstrating a high ASCL1:NeuroD1 ratio, and variant SCLC, demonstrating the converse, was further reinforced in primary SCLC tumours and patient-derived xenograft (PDX) models through profiling of genome-wide methylation and gene expression patterns18. Consensus clustering of either the SCLC methylome or RNA sequencing (RNA-seq) in primary human SCLC was consistent with at most four subtypes. The highest confidence model considered three clusters, with the largest (referred to as M1 in the methylation data and E1 in the expression data) representing the ASCL1-high/NeuroD1-low subtype and the second largest (M2, or E2) representing the NeuroD1-high subtype. Interestingly, a small number of primary tumours with highly divergent methylation and gene expression patterns were identified that expressed low levels of both ASCL1 and NeuroD1. Because of similarity in the gene expression pattern to a previously identified subpopulation in the gene expression profiling of lung squamous cell carcinomas by The Cancer Genome Atlas (TCGA)19, this population lacking neuroendocrine markers was labelled SQ-P to indicate its similarity to primitive squamous cell tumours. Pathological review of these cases, however, confirms that these are SCLC, not squamous tumours. Similar subtypes were observed in a large-scale gene expression survey of SCLC that delineated two groups: a dominant group of samples termed group2, characterized by high expression of chromogranin A (CHGA; also known as CgA), gastrin-releasing peptide (GRP), ASCL1 and protein delta homologue 1 (DLK1) (and thought to represent tumours with low activity of the Notch signalling pathway), and a minority of samples that lacked these markers termed group1 (ref.13).
Several recent studies of human tumours and cell lines have provided biological insights into the roles of ASCL1 and NeuroD1 and identified other relevant factors contributing to subtype definition. A high-throughput chemical screen of SCLC cell lines identified super-enhancer-mediated transcriptional addiction to MYC family proto-oncogenes as well as neurogenic transcription factors including ASCL1, NeuroD1 and insulinoma-associated protein 1 (INSM1)20. INSM1 is a zinc-finger transcription factor implicated as a driver of neuroendocrine differentiation in multiple tissues21,22,23,24. A broader analysis of the relative roles of ASCL1 and NeuroD1 in human SCLC cell lines confirmed and deepened our understanding of their roles, identifying several target genes differentially regulated by these transcription factors and implicated in SCLC biology25. Among others, these include for ASCL1 MYCL1 (also known as MYCL), BCL2, SOX2 and DLL3 and for NeuroD1 MYC as well as common targets INSM1 and HES6, an inhibitor of the HES1 transcription factor and of Notch-mediated repression of ASCL1 transcriptional activity26. Several of these downstream genes were found to be direct targets of ASCL1 or NeuroD1, respectively, by chromatin immunoprecipitation. ASCL1 and NeuroD1 appear to bind to and activate largely non-overlapping super-enhancers in discrete subtypes of SCLC, resulting in substantial differences in gene expression and supporting the idea that ASCL1-high and NeuroD1-high tumours represent distinct subtypes. Preliminary systems-level analyses of transcriptomic data from human and mouse SCLC cell lines and tumours identified gene expression programmes and biological ontologies that suggested further subdivision of ASCL1-high tumours into two discrete subsets, termed NE and NEv2 (ref.27).
Engineered mouse models
The first genetically engineered mouse model (GEMM) of SCLC was created in the laboratory of Anton Berns by introducing alleles of the Trp53 and Rb1 tumour suppressor genes in which key exons were flanked by loxP sites (‘floxed’ alleles)28. Intratracheal delivery of adenovirus expressing the CRE recombinase resulted in inactivation of both genes in cells in the respiratory epithelium of mice. After a several months delay following targeted disruption of Trp53 and Rb1, these mice developed tumours highly similar to human SCLC. Interestingly, and of potential relevance to consideration of SCLC subtypes, the use of adenoviruses with cell-type-specific promoters in this model suggested that SCLC tumours may arise from at least two different cells of origin: efficient tumorigenesis resulted from targeting of lung epithelial cells through use of the neuroendocrine-specific CALCA gene promoter (the CALCA gene encodes calcitonin gene-related peptide 1 (CGRP1)), and much less efficient tumorigenesis was observed when an SFTPC gene promoter was used (the SFTPC encodes pulmonary surfactant-associated protein C (SP-C), expressed at high levels in alveolar type 2 cells)29. How these differences in cell of origin may parallel distinct subtypes of human SCLC, what the relevant SP-C-expressing cell of origin might be and whether this observation could also be attributable to leaky expression in a cell type not normally expressing SP-C have not been further clarified, but these different cells of origin may influence the transcriptional programmes in the resulting SCLC tumours in mice30.
The original Berns GEMM was modified to incorporate a third floxed locus, Rbl2 (also known as p130), a paralogue of Rb1 (the human homologue of Rbl2 is inactivated in 5–10% of human SCLC)31. This conditional triple knockout Trp53/Rb1/Rbl2 model demonstrates accelerated tumorigenesis, phenotypically resembles the Trp53/Rb1 conditional double knockout and retains many of the characteristic features of human SCLC. Gene expression patterns of both Trp53/Rb1 and Trp53/Rb1/Rbl2 conditional knockout models appear to most resemble the ASCL1-high/NeuroD1-low subtype of human SCLC32.
The Trp53/Rb1/Rbl2 conditional knockout GEMM was subsequently used to interrogate the relative requirements of ASCL1 and NeuroD1 in SCLC oncogenesis by introducing additional loxP sites flanking key regions of the genes encoding each of these two transcription factors25. Strikingly, inactivation of Ascl1 appeared to completely abrogate neuroendocrine tumour formation when assessed approximately 6 months after adenoviral CRE exposure, whereas inactivation of Neurod1 had no evident impact on the number, size or histological appearance of resulting tumours. This result provided strong evidence for an essential role of ASCL1 in SCLC oncogenesis and further suggested that the existing mouse models of SCLC, both conditional double and triple knockouts, were largely reflective of the ASCL1-high/NeuroD1-low subtype of human SCLC.
A mouse model resulting in tumours representative of the NeuroD1-high subtype of SCLC was reported in 2017 (ref.32). This model explored the role of Myc, the expression of which had been previously noted to be associated with the variant subtype of human SCLC, as a driver of SCLC oncogenesis33. This model is based on the backbone of the Trp53/Rb1 conditional knockout mouse, with introduction of a CRE-activated MycT58A mutant that leads to stabilization of the resultant MYC protein. Stabilization of MYC markedly accelerated tumour initiation and growth. Initial tumour formation in this model appeared to reflect an ASCL1-high/NeuroD1-low state; however, invasive tumours demonstrated a NeuroD1-high/ASCL1-low state, resembling the NeuroD1-high variant subtype of human SCLC.
Together, these data suggested that MYC family members may serve as key differential drivers of SCLC subtypes, with MYCL1 being predominant in ASCL1-high classic SCLC and MYC being predominant in NeuroD1-high variant SCLC. These data also suggested that in mouse models of SCLC there may be sequential hierarchy between subtypes, with ASCL1 implicated as a driver in initial oncogenesis and NeuroD1-high tumours differentiating from or being selected from ASCL1-high precursors. Notably, whether ASCL1 is required for tumour formation in the model with Trp53/Rb1 conditional knockout and MycT58A expression (referred to hereafter as the Trp53−/−;Rb1−/−;MycT58A GEMM) has not yet been reported, definitive lineage tracing experiments have not been performed and the extent to which the hierarchical model suggested by these GEMMs is applicable to human tumour development has also not been demonstrated.
Non-neuroendocrine SCLC
Recent data are also beginning to clarify transcriptional drivers relevant in the subtype of tumours with low-level expression of both ASCL1 and NeuroD1. Expression profiling of a large panel of human SCLC identified differential expression of INSM1, encoding a transcription factor expressed preferentially in both ASCL1-high and NeuroD1-high SCLC subtypes relative to non-neuroendocrine, and YAP1, a regulator of transcription activated by the HIPPO growth signalling pathway, having the opposite profile — high in non-neuroendocrine but undetectable or low in most SCLC lines in the ASCL1-high or NeuroD1-high subtypes34. Examples of YAP1-high tumours were also noted in the previous RNA-seq data from primary human SCLC13. Intriguingly, the small YAP1-high subtype of SCLC cell lines appeared to be enriched for intact RB by immunohistochemistry, a rare event in SCLC34. Notably, and in contrast to data supporting driver roles for ASCL1, NeuroD1 and INSM1 in the control of neuroendocrine differentiation, similar data are currently lacking for YAP1. Whether high YAP1 represents a transcriptional driver of this subtype or a subtype-specific correlate in this subtype has not been determined.
A recent human transcription factor domain-focused CRISPR screen identified POU class 2 homeobox 3 (POU2F3) as being expressed and essential in a subtype of SCLC cell lines lacking high levels of expression of both ASCL1 or NeuroD1 (ref.35). POU2F3 is normally selectively expressed in tuft cells, a rare chemosensory cell type in the pulmonary epithelium36. POU2F3-expressing SCLC cell lines lack typical neuroendocrine markers and demonstrate an expression profile similar to that of tuft cells, suggesting the possibility of a distinct cell of origin35. Intriguingly, the same screen revealed additional transcription factor dependencies that appear unique to the POU2F3-expressing subtype of SCLC, including an alternative achaete-scute homologue, ASCL2, previously identified as overexpressed in non-neuroendocrine SCLC37. Whereas POU2F3-positive tumours express variable levels of YAP1, the relative expression of YAP1 and POU2F3 defines distinct populations of YAP1-high and POU2F3-high tumours, defining a third and fourth subtype of SCLC from the non-neuroendocrine subtype. Our current understanding of the data suggests that additional subtypes of SCLC lacking the expression of one of these four genes (ASCL1, NEUROD1, YAP1 or POU2F3) would be rare.
Intratumoural heterogeneity
The analysis of mutations in TP53 and RB1 in human SCLC has led to the idea that primary SCLC tumours are more clonal (and thus harbour fewer genetically heterogeneous clones) than other types of lung cancer such as lung adenocarcinoma38. As discussed above, there is no clear evidence in primary tumours that specific genetic events in SCLC lead to the growth of different subtypes; however, data from mouse genetics indicate that high levels of MYC can push SCLC cells towards the NeuroD1-high state. Furthermore, activation of Notch via overexpression of Notch intracellular domain (NICD) in the Trp53/Rb1/Rbl2 conditional knockout GEMM leads to the outgrowth of ASCL1-low/NeuroD1-low tumours, and it is possible that inactivating mutations in Notch genes in human tumours influence the fate of SCLC cells towards specific subtypes. Beyond the antagonistic relationship between activation of Notch signalling and expression of ASCL1 (refs13,39), the functional interactions between Notch pathway activity and the transcription regulators defining the four major subtypes remain to be investigated. More work is needed to better understand how the genetics of SCLC tumours control the presence and the growth of SCLC subtypes. Furthermore, emerging evidence supports a model in which biologically relevant intratumoural heterogeneity can occur within SCLC tumours and during SCLC progression, including functionally distinct subpopulations of interacting cells30. The generation of PDX mouse models from biopsy samples or circulating tumour cells both pretreatment and again on progression may prove particularly important in providing insight into the evolving intratumoural heterogeneity associated with chemotherapy resistance40,41.
SCLC cultures in vitro often are notable for morphologically different cell types, including in some cases mixtures of cells in suspension or loosely adherent and more strongly adherent monolayers10. Expression profiling of these distinct populations suggests that the suspended cells have more typical epithelial neuroendocrine features, whereas the adherent population adopts a more mesenchymal (non-neuroendocrine) expression profile10,37. The Berns laboratory demonstrated that these distinct populations also exist in mouse SCLC tumours and that a mixture of neuroendocrine and non-neuroendocrine cells had substantially enhanced capacity for liver metastasis versus isolated populations of either neuroendocrine or non-neuroendocrine subtypes42. A paracrine signalling pathway driven by expression of the ETS family transcription factor protein PEA3 in non-neuroendocrine cells has been implicated in promoting the enhanced metastasis of neuroendocrine cells in vivo43. Recent data have further demonstrated that activation of Notch signalling, generally suppressed in the predominant ASCL1-high SCLC subtype, can induce a neuroendocrine to non-neuroendocrine fate switch in both mouse and human SCLC cells39. Notch signalling induces the transcriptional repressor REST, which in turn leads to expression of HES1 specifically in non-neuroendocrine phenotype cells. Non-neuroendocrine derivatives have a reduced proliferative rate but are relatively chemoresistant and appear to support the survival and growth of the neuroendocrine subtype of cells within admixed tumours. Another level of intratumoural heterogeneity is suggested by the recent description of vascular mimicry in SCLC: differentiation of SCLC cells to express vascular endothelial cadherin and adoption of a distinct morphology with tumour-derived cells lining intratumoural blood-containing sinusoids44. Vascular mimicry may also contribute to robust tumour growth and chemoresistance in vivo. Whether this heterogeneity (mesenchymal-like SCLC cells, Notch-high REST-high SCLC cells and vascular-like SCLC cells) may relate to the four subtypes discussed above remains to be investigated.
Synthesis of available data
The recent SCLC profiling studies of both primary human and mouse tumours summarized above support a model of distinct SCLC molecular subtypes defined by relative expression of key transcription regulators among the class of tumours defined by the World Health Organization (WHO) 2015 classification as SCLC. Importantly, the primary tumours described in this synthesis were all confirmed by expert lung pathologists to meet the diagnostic criteria for SCLC using the criteria described in Box 1 (refs11,13). Most SCLCs express INSM1, a marker of both ASCL1-high and NeuroD1-high neuroendocrine subtypes. Representative GEMMs exist that appear to reflect these categories. A small fraction of SCLC tumours is INSM1-low, ASCL1-low and NeuroD1-low. These tumours lack neuroendocrine markers and appear to fall into discrete YAP1-high and POU2F3-high subtypes.
Evidence for these subtypes of SCLC has emerged from our multiple research teams working both collaboratively and independently: a variety of identifying terminology has been employed by different groups while broadly describing the same subtypes (Fig. 1). We now propose referring to these molecular subtypes as SCLC-A, SCLC-N, SCLC-Y and SCLC-P, with the last letter signifying the transcription regulator most strongly associated with each subtype — that is, ASCL1, NeuroD1, YAP1 and POU2F3, respectively.

Key studies described in the text that have defined small cell lung cancer (SCLC) subtypes on the basis of differential gene expression are aligned in temporal order, with the nomenclature proposed in this article at the bottom. Referenced articles include refs.9,13,14,18,25,27,32,34,35. ASCL1, achaete-scute homologue 1; INSM1, insulinoma-associated protein 1; NE, neuroendocrine; NeuroD1, neurogenic differentiation factor 1; POU2F3, POU class 2 homeobox 3; YAP1, yes-associated protein 1.
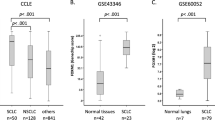
Differential expression of the discriminant transcription regulators can clearly distinguish these subtypes in both cell lines (n = 54) and in human tumours (n = 81) for which gene expression profiling is publicly available (Fig. 2a). Where multiple transcription regulators are expressed, samples are classified by the expression level of the transcription regulator with the greatest relative overall expression. A version of these data with individual cell lines and tumours identified is available online (Supplementary Fig. 1; Supplementary Table 1). On the basis of the 81 primary tumours, it appears that the proportion of SCLC-A is greatest (0.70 95% CI [0.60, 0.79]), followed by SCLC-N (0.11 95% CI [0.06, 0.20]), SCLC-Y (0.02 95% CI [0.01, 0.09]) and SCLC-P (0.16 95% CI [0.10, 0.26]) (Fig. 2b). We fully recognize that characterization of SCLC subtypes is still an area of active investigation and that these designations may need to change or be further specified. For example, although the transcription regulators outlined here are sufficient for accurate classification of the four proposed molecular subtypes, three of the authors (T.G.O., J.D.M. and A.F.G.) have proposed a multigene neuroendocrine/non-neuroendocrine score that also distinguishes SCLC-A and most SCLC-N from the non-neuroendocrine subtypes (SCLC-Y and SCLC-P) and may be more robust to noise37. ASCL1 expression is variable among SCLC-N subtype tumours, and it is currently unclear to what extent tumours that express multiple transcription regulators at different levels may differ from tumours defined by a single expressed transcription regulator. Multiple genes demonstrate differential expression among these subtypes (for example, Fig. 2c), and improved classifiers may therefore emerge in the future. In this respect, recent preliminary work has analysed transcription factors that must be either active (master regulators) or silenced (master destabilizers) in SCLC subtypes by assessing the dynamic equilibrium states of a transcription factor regulatory network with a combination of Boolean logic and Bayesian inference27. It remains to be seen whether this approach will provide more effective SCLC subtype classifiers. The elaboration of additional layers of complex transcriptional networks is critical for our understanding of the underlying biology of these tumours; however, this information may be dispensable for accurate classification. Despite these caveats, we think there will be value to the SCLC research community in a unified nomenclature now to clarify the currently fragmented terminology used in the literature, to foster communication among investigators and to serve as a framework for addressing active research questions in both preclinical and, ultimately, clinical research.

a | Hierarchical clustering of relative gene expression of four key transcription regulators defining subtypes in human small cell lung cancer (SCLC), including in primary tumours from Rudin et al.11 and George et al.13 (n = 81) and cell lines in the Cancer Cell Line Encyclopedia (CCLE) (n = 54)70. Clustering was performed using the R statistical computing environment, and the colour bar scale represents relative expression on a log scale. A version of these data with individual cell lines and tumours identified is available online (Supplementary Fig. 1; Supplementary Table 1). b | Estimates of relative frequencies of the four subtypes based on representation in primary human tumour data sets with 95% CIs (n = 81). c | Examples of differential expression of genes of interest (MYC, BCL2 and DLL3 are shown) among each subtype in primary human tumours (n = 81). NE, neuroendocrine.
Therapeutic implications
A better understanding of the critical signalling pathways operant in particular SCLC subtypes may define vulnerabilities and therapeutic targets. Indeed, recent data suggest that several putative targets being actively investigated in SCLC patients represent subtype-specific vulnerabilities. Delta-like protein 3 (DLL3), a target of multiple SCLC therapeutics now in clinical development, including an antibody drug conjugate, a bi-specific T cell engager and a chimeric antigen receptor (CAR)–T cell construct, is a direct transcriptional target of ASCL1; activity of these therapies can be anticipated to be highest in SCLC-A tumours on the basis of preferential expression of the target in this subtype45 (Fig. 2c). BCL2 is another direct transcriptional target of ASCL1 and is the focus of clinical development of multiple targeted inhibitors in active SCLC clinical trials; enrolment to these studies is currently biomarker unrestricted, but activity may be highest in SCLC-A18,46. CREBBP, one of the most frequently inactivated genes in human SCLC, encodes a histone acetyltransferase. A recent study found that in an Rb1/Trp53/Crebbp-deficient GEMM, Crebbp loss accelerates development of SCLC tumours (predominantly the SCLC-A subtype), albeit with selective activation of genes associated with epithelial-to-mesenchymal transition47. The Rb1/Trp53/Crebbp-deficient model demonstrates greater sensitivity to the histone deacetylase inhibitor pracinostat than Rb1/Trp53-deficient controls. The activity of another epigenetic modifier, the histone demethylase LSD1, has been reported to be dependent on disruption of INSM1 and GFI1B in SCLC48. Recent data also demonstrate that LSD1 inhibition leads to NOTCH1 activation and resultant ASCL1 suppression in SCLC49. Together, these data suggest selective activity of LSD1 inhibitors, which have been and are being explored in SCLC patients50, primarily in SCLC-A patients. We described above the SVV oncolytic virus, with selective tropism for SCLC-N subtype disease. This agent showed disappointing activity as a single agent in an unselected SCLC patient population51, but with appropriate biomarker-guided patient selection the SVV oncolytic virus could have selective efficacy either as a single agent or as a strategy to augment immunotherapy by introducing viral antigens selectively in tumour cells. A study randomizing unselected SCLC patients to chemotherapy with or without an insulin-like growth factor 1 receptor (IGF1R) inhibitor demonstrated no statistically significant difference in outcome52. However, the rare SCLC-P cell lines demonstrate a unique vulnerability to IGF1R depletion, suggesting re-exploration of IGF1R inhibitors as a targeted therapy approach specific to this subtype35.
One of the most promising areas of current clinical investigation in SCLC focuses on agents targeting DNA damage repair and cell cycle checkpoints53. The nearly universal loss of p53 and RB, two critical regulators of cell cycle progression, may make SCLC tumours of multiple subtypes particularly susceptible to genomic damage. Targets of particular interest here include poly(ADP-ribose) polymerase (PARP); the DNA damage response kinase ataxia telangiectasia and Rad3-related protein (ATR); and the cell cycle checkpoint kinases CHK1, WEE1 and aurora kinase A (AURKA), among others. A clinical trial of paclitaxel with or without alisertib, an investigational AURKA and AURKB inhibitor, showed only minor improvement in progression-free survival (PFS) in an unselected SCLC patient population, but a subtype analysis showed a remarkable benefit of alisertib specifically in patients with MYC-high tumours, in which PFS more than doubled; by contrast, patients with MYC-low tumours did better on chemotherapy alone (interaction P = 0.0006). This result is entirely consistent with data from the Trp53−/−;Rb1−/−;MycT58A GEMM (which include SCLC-N MYC-high tumours), which demonstrated the same selective sensitivity to aurora kinase inhibition32. Activity of the CHK1 inhibitor prexasertib in SCLC cell lines also appeared to correlate with MYC expression, although this agent also shows high-level single-agent activity in an SCLC-A mouse model54. Whether other cell cycle checkpoint and DNA damage repair targets have subtype-selective activity has not been reported.
Continuing to explore these and other targeted therapies that might be subtype-specific in SCLC patients irrespective of tumour subtype or biomarker selection creates two major problems in therapeutic research. First, enrolment of an unselected patient population may mask the benefit of a targeted therapy in a select subtype, resulting in active drugs being discarded. Second, this approach by necessity leads to study participation by patients whose tumours lack the target and who are thus unlikely to benefit. As an initial suggestion, we would propose that subtype categorization be assessed as a correlate of clinical outcomes in ongoing and recently completed trials in SCLC to provide clinical insight into both the prognostic significance of subtype classification and the predictive significance for both standard and investigational therapies. Hypothesized subtype-specific vulnerabilities based on preclinical and these exploratory clinical analyses could be validated in subsequent prospective clinical trials.
Open questions
Identification and characterization of SCLC subtypes is a work in progress, and many questions remain. We list some of particular interest here.
Do subtypes reflect different cells of origin and/or oncogenic pathways?
The recent description of SCLC-P, with an expression profile closely resembling that of pulmonary tuft cells, strongly suggests a distinct cell of origin for this subtype, although transdifferentiation towards a tuft cell expression profile from a cell of origin shared with other subtypes remains an alternative explanation35. Data from the Berns laboratory noted above suggest that different cells within the respiratory epithelium can give rise to tumours resembling SCLC29; it is not clear whether this is also the case in human SCLC. To what extent are different subtypes in either mice or humans reflective of different origins and different developmental histories?
Do subtypes have different metastatic drivers or organ tropisms?
The lethality of SCLC is largely due to its exceptional metastatic potential3. Very recent data using different promoters to direct CRE recombinase expression in distinct cell types in the lung (either to neuroendocrine cells specifically or to a broader array of possible cell types) in the Trp53/Rb1/Rbl2 conditional knockout GEMM surprisingly reveal different programmes of metastatic progression, with one model demonstrating metastases with consistent amplification of Nfib and increases in chromatin accessibility and the other demonstrating metastases with neither of these features30. NFIB amplification is a feature of some but not all human SCLC metastases: do these differ in subtype? Do subtypes dictate different patterns of predominant metastatic spread?
Is there biological plasticity between subtypes?
The apparent requirement for ASCL1 for SCLC tumorigenesis in mice in the context of Trp53/Rb1/Rbl2 deficiency, together with data demonstrating ASCL1 predominance in early lesions in the Trp53−/−;Rb1−/−;MycT58A GEMM, suggests a possible hierarchy, with SCLC-A being a necessary precursor of SCLC-N in the mouse25,32. Testing of this hypothesis, by inactivation of Ascl1 in this model, has not yet been reported. Can tumours evolve (perhaps under subtype-specific therapeutic selection) in the other direction, from SCLC-N to SCLC-A? Initial experience with flow cytometry showed that most SCLC cell lines express either neuroendocrine (NCAM1, CD24, CADM1 and ALCAM) or non-neuroendocrine (CD151 and EPHA2) surface markers, whereas a few expressed both; upon drug treatment, surface marker profiles shifted with increased numbers expressing both classes of marker, possibly owing to plasticity55. Will single-cell RNA-seq reveal representation of multiple subtypes, in varying ratios, in most (or all) SCLC tumours? By computational tumour deconvolution, preliminary data suggest that virtually all SCLC tumours were composed of multiple subtypes, signalling an urgent need for longitudinal studies reporting on intratumor heterogeneity with respect to progression and treatment27. If the rare SCLC-Y tumours do retain intact RB1, these may represent a truly separate tumour class. The relation of the newly discovered SCLC-P subtype to others remains to be determined, but it too may represent a distinct lineage.
Is subtype assignment in de novo disease prognostic?
Early observational data suggested that variant (that is, SCLC-N) cell lines were more commonly derived from previously treated patients, while classic (that is, SCLC-A) lines were more likely to be derived from untreated patients10. Are SCLC-N more chemoresistant? If SCLC-N is in fact over-represented in recurrent or chemoresistant disease, is this attributable to selection or tumour evolution? The SCLC-Y phenotype was found to be associated with poor prognosis, with shorter patient survival and increased chemoresistance34. The clinical outcomes for SCLC-P patients have not been defined.
How do the immune milieu and microenvironment differ between subtypes?
The most notable recent clinical progress against SCLC has centred around the use of immune checkpoint blockade targeting PD1 or PDL1 with or without concurrent targeting of CTLA4 (refs4,56). Initial studies of nivolumab (with or without the CTLA4 inhibitor ipilimumab) or another PD1 inhibitor, pembrolizumab, have explored previously described correlates of immune response, including PDL1 expression and tumour mutational burden56,57. Only a small minority of patients with SCLC demonstrate durable benefit from immunotherapy. Might immune checkpoint response differ in SCLC by tumour subtype? SCLC subtypes clearly differ substantially in cell surface proteins, including Notch receptors and adhesion molecules. Recent data point to a remarkable synergy between inhibition of PARP or CHK1 and PD1 blockade in immunocompetent mouse models of the SCLC-A subtype58. Whether these combinations will have broader application to other subtypes remains to be assessed. To date, no studies have examined subtype-specific differences in tumour stromal composition, immune infiltration or markers of immune activation. However, recent studies in lung adenocarcinoma point to tumour-specific determinants of immunoresistance, independent of known T cell interaction factors; therefore, it is reasonable to hypothesize that this might be true in SCLC as well59.
Are similar subtypes found in other neuroendocrine tumours?
Aggressive and lethal neuroendocrine tumours can arise from adenocarcinomas of the lung, prostate and other tissues under the selective pressure of targeted or hormonal therapies, and this lineage plasticity is associated with inactivation of TP53 and RB1 (refs60,61,62,63). Whether these tumours most closely resemble one of the subtypes of SCLC described here has not been defined. We have begun to dissect the genetic landscapes of large cell neuroendocrine cancers of the lung; these fall into at least two large classes — one with TP53 and RB1 deficiency resembling SCLC and the other with a mutational spectrum more closely related to lung adenocarcinoma64,65. Functional subtyping of SCLC derived from adenocarcinoma via lineage plasticity on the basis of gene expression profiling has not been reported. Understanding whether the subtypes of disease described here are specific to SCLC or are representative of broader commonalities among neuroendocrine cancers will be of interest and of potential relevance in defining therapeutic vulnerabilities.
Summary
We have made substantial progress over the past several years in our understanding of SCLC biology. One key insight emerging from complementary human and mouse investigation is the classification of SCLC subtypes defined by distinct gene expression profiles. Several therapeutic targets that are the focus of recent, active and planned clinical trials appear to differ in subtype specificity. Further investigation of the nature of these subtypes is needed to define their differences, commonalities and capacity for interconversion; what determines their growth, survival and metastasis; and their therapeutic vulnerabilities and dependencies. A better understanding of the biology of these subtypes, and application in the context of subtype-specific clinical investigations, may represent an important path forward in defining better treatments for SCLC.
Change history
07 June 2019
An amendment to this paper has been published and can be accessed via a link at the top of the paper.
27 June 2019
An author correction to Supplementary Table 1 was made, but the original file was not updated. We have now updated Supplementary Table 1 in the original article.
References
Gazdar, A. F., Bunn, P. A. & Minna, J. D. Small-cell lung cancer: what we know, what we need to know and the path forward. Nat. Rev. Cancer 17, 725–737 (2017).
Sabari, J. K. et al. Unravelling the biology of SCLC: implications for therapy. Nat. Rev. Clin. Oncol. 14, 549–561 (2017).
Hann, C. L. et al. in Cancer Principles & Practice of Oncology Ch. 49 (eds DeVita, V. T., Lawrence, T. S. & Rosenberg, S. A.) 671–700 (Wolters Kluwer, 2019).
Horn, L. et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N. Engl. J. Med. 379, 2220–2229 (2018).
von Pawel, J. et al. Topotecan versus cyclophosphamide, doxorubicin, and vincristine for the treatment of recurrent small-cell lung cancer. J. Clin. Oncol. 17, 658–667 (1999).
Ready, N. et al. Third-line nivolumab monotherapy in recurrent SCLC: CheckMate 032. J. Thorac. Oncol. 14, 237–244 (2018).
Jordan, E. J. et al. Prospective comprehensive molecular characterization of lung adenocarcinomas for efficient patient matching to approved and emerging therapies. Cancer Discov. 7, 596–609 (2017).
Gazdar, A. F. et al. Establishment of continuous, clonable cultures of small-cell carcinoma of lung which have amine precursor uptake and decarboxylation cell properties. Cancer Res. 40, 3502–3507 (1980).
Carney, D. N. et al. Establishment and identification of small cell lung cancer cell lines having classic and variant features. Cancer Res. 45, 2913–2923 (1985).
Gazdar, A. F. et al. Characterization of variant subclasses of cell lines derived from small cell lung cancer having distinctive biochemical, morphological, and growth properties. Cancer Res. 45, 2924–2930 (1985).
Rudin, C. M. et al. Comprehensive genomic analysis identifies SOX2 as a frequently amplified gene in small-cell lung cancer. Nat. Genet. 44, 1111–1116 (2012).
Peifer, M. et al. Integrative genome analyses identify key somatic driver mutations of small-cell lung cancer. Nat. Genet. 44, 1104–1110 (2012).
George, J. et al. Comprehensive genomic profiles of small cell lung cancer. Nature 524, 47–53 (2015).
Poirier, J. T. et al. Selective tropism of Seneca Valley virus for variant subtype small cell lung cancer. J. Natl Cancer Inst. 105, 1059–1065 (2013).
Neptune, E. R. et al. Targeted disruption of NeuroD, a proneural basic helix-loop-helix factor, impairs distal lung formation and neuroendocrine morphology in the neonatal lung. J. Biol. Chem. 283, 21160–21169 (2008).
Borges, M. et al. An achaete-scute homologue essential for neuroendocrine differentiation in the lung. Nature 386, 852–855 (1997).
Ito, T. et al. Basic helix-loop-helix transcription factors regulate the neuroendocrine differentiation of fetal mouse pulmonary epithelium. Development 127, 3913–3921 (2000).
Poirier, J. T. et al. DNA methylation in small cell lung cancer defines distinct disease subtypes and correlates with high expression of EZH2. Oncogene 34, 5869–5878 (2015).
The Cancer Genome Atlas Research Network. Comprehensive genomic characterization of squamous cell lung cancers. Nature 489, 519–525 (2012).
Christensen, C. L. et al. Targeting transcriptional addictions in small cell lung cancer with a covalent CDK7 inhibitor. Cancer Cell 26, 909–922 (2014).
Lan, M. S. & Breslin, M. B. Structure, expression, and biological function of INSM1 transcription factor in neuroendocrine differentiation. FASEB J. 23, 2024–2033 (2009).
Fujino, K. et al. Insulinoma-associated protein 1 is a crucial regulator of neuroendocrine differentiation in lung cancer. Am. J. Pathol. 185, 3164–3177 (2015).
Gierl, M. S. et al. The zinc-finger factor Insm1 (IA-1) is essential for the development of pancreatic beta cells and intestinal endocrine cells. Genes Dev. 20, 2465–2478 (2006).
Wildner, H. et al. Insm1 (IA-1) is a crucial component of the transcriptional network that controls differentiation of the sympatho-adrenal lineage. Development 135, 473–481 (2008).
Borromeo, M. D. et al. ASCL1 and NEUROD1 reveal heterogeneity in pulmonary neuroendocrine tumors and regulate distinct genetic programs. Cell Rep. 16, 1259–1272 (2016).
Gratton, M. O. et al. Hes6 promotes cortical neurogenesis and inhibits Hes1 transcription repression activity by multiple mechanisms. Mol. Cell. Biol. 23, 6922–6935 (2003).
Wooten, D. et al. Small cell lung cancer subtypes identified by systems-level modeling of transcription factor networks. Preprint at bioRxiv https://www.biorxiv.org/content/10.1101/506402v2 (2018).
Meuwissen, R. et al. Induction of small cell lung cancer by somatic inactivation of both Trp53 and Rb1 in a conditional mouse model. Cancer Cell 4, 181–189 (2003).
Sutherland, K. D. et al. Cell of origin of small cell lung cancer: inactivation of Trp53 and Rb1 in distinct cell types of adult mouse lung. Cancer Cell 19, 754–764 (2011).
Yang, D. et al. Intertumoral heterogeneity in SCLC is influenced by the cell type of origin. Cancer Discov. 8, 1316–1331 (2018).
Schaffer, B. E. et al. Loss of p130 accelerates tumor development in a mouse model for human small-cell lung carcinoma. Cancer Res. 70, 3877–3883 (2010).
Mollaoglu, G. et al. MYC drives progression of small cell lung cancer to a variant neuroendocrine subtype with vulnerability to aurora kinase inhibition. Cancer Cell 31, 270–285 (2017).
Little, C. D. et al. Amplification and expression of the c-myc oncogene in human lung cancer cell lines. Nature 306, 194–196 (1983).
McColl, K. et al. Reciprocal expression of INSM1 and YAP1 defines subgroups in small cell lung cancer. Oncotarget 8, 73745–73756 (2017).
Huang, Y. H. et al. POU2F3 is a master regulator of a tuft cell-like variant of small cell lung cancer. Genes Dev. 32, 915–928 (2018).
Yamashita, J. et al. Skn-1a/Pou2f3 functions as a master regulator to generate Trpm5-expressing chemosensory cells in mice. PLOS ONE 12, e0189340 (2017).
Zhang, W. et al. Small cell lung cancer tumors and preclinical models display heterogeneity of neuroendocrine phenotypes. Transl Lung Cancer Res. 7, 32–49 (2018).
The Cancer Genome Atlas Research Network. Comprehensive molecular profiling of lung adenocarcinoma. Nature 511, 543–550 (2014).
Lim, J. S. et al. Intratumoural heterogeneity generated by Notch signalling promotes small-cell lung cancer. Nature 545, 360–364 (2017).
Hodgkinson, C. L. et al. Tumorigenicity and genetic profiling of circulating tumor cells in small-cell lung cancer. Nat. Med. 20, 897–903 (2014).
Drapkin, B. J. et al. Genomic and functional fidelity of small cell lung cancer patient-derived xenografts. Cancer Discov. 8, 600–615 (2018).
Calbo, J. et al. A functional role for tumor cell heterogeneity in a mouse model of small cell lung cancer. Cancer Cell 19, 244–256 (2011).
Kwon, M. C. et al. Paracrine signaling between tumor subclones of mouse SCLC: a critical role of ETS transcription factor Pea3 in facilitating metastasis. Genes Dev. 29, 1587–1592 (2015).
Williamson, S. C. et al. Vasculogenic mimicry in small cell lung cancer. Nat. Commun. 7, 13322 (2016).
Saunders, L. R. et al. A DLL3-targeted antibody-drug conjugate eradicates high-grade pulmonary neuroendocrine tumor-initiating cells in vivo. Sci. Transl Med. 7, 302ra136 (2015).
Cardnell, R. J. et al. Protein expression of TTF1 and cMYC define distinct molecular subgroups of small cell lung cancer with unique vulnerabilities to aurora kinase inhibition, DLL3 targeting, and other targeted therapies. Oncotarget 8, 73419–73432 (2017).
Jia, D. et al. Crebbp loss drives small cell lung cancer and increases sensitivity to HDAC inhibition. Cancer Discov. 8, 1422–1437 (2018).
Takagi, S. et al. LSD1 inhibitor T-3775440 inhibits SCLC cell proliferation by disrupting LSD1 interactions with SNAG domain proteins INSM1 and GFI1B. Cancer Res. 77, 4652–4662 (2017).
Augert, A. et al. Targeting NOTCH activation in small cell lung cancer through LSD1 inhibition. Sci. Signal. 12, eaau2922 (2019).
US National Library of Medicine. ClinicalTrials.gov https://clinicaltrials.gov/ct2/show/NCT02034123 (2019).
Rudin, C. M. et al. Phase I clinical study of Seneca Valley Virus (SVV-001), a replication-competent picornavirus, in advanced solid tumors with neuroendocrine features. Clin. Cancer Res. 17, 888–895 (2011).
Belani, C. P. et al. Vismodegib or cixutumumab in combination with standard chemotherapy for patients with extensive-stage small cell lung cancer: a trial of the ECOG-ACRIN Cancer Research Group (E1508). Cancer 122, 2371–2378 (2016).
Sen, T., Gay, C. M. & Byers, L. A. Targeting DNA damage repair in small cell lung cancer and the biomarker landscape. Transl Lung Cancer Res. 7, 50–68 (2018).
Sen, T. et al. CHK1 inhibition in small-cell lung cancer produces single-agent activity in biomarker-defined disease subsets and combination activity with cisplatin or olaparib. Cancer Res. 77, 3870–3884 (2017).
Udyavar, A. R. et al. Novel hybrid phenotype revealed in small cell lung cancer by a transcription factor network model that can explain tumor heterogeneity. Cancer Res. 77, 1063–1074 (2017).
Hellmann, M. D. et al. Tumor mutational burden and efficacy of nivolumab monotherapy and in combination with ipilimumab in small-cell lung cancer. Cancer Cell 33, 853–861 (2018).
Ott, P. A. et al. Pembrolizumab in patients with extensive-stage small-cell lung cancer: results from the phase Ib KEYNOTE-028 Study. J. Clin. Oncol. 35, 3823–3829 (2017).
Sen, T. et al. Targeting DNA damage response promotes anti-tumor immunity through STING-mediated T cell activation in small cell lung cancer. Cancer Discov. https://doi.org/10.1158/2159-8290.CD-18-1020 (2019).
Skoulidis, F. et al. STK11/LKB1 mutations and PD-1 inhibitor resistance in KRAS-mutant lung adenocarcinoma. Cancer Discov. 8, 822–835 (2018).
Sequist, L. V. et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci. Transl Med. 3, 75ra26 (2011).
Niederst, M. J. et al. RB loss in resistant EGFR mutant lung adenocarcinomas that transform to small-cell lung cancer. Nat. Commun. 6, 6377 (2015).
Mu, P. et al. SOX2 promotes lineage plasticity and antiandrogen resistance in TP53- and RB1-deficient prostate cancer. Science 355, 84–88 (2017).
Ku, S. Y. et al. Rb1 and Trp53 cooperate to suppress prostate cancer lineage plasticity, metastasis, and antiandrogen resistance. Science 355, 78–83 (2017).
Rekhtman, N. et al. Next-generation sequencing of pulmonary large cell neuroendocrine carcinoma reveals small cell carcinoma-like and non-small cell carcinoma-like subsets. Clin. Cancer Res. 22, 3618–3629 (2016).
George, J. et al. Integrative genomic profiling of large-cell neuroendocrine carcinomas reveals distinct subtypes of high-grade neuroendocrine lung tumors. Nat. Commun. 9, 1048 (2018).
Travis, W. D. et al. The 2015 World Health Organization Classification of Lung Tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J. Thorac Oncol. 10, 1243–1260 (2015).
Guinee, D. G. et al. The spectrum of immunohistochemical staining of small-cell lung carcinoma in specimens from transbronchial and open-lung biopsies. Am. J. Clin. Pathol. 102, 406–414 (1994).
Junker, K., Wiethege, T. & Muller, K. M. Pathology of small-cell lung cancer. J. Cancer Res. Clin. Oncol. 126, 361–368 (2000).
Kim, Y. H. et al. Combined microarray analysis of small cell lung cancer reveals altered apoptotic balance and distinct expression signatures of MYC family gene amplification. Oncogene 25, 130–138 (2006).
Barretina, J. et al. The Cancer Cell Line Encyclopedia enables predictive modelling of anticancer drug sensitivity. Nature 483, 603–607 (2012).
Acknowledgements
The authors thank N. Rekhtman for insightful comment regarding pathological criteria for small cell lung cancer diagnosis. This work was supported by grants from the US National Institutes of Health, including U24CA213274 (C.M.R., J.T.P., A.D., J.D.M. and A.F.G.), R01CA197936 (C.M.R., J.T.P. and C.D.), R01CA207295 (L.A.B.), U01CA213273 (L.A.B., J.V.H. and J.S.), P50CA70907 and U01CA213338 (J.E.J., J.D.M. and A.F.G.), U54CA217450 (J.M.L. and V.Q.), UG1CA233259 (J.M.L.) and R21CA216504 (T.G.O.); by Veterans Affairs Merit Review I01CX001425 (P.P.M.); by a LUNGevity Foundation Career Development Award (J.M.L.); and by Cancer Research UK A27412, A25254 and A20465 (C.D.).
Reviewer information
Nature Reviews Cancer thanks T. Bivona, E. Brambilla and other anonymous reviewer(s) for their contribution to the peer review of this work.
Author information
Authors and Affiliations
Contributions
C.M.R. and J.T.P. researched data for the article, made substantial contributions to the discussion of content, wrote the article and reviewed or edited the article before submission. The other authors all made substantial contributions to the discussion of content and reviewed or edited the article before submission.
Corresponding authors
Ethics declarations
Competing interests
C.M.R. has consulted for AbbVie, Amgen, Ascentage, AstraZeneca, BMS, Celgene, Daiichi Sankyo, Genentech/Roche, Ipsen, Loxo and PharmaMar; is on the scientific advisory board for Elucida and Harpoon; and receives research funding from Daiichi Sankyo. L.A.B. has consulted for AbbVie, AstraZeneca, BerGenBio, Genmab and PharmaMar and receives research support from AbbVie, AstraZeneca, Genmab and Tolero. C.D. has consulted for AstraZeneca and Merck and receives research funding from AstraZeneca, Epigene, Amgen, FLX Bio, Menarini and Angel. J.V.H. has consulted for AstraZeneca, Boehringer Ingelheim, Exelixis, Genentech, GlaxoSmithKline, Guardant, Hengrui, Lilly, Novartis, Spectrum, EMD Serono and Synta; has received research support from AstraZeneca, Bayer, GlaxoSmithKline and Spectrum; and receives royalties and licensing fees from Spectrum. J.M.L. receives research funding from Ipsen and AbbVie. D.M. received research funding from Janssen and Roche. J.D.M. and A.F.G. receive licensing royalties for cell lines from the US National Institutes of Health and the University of Texas Southwestern Medical Center. J.S. receives research funding from AbbVie. C.R.V. is an adviser to KSQ Therapeutics. All other authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Rudin, C.M., Poirier, J.T., Byers, L.A. et al. Molecular subtypes of small cell lung cancer: a synthesis of human and mouse model data. Nat Rev Cancer 19, 289–297 (2019). https://doi.org/10.1038/s41568-019-0133-9
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41568-019-0133-9
This article is cited by
-
C-Myc protein expression indicates unfavorable clinical outcome in surgically resected small cell lung cancer
World Journal of Surgical Oncology (2024)
-
Evolving insights into the improvement of adoptive T-cell immunotherapy through PD-1/PD-L1 blockade in the clinical spectrum of lung cancer
Molecular Cancer (2024)
-
Small cells – big issues: biological implications and preclinical advancements in small cell lung cancer
Molecular Cancer (2024)
-
Molecular profile of bladder cancer progression to clinically aggressive subtypes
Nature Reviews Urology (2024)
-
Genetically-engineered mouse models of small cell lung cancer: the next generation
Oncogene (2024)
