
Abstract
Study design:
Pharmacologically blocking the spinal cord produces sedative effects and reduces anesthesia requirements in patients and animals. Whether spinal cord injury also reduces anesthesia requirements remains unclear.
Methods:
We retrospectively analyzed data from urethane-anesthetized rats15 to assess anesthesia requirements immediately after complete thoracic transection of the spinal cord. The depth of anesthesia was monitored up to 12 h after spinal transection by the reflexes to noxious stimuli and by electrophysiological recordings from the infragranular layers of the primary somatosensory cortex. Whenever animals displayed electrophysiological and/or behavioral signs of activation, we delivered an additional dose of anesthesia. Anesthetic requirements in animals receiving spinal transection (n=11) were compared with control animals receiving ‘sham’ lesion (n=9).
Results:
The cumulative dose necessary to maintain a stable level of anesthesia was significantly lower in transected animals compared with control animals. By about 7 h after spinal cord injury, on average the cumulative dose of urethane was only 1.13±0.14 of the original dose, compared with 1.64±0.19 of the original dose in control animals.
Conclusions:
Spinal transection immediately decreased anesthetic requirements in rats. To establish whether these results are relevant for patients with spinal cord injury will require further investigation.
Similar content being viewed by others

Introduction
A number of clinical studies have shown that spinal anesthesia can dramatically reduce the level of arousal in patients, thereby decreasing the requirements for sedation and general anesthesia.1, 2, 3, 4, 5, 6, 7, 8 The sedative effect of spinal anesthesia could be due to the loss of somatosensory inputs to the brain, as suggested by animal studies.9, 10, 11, 12, 13, 14 Therefore, at least in principle, spinal cord injury should have the same sedative effects as spinal anesthesia. Somewhat surprisingly, it is not a common clinical practice to consider that spinal cord injury patients might have lower anesthetic requirements than patients with intact spinal cord, possibly because of lack of studies directly addressing the problem. We recently showed that, similarly to spinal anesthesia, complete transection of the spinal cord immediately slows down cortical electroencephalography (EEG) activity in anesthetized rats.15 However, whether this slower EEG activity really reflects a state of deeper anesthesia after spinal cord injury remains unclear. To address this issue, we retrospectively analyzed the data from the same experiments to specifically investigate whether spinal cord injury decreases anesthetic requirements in the same animal model.
Materials and methods
Experiments were performed following the rules of International Council for Laboratory Animal Science (Barcelona, Spain), European Union regulation 86/609/EEC and were approved by the Ethical Committee for Animal Research of the Hospital Nacional de Parapléjicos (Toledo, Spain). A total of 23 male Wistar rats were used in this study, divided into 2 groups: (1) 14 animals received spinal cord transection and (2) 9 control animals received ‘sham’ injury. In our previous work, we studied changes in cortical evoked responses and spontaneous activity within the first hour after spinal transection.15 This time framework was too short to rigorously evaluate whether anesthesia requirements changed after the spinal cord transection. In the present work, we retrospectively analyzed data from the same animals, which were followed up to 12 h after the spinal cord transection, in order to specifically investigate changes in anesthesia requirements. The overall experimental protocol was described in detail in our previous study and is briefly restated below.
Animals were anesthetized with intra-peritoneal urethane, using an initial dose of 1.5 g/kg. The body temperature of the animal was kept constant at 36.5°C using an automatically controlled heating pad. A laminectomy was performed at thoracic level (T9-T10) keeping the dura mater intact and covered with agar (4%) in order to protect the area. The animals were placed in a stereotaxic frame (SR-6 Narishige Scientific Instruments, Tokyo, Japan), the skin of the head was softly removed and the skull was exposed. A craniotomy was performed on the right side of the midline over the somatosensory cortex (AP: 1 to −4; ML: 1–5; atlas of Paxinos and Watson, 2007), and the cisterna magna was opened to guarantee the stability of the recordings. Small incisions in the dura mater were performed to allow the recording electrodes to be lowered into the infragranular cerebral cortex (depth: 1.1 to 1.8 mm). Once the electrodes were placed in the hindpaw representation (antero–posterior: −0.5 to −1 mm; medio–lateral: 2 to 2.5 mm) and forepaw representation (antero–posterior: 0 to 0.5 mm; medio–lateral: 3.5 to 4.5 mm) of the primary somatosensory cortex, we performed a pre-lesion protocol, recording evoked responses and spontaneous activity with intact spinal cord.15 We then performed the complete transection of the spinal cord with a scalpel blade. Immediately after transection, few pulses of electrical stimulation of the hindpaw at very high intensity (0.5 Hz, 1 ms duration, 10 stimuli, 10 mA) were applied in order to confirm that no physiological responses were evoked in the cortex by stimuli delivered below the level of the lesion. The complete cut of the spinal cord was visually confirmed under the surgical microscope by the total separation of the borders. Between 10 and 30 min after the transection, we started the first post-lesion protocol, recording evoked responses and spontaneous activity with the spinal cord transected. Post-lesion protocols (up to 12) were then repeated approximately every hour. In control animals receiving ‘sham’ injury, the spinal cord remained intact after the laminectomy for the entire duration of the experiment. Besides the absence of spinal cord lesion, the experimental procedures were the same as in the transected animals. Both pre-lesion and post-lesion protocols consisted of stimulating the extremities (100 electrical pulses of 1 ms at 0.5 Hz) at low intensity (0.5 mA) and high intensity (5 mA), with at least 200 s of spontaneous recordings before each stimulation. However, in the present study, we consider only the electrophysiological data that were used to monitor the depth of anesthesia.
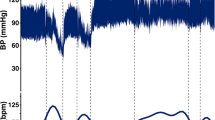
We continuously monitored the depth of anesthesia by the cortical recordings and the reflexes to noxious stimuli, in order to maintain the animals at stage III-3/III-416 (Figures 1a and b). The reflexes to noxious stimuli consisted of a pinch withdrawal reflex to manual stimulation of the forepaw and corneal reflex. The pinch withdrawal reflex is present in stage III-2 but not in stage III-3 and the corneal reflex is decreased in stage III-3, so these reflexes jointly offer a good behavioral measure of the level of anesthesia.16 The reflexes were evaluated at least once before the beginning of each protocol. As behavioral signs of activation, we used the pinch withdrawal reflex as well as the presence of whisker movements.16 As a neurophysiological sign of activation, we considered a desynchronized EEG with tonic firing (Figure 1c) for at least 20 min, which on average corresponds to about two physiological cycles of urethane.17 Whenever animals displayed electrophysiological and/or behavioral signs of activation, (Figure 1c) we delivered an additional dose of anesthesia (0.1–0.4 of the initial dose). Three transected animals were excluded from the analyses, because they received supplements of anesthesia at predetermined times after the transection. Statistical differences in anesthesia requirements between control and transected animals were evaluated using unpaired t-tests for continuous variables and Mann–Whitney U test for discrete variables. Differences were considered significant at P<0.05.

Cortical recordings were used to monitor the depth of anesthesia. (a–c) Representative 10-s recordings from the forepaw representation (upper traces in black) and the hindpaw representation (lower traces in gray) of the primary somatosensory cortex: (a) delta oscillations (1–4 Hz) typically observed in intact animals, (b) slow-wave activity (<1 Hz) typically observed after spinal cord transection(15), and (c) activation requiring additional anesthesia. Note the tonic neuronal firing in c.
We certify that all applicable institutional and governmental regulations concerning the ethical use of animals were followed during the course of this research.
Results
Control animals (n=9) survived 7.8±2.8 protocols after ‘sham’ injury (range 4–13). In order to maintain a stable level of anesthesia, we needed to provide supplemental doses of urethane (0.26±0.07 of the initial dose) every 2.3 protocols (range 1–3) after ‘sham’ injury. At the 7th protocol after ‘sham’ injury, on average the cumulative dose of urethane was 1.64±0.19 of the original dose (Figure 2).

Complete transection of the spinal cord decreases anesthestic requirements. Average cumulative doses—given as fraction of the initial dose of urethane—for control animals receiving ‘sham’ injury (n=9, black) and transected animals receiving spinal cord injury (n=11, gray). Error bars indicate standard deviations. Supplemental doses of urethane were given before the protocol indicated in the x-axis. Time between protocols is approximately 1 h.
Transected animals (n=11) survived 9.1±3.0 protocols after spinal cord injury (range 3–13), which was not significantly different from control animals (P=0.24). In order to maintain a stable level of anesthesia, we needed to provide smaller supplemental doses of urethane (0.15±0.06 of the original dose, P<0.0001) and at a lower rate compared with control animals, namely every 4.4 protocols (range 2–8) after spinal cord injury (P<0.0001). The cumulative dose was significantly lower in transected animals compared with control animals starting from the first protocol after spinal cord injury (P=0.0186), and the significance of this difference progressively increased in subsequent protocols (P=0.0011, P=0.0003, etc.). At the 7th protocol after spinal cord injury, on average the cumulative dose of urethane was only 1.13±0.14 of the original dose (Figure 2).
Discussion
The main result of the present work is that complete transection of the spinal cord at thoracic level immediately decreases anesthesia requirements in rats. The slower EEG activity we observed after spinal transection15 thus reflected a state of deeper anesthesia induced by the somatosensory deafferentation. These results were obtained in urethane-anesthetized rats and should be confirmed with more clinically relevant anesthetics. Nonetheless, we believe that the main conclusion of the present work will remain valid.
The sedative effects of pharmacologically blocking the spinal cord in patients are well documented. Tverskoy et al. (1994) (ref 1) showed that after spinal blockade at level L3-L4 with subarachnoid bupivacaine, the hypnotic dose of thiopental decreased by 36.2%. The same group later showed that midazolam hypnotic requirements decreased by 50% after intramuscular injection of bupivacaine and by 80% after epidural injection of bupivacaine at level L3-L4.4 Similar results were obtained by other groups: after spinal blockade at level T4-T6 with subarachnoid hyperbaric tetracaine, the induction dose of midazolam sedation decreased by 48.3%;3 epidural lidocaine doubled the duration until arousal from isoflurane anesthesia;2 and spinal anesthesia with hyperbaric bupivacaine produced significant sedative effects.5 These early results were later confirmed in three randomized, double-blind, placebo-controlled studies, which corroborated the sedative effects of epidural and spinal lidocaine anesthesia.6, 7, 8
Most of the clinical studies above suggested that the sedative effects of spinal anesthesia were likely due to somatosensory deafferentation. This idea was further supported by animal studies.9, 10, 11, 12, 13, 14 In particular, in a series of works in goats, Antognini and colleagues9, 10, 11, 12, 13 elegantly showed that pharmacological blockage of the spinal cord depressed the activating action of the forebrain reticular formation on cortical EEG. Depression of brainstem activity by epidural anesthesia was also confirmed in humans.18 The present study supports the deafferentation hypothesis and provides strong evidence against the classical criticism that spinal anesthetics could directly affect the brainstem through rostral diffusion in the cephalo-spinal fluid. In fact, there was no pharmacological agent that could diffuse in our transected animals. We therefore suggest that somatosensory deafferentation at the spinal level, independently of its origin, decreases the arousal level of the brain.
As follows from the above considerations, the most likely mechanism by which spinal cord injury could decrease anesthetic requirements is through an indirect depression of non-specific activating systems in the brainstem; by decreasing the tone of afferent somatosensory activity, spinal cord injury could affect the activity of the reticular formation,19, 20, 21 the locus coeruleus,22, 23, 24, 25, 26, 27 the raphe,28, 29, 30 and other brainstem and thalamic nuclei regulating cortical arousal. In agreement with this interpretation, the cerveau isolé (isolated forebrain) in vivo preparation displays the major EEG rhythms of sleep in absence of general anesthetics.31 Importantly, depression of non-specific activating systems in the brainstem after spinal cord injury is independent of the mechanism of action of urethane, which unspecifically increases the function of inhibitory receptors while decreasing the function of excitatory receptors.31 Similar results are thus expected with other anesthetics.
Somatosensory deafferentation is not the only possible cause of the reduction of anesthetic requirements. In fact, spinal cord injury disrupts not only the ascending somatosensory pathways, but also the descending pathways from central control centers to spinal sympathetic neurons. Loss of supraspinal control over the sympathetic nervous system could result in reduced overall sympathetic activity below the level of the injury and unopposed parasympathetic outflow through the intact vagal nerve. Moreover, spinal shock typically occurs during the acute phase following spinal cord injury, leading to a transitory suspension of function and reflexes below the level of the injury. All these factors could modify the normal pharmacokinetics of the anesthetic agents, possibly contributing to the reduction of anesthesia requirements we observed after transection of the spinal cord. Considering the disruption of descending pathways would be particularly important in the case of incomplete spinal lesions. In fact, loss of descending inhibition onto spared spinothalamic fibers can lead to hyperactivity of dorsal horn neurons originating from the spinothalamic tract,32, 33 and to supraspinal hyperexcitability in response to preserved spinothalamic inputs.34 The equilibrium between dorsal column deafferentation and spinothalamic hyperactivity is thus likely to have a critical role in determining the anesthetic requirements after incomplete spinal cord injuries.
Our results have some important clinical implications. In particular, we expect patients with spinal cord injuries—and more in general, patients with important degrees of sensory deafferentation—to require fewer anesthesias compared with patients with intact somatosensory system. This prediction was partly verified by Yoo et al.,35 who showed that anesthesia requirements decreased by 20–39% in patients with spinal cord injury undergoing surgery below the level of the injury. The same group, however, reported no changes in anesthesia requirements in patients with acute spinal injuries undergoing surgery at the level of the injury.36 These apparent differences could possibly be explained by acute and long-term compensatory mechanisms occurring in the brain in response to the deafferentation. Somatosensory deafferentation could also have a role in the complex spectrum of sleep disturbances observed after spinal cord injury.37, 38, 39, 40, 41, 42 In any case, our data are limited to the first few hours after spinal cord injury in a rat animal model with urethane anesthesia, and further investigation should be conducted in patients.
In conclusion, we showed that complete transection of the spinal cord immediately decreases anesthesia requirements in rats. To establish whether these results are relevant for patients with spinal cord injury will require further investigation.
References
Tverskoy M, Shagal M, Finger J, Kissin I . Subarachnoid bupivacaine blockade decreases midazolam and thiopental hypnotic requirements. J Clin Anesth 1994; 6: 487–490.
Inagaki Y, Mashimo T, Kuzukawa A, Tsuda Y, Yoshiya I . Epidural lidocaine delays arousal from isoflurane anesthesia. Anesth Analg 1994; 79: 368–372.
Ben-David B, Vaida S, Gaitini L . The influence of high spinal anesthesia on sensitivity to midazolam sedation. Anesth Analg 1995; 81: 525–528.
Tverskoy M, Shifrin V, Finger J, Fleyshman G, Kissin I . Effect of epidural bupivacaine block on midazolam hypnotic requirements. Reg Anesth 1996; 21: 209–213.
Gentili M, Huu PC, Enel D, Hollande J, Bonnet F . Sedation depends on the level of sensory block induced by spinal anaesthesia. Br J Anaesth 1998; 81: 970–971.
Hodgson PS, Liu SS . Epidural lidocaine decreases sevoflurane requirement for adequate depth of anesthesia as measured by the Bispectral Index monitor. Anesthesiology 2001; 94: 799–803.
Hodgson PS, Liu SS, Gras TW . Does epidural anesthesia have general anesthetic effects? A prospective, randomized, double-blind, placebo-controlled trial. Anesthesiology 1999; 91: 1687–1692.
Pollock JE, Neal JM, Liu SS, Burkhead D, Polissar N . Sedation during spinal anesthesia. Anesthesiology 2000; 93: 728–734.
Antognini JF, Atherley R, Carstens E . Isoflurane action in spinal cord indirectly depresses cortical activity associated with electrical stimulation of the reticular formation. Anesth Analg 2003; 96: 999–1003.
Antognini JF, Carstens E, Sudo M, Sudo S . Isoflurane depresses electroencephalographic and medial thalamic responses to noxious stimulation via an indirect spinal action. Anesth Analg 2000; 91: 1282–1288.
Antognini JF, Jinks SL, Atherley R, Clayton C, Carstens E . Spinal anaesthesia indirectly depresses cortical activity associated with electrical stimulation of the reticular formation. Br J Anaesth 2003; 91: 233–238.
Antognini JF, Saadi J, Wang XW, Carstens E, Piercy M . Propofol action in both spinal cord and brain blunts electroencephalographic responses to noxious stimulation in goats. Sleep 2001; 24: 26–31.
Antognini JF, Wang XW, Carstens E . Isoflurane action in the spinal cord blunts electroencephalographic and thalamic-reticular formation responses to noxious stimulation in goats. Anesthesiology 2000; 92: 559–566.
Eappen S, Kissin I . Effect of subarachnoid bupivacaine block on anesthetic requirements for thiopental in rats. Anesthesiology 1998; 88: 1036–1042.
Aguilar J, Humanes-Valera D, Alonso-Calvino E, Yague JG, Moxon KA, Oliviero A et al. Spinal cord injury immediately changes the state of the brain. J Neurosci 2010; 30: 7528–7537.
Friedberg MH, Lee SM, Ebner FF . Modulation of receptive field properties of thalamic somatosensory neurons by the depth of anesthesia. J Neurophysiol 1999; 81: 2243–2252.
Clement EA, Richard A, Thwaites M, Ailon J, Peters S, Dickson CT . Cyclic and sleep-like spontaneous alternations of brain state under urethane anaesthesia. PLoS One 2008; 3: e2004.
Doufas AG, Wadhwa A, Shah YM, Lin CM, Haugh GS, Sessler DI . Block-dependent sedation during epidural anaesthesia is associated with delayed brainstem conduction. Br J Anaesth 2004; 93: 228–234.
Peterson BW, Franck JI, Daunton NG . Changes in responses of medial pontomedullary reticular neurons during repetitive cutaneous, vestibular, cortical, and tectal stimulation. J Neurophysiol 1976; 39: 564–581.
Tamasy V, Koranyi L, Lissak K . Early postnatal development of wakefulness-sleep cycle and neuronal responsiveness: a multiunit activity study on freely moving newborn rat. Electroencephalogr Clin Neurophysiol 1980; 49: 102–111.
Faingold CL, Stittsworth Jr JD . Comparative effects of pentylenetetrazol on the sensory responsiveness of lateral geniculate and reticular formation neurons. Electroencephalogr Clin Neurophysiol 1980; 49: 168–172.
Cedarbaum JM, Aghajanian GK . Activation of locus coeruleus neurons by peripheral stimuli: modulation by a collateral inhibitory mechanism. Life Sci 1978; 23: 1383–1392.
Foote SL, Aston-Jones G, Bloom FE . Impulse activity of locus coeruleus neurons in awake rats and monkeys is a function of sensory stimulation and arousal. Proc Natl Acad Sci USA 1980; 77: 3033–3037.
Aston-Jones G, Bloom FE . Norepinephrine-containing locus coeruleus neurons in behaving rats exhibit pronounced responses to non-noxious environmental stimuli. J Neurosci 1981; 1: 887–900.
Elam M, Svensson TH, Thoren P . Locus coeruleus neurons and sympathetic nerves: activation by cutaneous sensory afferents. Brain Res 1986; 366: 254–261.
Hirata H, Aston-Jones G . A novel long-latency response of locus coeruleus neurons to noxious stimuli: mediation by peripheral C-fibers. J Neurophysiol 1994; 71: 1752–1761.
Aston-Jones G, Foote SL, Bloom FE . Low doses of ethanol disrupt sensory responses of brain noradrenergic neurones. Nature 1982; 296: 857–860.
Moolenaar GM, Holloway JA, Trouth CO . Responses of caudal raphe neurons to peripheral somatic stimulation. Exp Neurol 1976; 53: 304–313.
Springfield SA, Moolenaar GM . Differences in the responses of raphe nuclei to repetitive somatosensory stimulation. Exp Neurol 1983; 79: 360–370.
Waterhouse BD, Devilbiss D, Seiple S, Markowitz R . Sensorimotor-related discharge of simultaneously recorded, single neurons in the dorsal raphe nucleus of the awake, unrestrained rat. Brain Res 2004; 1000: 183–191.
Steriade M, Nunez A, Amzica F . Intracellular analysis of relations between the slow (<1 Hz) neocortical oscillation and other sleep rhythms of the electroencephalogram. J Neurosci 1993; 13: 3266–3283.
Brenowitz GL, Pubols LM . Increased receptive field size of dorsal horn neurons following chronic spinal cord hemisections in cats. Brain Res 1981; 216: 45–59.
Hains BC, Willis WD, Hulsebosch CE . Temporal plasticity of dorsal horn somatosensory neurons after acute and chronic spinal cord hemisection in rat. Brain Res 2003; 970: 238–241.
Yague JG, Foffani G, Aguilar J . Cortical hyperexcitability in response to preserved spinothalamic inputs immediately after spinal cord hemisection. Exp Neurol 2011; 227: 252–263.
Yoo K, Hwang J, Jeong S, Kim S, Bae H, Choi J et al. Anesthetic requirements and stress hormone responses in spinal cord-injured patients undergoing surgery below the level of injury. Anesth Analg 2006; 102: 1223–1228.
Yoo KY, Kim TS, Jeong CW, Kim SJ, Jeong ST, Jeong SW et al. Anaesthetic requirements and stress hormone responses in acute cord-injured patients undergoing surgery of the injured spine. Eur J Anaesthesiol 2009; 26: 304–310.
Adey WR, Bors E, Porter RW . EEG sleep patterns after high cervical lesions in man. Arch Neurol 1968; 19: 377–383.
Biering-Sorensen F, Biering-Sorensen M . Sleep disturbances in the spinal cord injured: an epidemiological questionnaire investigation, including a normal population. Spinal Cord 2001; 39: 505–513.
Bonekat HW, Andersen G, Squires J . Obstructive disordered breathing during sleep in patients with spinal cord injury. Paraplegia 1990; 28: 392–398.
Esteves AM, Mello MT, Squarcini CF, Lancellotti CL, Comparoni A, Tufik S . Sleep patterns over 15-day period in rats with spinal cord injury. Spinal Cord 2007; 45: 360–366.
McEvoy RD, Mykytyn I, Sajkov D, Flavell H, Marshall R, Antic R et al. Sleep apnoea in patients with quadriplegia. Thorax 1995; 50: 613–619.
Scheer FA, Zeitzer JM, Ayas NT, Brown R, Czeisler CA, Shea SA . Reduced sleep efficiency in cervical spinal cord injury; association with abolished night time melatonin secretion. Spinal Cord 2006; 44: 78–81.
Acknowledgements
This work was supported by FISCAM (Gobierno de Castilla-La Mancha) and Fondo de Investigación Sanitaria del Instituto de Salud Carlos III PI08/1852 PI08/1810 (Spain), co-funded by FEDER.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Foffani, G., Humanes-Valera, D., Calderon-Muñoz, F. et al. Spinal cord injury immediately decreases anesthetic requirements in rats. Spinal Cord 49, 822–826 (2011). https://doi.org/10.1038/sc.2011.11
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2011.11
