
Abstract
Study design:
Development of a prospective patient registry.
Objective:
To develop a patient registry for persons with traumatic spinal cord injuries (SCI), which can be used to answer research questions and improve patient outcomes.
Setting:
Nine provinces in Canada.
Methods:
The Rick Hansen Spinal Cord Injury Registry (RHSCIR) is part of the Translational Research Program of the Rick Hansen Institute. The launch of RHSCIR in 2004 heralded the initiation of the first nation-wide SCI patient registry within Canada. Currently, RHSCIR is being implemented in 14 cities located in 9 provinces, and there are over 1500 individuals who have sustained an acute traumatic SCI registered to date. Data are captured from the pre-hospital, acute and rehabilitation phases of care, and participants are followed in the community at 1, 2, 5 and then every 5 years post-injury.
Results:
During the development of RHSCIR, there were many challenges that were overcome in selecting data elements, establishing the governance structure, and creating a patient privacy and confidentiality framework across multiple provincial jurisdictions. The benefits of implementing a national registry are now being realized. The collection of an internationally standardized set of clinical information is helping inform clinicians of beneficial interventions and encouraging a shift towards evidence-based practices. Furthermore, through RHSCIR, a network is forming amongst SCI clinicians and researchers, which is fostering new collaborations and the launch of multi-center clinical trials.
Conclusions:
For networks that are establishing SCI registries, the experiences and lessons learned in the development of RHSCIR may provide useful insights and guidance.
Similar content being viewed by others

Introduction
A patient registry is defined as ‘an organized system that uses observational study methods to collect uniform data (clinical and other) to evaluate specified outcomes for a population defined by a particular disease, condition or exposure, which serves predetermined scientific, clinical or policy purpose(s)’.1 Given the devastating personal and economic consequences of spinal cord injury (SCI), it is critical to collect high quality, prospective data. Patient registries, when coupled with well-defined and methodologically strong research questions, can provide insights into a number of topics surrounding disease/condition progression and health care for a defined patient population.1 By identifying and substantiating interventions and techniques that are effective, a patient registry can support the increasingly recognized need for evidence-based practice. The data elements collected by patient registries commonly have standard definitions and are linked to the original data sources, ensuring that a centralized, comprehensive data set is provided.1 Registry data can also provide longitudinal information on patient outcomes, which are essential for our understanding of specific health conditions, and critical for evaluating the effectiveness of our interventions.1
In the context of SCI, in which patient survival is high, but neurologic recovery is variable,2 longitudinal patient data has the potential to inform clinicians which acute care, rehabilitation and/or community interventions contribute to positive long-term patient outcomes. Information collected from international SCI registries, such as the European Multi-center Study about Spinal Cord Injury, has already contributed to large-scale observational studies on topics such as American Spinal Injury Association (ASIA) Impairment Scale (AIS) validation3 and spontaneous recovery patterns.4 Other SCI registries such as the US Model SCI Database have contributed greatly to our understanding of the epidemiology of traumatic SCI5 and predictors of participation and quality of life following injury.6
In Canada, the first SCI patient registry known as the Rick Hansen Spinal Cord Injury Registry (RHSCIR) was launched in 2004. The RHSCIR supports the translational research activities of the Rick Hansen Institute (RHI) and other academic organizations in Canada. It was initiated with the vision of not only creating a national registry of individuals who sustain an acute traumatic SCI, but also linking researchers, clinicians, as well as patients with SCI, to facilitate clinical research and evidence-based practices in care delivery. Because of the publicly funded structure of Canada's health care system, RHSCIR is uniquely positioned to capture detailed information on the pre-hospital, acute, rehabilitation and community phases in a large representative sample of persons sustaining traumatic SCI. The purpose of this article is to provide an overview of how RHSCIR was developed, to share with the scientific community our experiences, insights and lessons learned during its development, and highlight potential impacts of implementing this kind of registry on clinical research and practice.
Overview of the national SCI registry: RHSCIR
The RHSCIR is a Canadian-wide observational database of patients with acute traumatic SCI admitted to major trauma centers and the accompanying rehabilitation centers. These centers, referred to as local ‘RHSCIR sites’, all obtain Institutional Research Ethics Board (REB) approval to enroll patients and enter their data into RHSCIR. Importantly, in the context of privacy protection, a data-sharing agreement is established between the facilities comprising the RHSCIR site, the university overseeing the clinical research and the RHI, to store data in a de-identified manner at the national office located in Vancouver, British Columbia, Canada.
At each site, local coordinators are funded by RHSCIR to recruit and consent patients and collect data. All patients clinically diagnosed with an acute traumatic SCI are eligible to be included in RHSCIR, and are approached to obtain informed consent. For patients who consent to be part of RHSCIR, approximately 265 data elements are collected during the pre-hospital, acute and in-patient rehabilitation phases of their care (see Table 1 and Supplementary Appendix I), including socio-demographic factors, medical history, injury details, diagnoses and interventions, neurologic impairment, complications and patient-reported outcomes. Upon discharge into the community, RHSCIR participants are contacted at 1, 2, 5 and 10 years from the date of injury, to complete the patient-reported outcome measures conducted either by an interviewer or by a self-administered questionnaire. This follow-up is intended to continue for every 5 years until death or the participant's voluntary withdrawal from RHSCIR.
For patients who do not consent to be a part of RHSCIR or who were missed and added later when the RHSCIR enrollment was reconciled with the hospital health records, a ‘minimal data set’ is collected through medical chart abstraction. This data set contains only a minimal number of data elements to document the type of traumatic SCI, as well as the characteristics of the injury and person who sustains it. The minimal data set is included to ensure the population-based information is collected from each site with no selection bias, an important lesson learned from the Registry of the Canadian Stroke Network.7 As some patients with traumatic SCI, particularly those with AIS D are often admitted to community hospitals, RHSCIR does not capture all incident cases of traumatic SCI in Canada; however, centers with the highest patient volume were selected as RHSCIR sites.
Data recorded by the local RHSCIR representatives are based on standard definitions. Where possible, the data elements are aligned with the International SCI Data Sets,8 to ensure the registry will be able to facilitate the exchange of data internationally. To prevent duplication of data collection, data are linked locally to other data sources (for example, trauma registry). All data are then entered into the local RHSCIR database and de-identified before being exported electronically to the national RHSCIR office.
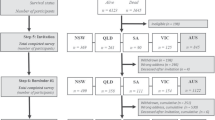
To date, RHSCIR has been implemented in 14 Canadian cities located in nine provinces (Figure 1), which account for almost all of the Canadian population. Currently, with the local sites actively enrolling and exporting data into the national RHSCIR, there are over 1500 unique participants in the national database (Figure 2).

A map of Canada indicating the location of the 14 RHSCIR sites.

The cumulative enrolment in the RHSCIR by Canadian province. The RHSCIR sites in St. John's Newfoundland and Saint John New Brunswick are still preparing to launch and no data has been collected as of December 2010. Participants enrolled in 2004 are included in the 2005 estimate and enrollment is up until 22 November 2010. AB, Alberta; BC, British Columbia; MB, Manitoba; NS, Nova Scotia; ON, Ontario; QC, Quebec; SK, Saskatchewan.
Development of RHSCIR and its impact on SCI research and care
Although randomized, controlled trials are considered the benchmark method for assessing the efficacy of novel therapies, they have profound limitations: being dependent upon strict inclusion and exclusion criteria, large numbers of participants and the need to standardize all aspects of care other than those being studied.9
In contrast, observational studies often include a broader representation of a patient population of interest. Observational studies are well-suited for investigating potential connections between clinical care and patient outcome, as the statistical models can adjust for confounders such as coexisting conditions.10, 11 This not only increases the relevance of such studies, but also provides a more accurate representation of the actual clinical setting. Observational studies are more relevant for determining the efficacy of the real world treatment protocols as opposed to the effectiveness of a single intervention in an idealized clinical setting(s).
Challenges of developing and implementing patient-registries have been documented.1 In designing a registry, it is critical that its purpose is clearly defined a priori, as the burden of collecting the data can easily outweigh the data's usefulness if sufficient thought does not go into what data elements ought to be captured (and why). Registries can also can extremely expensive to operate and hence, the value of a registry needs to be carefully considered and clearly articulated. Finally, a registry needs an effective governance structure to set the research agenda, and ensure appropriate and timely access to the data. Below are some lessons learned with respect to selecting the data elements and implementing a governance structure. Furthermore, examples of how RHSCIR has facilitated clinical research and evidence-based practices in care delivery are described.
Deciding upon data content
Researchers, clinicians and persons with SCI were consulted regarding the type of information they felt would be useful to have within a national SCI registry. There was an interest in capturing information along the continuum from the time of injury until the end of life in the community, a task made possible by the unique single-payer funding within the publicly funded Canadian health care system. Researchers wanted RHSCIR to capture data that would allow them to answer questions related to the epidemiology of the injury and the effectiveness of a variety of current and proposed treatments. As RHSCIR is implemented at large trauma and rehabilitation centers across Canada and standardizes the collection of data, researchers articulated the desire to use it to facilitate the implementation of clinical trials. Clinicians also wanted to have information that would enable them to evaluate the quality of care delivery and to facilitate the implementation of evidence-based practices. Finally, persons with SCI wanted to be notified of upcoming and ongoing research studies (particularly neuroprotective trials), whereas the SCI community organizations wanted aggregate data to help them better understand the people whom they serve.
Following consultation with these groups, research questions and data requirements were developed (see Table 2 and Supplementary Appendix I), using an iterative approach with the goal of obtaining consensus among the various groups. In addition, an environmental scan of international SCI databases was conducted as part of a workshop held in 2002 at the joint ASIA and International Spinal Cord Society meeting in Vancouver, British Columbia, Canada, which identified data elements commonly included in SCI registries at that time. As with all registries, striking the balance between collecting too much versus not collecting enough data was recognized as a major challenge. Consideration was given to the broad range of users and their short- and long-term data requirements. To accommodate future research studies, the data elements required to link the local RHSCIR data to other clinical and administrative databases were incorporated. A study at one of the RHSCIR sites is planning to link RHSCIR to other external databases and examine the use of health care services following discharge into the community. The RHSCIR data set will be revised in 2011, and where possible, the data set will be further aligned with the International SCI Data Sets.8 A current limitation of RHSCIR is that it does not include non-traumatic SCI and it does not include enough clinically relevant rehabilitation measures. To address this gap, we are working on the development of a non-traumatic SCI data set the incorporation of additional rehabilitation elements.
Governance
The governance structure for RHSCIR has evolved during its development. There was a transition from a Steering Committee to a more permanent Data Executive Scientific Committee, when the majority of the trauma and rehabilitation sites joined the RHSCIR network. Currently, the Data Executive Scientific Committee critically reviews data requests (Figure 3). Once approved by the Data Executive Scientific Committee, access to and usage of the national de-identified data must then be approved by the Data Access Committee to remain in accordance with the privacy protection framework established by the RHI to manage its SCI data holdings. The Data Access Committee comprised of a custodian from each of the RHSCIR participating sites and ultimately provides approval for disclosure of the site data. For scientific papers that emerge from national RHSCIR data, authorship guidelines have been established that recognize both the contribution of data and the scientific input on the research projects. In contrast, it should be noted that investigators at each RHSCIR site remain in full control over access to their own local site data so that they have the freedom to continue to do their own institutional studies.

Overview of the process to review and approve data requests involving national RHSCIR data.
Examples of how RHSCIR has facilitated clinical research and care delivery
With the RHSCIR sites now collecting data, the ability of the Registry to facilitate clinical research is being realized (see Table 2). Local sites are now using RHSCIR to determine if patients are eligible for upcoming research projects at their sites. Registry participants consent to being contacted by the local RHSCIR team regarding upcoming studies when they sign the RHSCIR consent form, which helps streamline the recruitment process for future studies. For example, if a RHSCIR participant indicates that they would like to be notified regarding upcoming studies the local RHSCIR team can directly contact these patients once the study receives REB approval, rather than relying on the health professionals providing the patients’ care to be the first point of contact. By serving as the primary contact between the RHSCIR participants and local clinical researchers, RHSCIR has helped expedite the recruitment process. In addition, two clinical studies sponsored by the RHI will soon be launched at sites within the RHSCIR network. These clinical studies will leverage the data elements collected for RHSCIR, thereby eliminating duplicate data collection and facilitating the use of standardized data definitions. Other ongoing studies are using RHSCIR data to investigate which patient-flow models result in superior patient outcomes as a precursor to the creation and implementation of new best practices.
The implementation of the RHSCIR data set has established standards for SCI clinical practice at participating RHSCIR sites and has positively impacted patient care. For example, during the RHSCIR development phase, pilot studies,12 in one province, aligned data collection in four spinal trauma centres and two rehabilitation centres leading to substantial enhanced communication and continuity across the care continuum plus the establishment of infrastructure for multi-site research studies that are now being funded by RHI. The need to standardize data collection at the RHSCIR sites has ensured that each site received training by qualified clinical staff on administering the International Standards for the Neurological Classification of SCI (ISNCSCI)13 and the International Core Data Set.14 This not only improves the data quality, but also provides ongoing training to all SCI clinical staff at facilities participating within the RHSCIR site; this may include physicians, nurses, physiotherapists and other allied health professionals. The approach enhances knowledge translation as these practitioners are training the next generation of health professionals who will be providing care for individuals with SCI. Since the implementation of RHSCIR, there has been an increase in the number of sites administering the ISNCSCI, which has improved the clinical reporting of SCIs. Local sites also use RHSCIR data to report to hospital administrators regarding the number and type of SCIs, which has helped justify staffing resources and bed allocations.
Challenges to launching RHSCIR: obtaining ethics approval and protecting privacy
Protecting the privacy of registry participants is fundamental to the RHSCIR project. All sites obtain study approval from their respective REBs to implement RHSCIR, which aligns the Registry project to that of clinical trials and ensures research is conducted in accordance with the Best Practices for Protecting Privacy in Health Research of the Canadian Institute for Health Research and the Tri-Council Policy Statement.15, 16 All of the participating RHSCIR sites adhere to one standardized study protocol prepared by the national RHSCIR team. Some differences in provincial and local processes and privacy requirements for obtaining REB approval have been challenging for RHSCIR resulting in some delays in participant recruitment and data collection. Collection of a minimal data set from patients who do not provide consent has been particularly problematic. The current minimal data set includes data related to age, gender, details of the injury, neurological assessment and clinical procedures, but in a few RHSCIR sites, the REBs have only allowed age, gender and date of injury to be collected. However, the implementation of RHSCIR in various provinces across Canada has enabled the national and local RHSCIR site staff to demonstrate the approval of the data set in other jurisdictions as a means of addressing specific REBs concerns.
To ensure the protection of patients’ privacy, the data is de-identified once it leaves the local RHSCIR sites. Identification of patient information is maintained between local and national data sets via a unique ‘RHSCIR identification number,’ which functions as a link to the personal identifiers within the patient information, held at the local sites. The Registry identification numbers are also used to prevent duplication in data collection and facilitate tracking of patient transfers between sites. Storage and handling of the identifying SCI data at local RHSCIR sites is also subject to the privacy regulations of the respective province. Local sites are obliged to follow their own institutional guidelines with respect to privacy and security policies. Since the launch of RHSCIR in 2004, new privacy legislations have been introduced at both the national and provincial levels. The interpretations of provincial legislations also vary, depending on the provincial privacy commissioners and institutional and/or health authority privacy officers. These variations have created considerable challenges for RHSCIR to standardize its policies and procedures across all sites. In response to these or any future privacy jurisdictions the Registry may encounter, the RHI proactively created a national privacy and security framework for RHSCIR's personal health information handling practices that meets a ‘high-water mark’ of best practices across Canada. The framework is based on international privacy requirements and ensures a ‘gold standard’ and consistent approach to protecting the privacy of RHSCIR participants.
A new web-platform is currently being developed to collect and manage data called the Global Research Platform, with the first release scheduled for late 2011. The new platform will be built using the principles of ‘Privacy by Design,’17 which encourage the concept of planning for privacy protection throughout the development life cycle, thereby embedding it into the product as well as the culture of the organization, making protection of privacy the default mode of operation. For example, a toolkit developed by Privacy Analytics18 is embedded into the data disclosure process, which evaluates and facilitates management of the risk of re-identification for a particular analytical data set before it is released.
Conclusion
There are numerous benefits to developing a patient registry, some of which include providing a repository of data for researchers, a mechanism to introduce and validate evidence-based practice, and the infrastructure for clinical trials. These benefits are quickly being realized in Canada with the implementation of RHSCIR. The RHI is currently expanding RHSCIR internationally and the data set will continue to align with international SCI data sets. Maintaining the privacy of the Registry participants and security of the data remain fundamental priorities for RHSCIR and will continue to be a focus of the new web-platform. Lessons learned from the Registry of the Canadian Stroke Network have shaped RHSCIR, and perhaps our lessons learned from RHSCIR can further inform future SCI registry initiatives.
References
Gliklich RE, Dreyer NA eds. Registries for Evaluating Patient Outcomes. (Prepared by Outcome DEcIDE Center under Contract No. HHSA-290-200-500-35I.). Agency for Healthcare Research and Quality: Rockville, 2010.
Fisher CG, Noonan VK, Dvorak MF . Changing face of spine trauma care in North America. Spine 2006; 31 (11 Suppl): S2–S8; discussion S36.
van Middendorp JJ, Hosman AJ, Pouw MH, van de Meent H . Is determination between complete and incomplete traumatic spinal cord injury clinically relevant? Validation of the ASIA sacral sparing criteria in a prospective cohort of 432 patients. Spinal Cord 2009; 47: 809–816.
Curt A, van Hedel HJ, Klaus D, Dietz V . Recovery from a spinal cord injury: significance of compensation, neural plasticity, and repair. J Neurotrauma 2008; 25: 677–685.
Jackson AB, Dijkers M, Devivo MJ, Poczatek RB . A demographic profile of new traumatic spinal cord injuries: change and stability over 30 years. Arch Phys Med Rehabil 2004; 85: 1740–1748.
Dijkers MP . Correlates of life satisfaction among persons with spinal cord injury. Arch Phys Med Rehabil 1999; 80: 867–876.
Tu JV, Willison DJ, Silver FL, Fang J, Richards JA, Laupacis A et al. Impracticability of informed consent in the Registry of the Canadian Stroke Network. N Engl J Med 2004; 350: 1414–1421.
Biering-Sorensen F, Charlifue S, DeVivo M, Noonan V, Post M, Stripling T et al. International spinal cord injury data sets. Spinal Cord 2006; 44: 530–534.
Abel U, Koch A . The role of randomization in clinical studies: myths and beliefs. J Clin Epidemiol 1999; 52: 487–497.
Roder C, Muller U, Aebi M . The rationale for a spine registry. Eur Spine J 2006; 15 (Suppl 1): S52–S56.
Black N . Why we need observational studies to evaluate the effectiveness of health care. BMJ 1996; 312: 1215–1218.
Ontario Spinal Cord Informatics: Informing Practice Research and Innovations. Ontario Neurotrauma Foundation, November, 2009. Available from: http://www.onf.org.
American Spinal Injury Association. Reference Manual of the International Standards for Neurological Classification of Spinal Cord Injury. American Spinal Injury Association: Chicago, 2003.
DeVivo M, Biering-Sorensen F, Charlifue S, Noonan V, Post M, Stripling T et al. International spinal cord injury core data set. Spinal Cord 2006; 44: 535–540.
Canadian Institutes of Health Research (CIHR). CIHR Best Practices for Protecting Privacy in Health Research [document on Internet]. Canadian Institutes of Health Research: Ottawa, 2005 [cited 2010 Nov 18]. Available from: http://www.cihr-irsc.gc.ca/e/29072.html.
Canadian Institutes of Health Research Natural Sciences and Engineering Research Council of Canada, and Social Sciences and Humanities Research Council of Canada. Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans, December 2010.
Privacy by Design (homepage on the Internet). Information and Privacy Commissioner of Ontario: Toronto, 2010 (cited 2010 Nov 18). Available from: http://www.privacybydesign.ca.
Privacy Analytics (homepage on the Internet). Privacy Analytics Inc.: Ottawa, 2008–2010 (cited 2010 Nov 18). Available from: http://www.privacyanalytics.ca.
Acknowledgements
Funding for this project was provided by the Rick Hansen Foundation and Health Canada. We would like to acknowledge the contributions of Catherine McGuinness, Rob Hickling, Sylvia Kingsmill, Lise Bélanger, John Cobb, Brian Sun, M Verrier and Janet Mou in the preparation of this manuscript.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
Dr Noonan and Ms Lesley Soril are employees of the RHI. Drs Brian Kwon, Michael Fehlings and Marcel Dvorak have received funding from the RHI to implement the Rick Hansen SCI Registry at their institutions and they also consult for the RHI. Drs John Hurlbert and Michael Johnson have received funding from the Rick Hansen Institute to implement the Rick Hansen SCI Registry at their institutions. Dr Andrea Townson declares no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Spinal Cord website
Supplementary information
Rights and permissions
About this article
Cite this article
Noonan, V., Kwon, B., Soril, L. et al. The Rick Hansen Spinal Cord Injury Registry (RHSCIR): a national patient-registry. Spinal Cord 50, 22–27 (2012). https://doi.org/10.1038/sc.2011.109
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2011.109
Keywords
This article is cited by
-
Studying missingness in spinal cord injury data: challenges and impact of data imputation
BMC Medical Research Methodology (2024)
-
Interrater reliability of the Standing and Walking Assessment Tool for spinal cord injury
Spinal Cord (2023)
-
The effect of rurality and distance from care on health outcomes, environmental barriers, and healthcare utilization patterns in persons with traumatic spinal cord injury
Spinal Cord (2023)
-
Technology used in activity based therapy for individuals living with spinal cord injury across Canada
Spinal Cord Series and Cases (2023)
-
Multimorbidity in persons with non-traumatic spinal cord injury and its impact on healthcare utilization and health outcomes
Spinal Cord (2023)
