
Abstract
Study Design:
This was a retrospective observational study.
Objectives:
The objectives were to describe the prognosis of upper extremity function following cervical spinal cord injury (CSCI), and to identify prognostic factors for functional recovery.
Setting:
Spinal Injuries Center, Japan.
Methods:
Sixty patients with C3–4 CSCI without major bone injury participated in the study. Patients were treated nonsurgically and evaluated using the American Spinal Injury Association (ASIA) scales for the upper and lower extremities, their residual cervical motor functions, the modified Frankel grade and an upper extremity function scale. We compared the findings for the upper extremity function scale at 6 months with those for the residual cervical motor functions and modified Frankel grade obtained 3 days after injury.
Results:
Most patients with CSCI who could flex their hip and knee from a supine position (95%) or who showed some active elbow extension (86%) 3 days after their injury could use a spoon at 6 months. We compared patients who used their fingers at 6 months to those who could not, and observed significant differences in age and ASIA scores for the upper and lower extremities obtained 3 days after injury. A strong correlation was observed between the initial motor scores and the extent of functional recovery at 6 months.
Conclusion:
Hip and knee flexion from the supine position and elbow extension 3 days after injury significantly predicted a positive prognosis for upper extremity function. Younger age and higher ASIA motor scores obtained 3 days after injury were factors associated with neurological recovery.
Similar content being viewed by others

Introduction
The incidence of cervical spinal cord injury (CSCI) without major bone injury1 has increased dramatically in developed countries because of the increasing elderly population.2 Most patients with CSCI are elderly and present with spinal hyperextension predominantly at the C3–4 level, and with spinal cord compression resulting from spinal stenosis.3, 4, 5, 6 CSCI can cause sensory deficits, paresis or paralysis throughout the body, which often includes the upper limbs. The consequences of CSCI can be permanent and typically impair the patient’s quality of life, particularly when they involve the upper limbs. Anderson7 analyzed 681 responses from patients with spinal cord injury and found that regaining arm and hand function was most important to patients with quadriplegia. Thus, the recovery of upper-limb function after CSCI is important, as the upper limbs are a primary factor in enabling functional independence.7, 8
The prognosis for patients with CSCI should be known in order to standardize and to determine the goals of a rehabilitation program. The time course profiles and prognostic factors of upper extremity function recovery, however, remain unclear. Depending on the spinal level at which the injury occurs, CSCI can cause various degrees of paralysis. In addition, surgical intervention may affect the prognosis of paralysis. Previous studies that report the prognosis for upper extremity recovery, and data on the prognosis of participants with different injury levels, diagnosis or treatments were pooled and analyzed as a group.9, 10 Nevertheless, it is difficult to investigate the prognosis of paralysis in the upper extremities with different injury levels because the extent of paralysis can differ, depending on the level injured. Therefore, when evaluating paralysis in the upper extremities following CSCI, the injury level, type of injury and treatment should be uniform to allow meaningful analysis. To our knowledge, no study has used such an approach to investigate the prognosis of upper extremity paralysis in patients with CSCI at a specific spinal level. Here, we describe the prognosis of upper extremity function and identify the prognostic factors for functional recovery in the upper extremities following CSCI.
Materials and methods
A total of 526 patients with acute spinal injury were treated at the Spinal Injury Center in Fukuoka, Japan, between July 2005 and April 2011. All patients underwent dynamic cervical radiographs, computed tomography, magnetic resonance imaging and neurologic examination on admission. Because the purpose of this study was to assess functional recovery under similar pathological conditions, we selected patients with similar diagnoses and injury levels. Therefore, we retrospectively selected 60 of the 526 patients based on the following criteria: (1) admission within 3 days following injury, (2) observation for >6 months, (3) CSCI without major bone injury, (4) evidence of C3–4 cord injury with T2-weighted magnetic resonance images and (5) nonsurgical treatment. Minor bone injuries were considered a small avulsion fracture of the vertebral body, spinous process fracture or bone bruise in the vertebral body without noticeable vertebral collapse.1 Patients were excluded from the study if they experienced complications that required their transfer to another unit or hospital for treatment (for example, respiratory or heart failure). Evidence of preinjury cervical myelopathy was also an exclusion criterion. The 60 patients selected for the study included 54 men and 6 women, with a mean age of 63.2±10.7 years (median, 65 years; range, 34–82 years) at the time of injury.
For each patient, we documented both the upper extremity motor score (UEMS; range, 0–50) and lower extremity motor score (LEMS; range, 0–50) from the American Spinal Injury Association (ASIA) motor score system.11 In addition, we documented the modified Frankel grade,12, 13, 14 and the lowest level of residual cervical motor function based on the ASIA key muscle groups (C5, elbow flexors; C6, wrist extensors; C7, elbow extensors; C8, finger flexors; T1, finger abductors; Table 1).11 The lowest level of residual cervical motor function was defined as the most caudal level to which any observable movement with gravity eliminated could be attributed. In addition, we used our own upper extremity function scale that evaluated the ability to eat a meal independently (Table 2 and Figure 1). Patients were assigned to one of two groups based on their ratings in this scale and finger movement ability (A and B: unable to use their fingers; C-E: able to use their fingers). In the analysis, we performed further comparisons between these two groups. A spine surgeon and a physiotherapist, each with over 5 years of experience in practice, performed the neurological evaluations at 3 days and 6 months after the injury. The average follow-up period was 24.2 months (range, 7–60 months) after the injury. Our institutional review board approved this research project, and all subjects provided written informed consent before they were included in this retrospective study.

A brace used by patients with grade B (a), and a thick-handled fork used in patients with grade C (b). Scores were determined by the upper extremity function scale.
Statistical analysis
The relationships between the modified Frankel grade and the upper extremity function scale, and between the lowest level of residual cervical motor function and the upper extremity function scale, were assessed using χ2 tests. The relationship between age and the upper extremity function scale were assessed using Student’s t-test. The relationship between the ASIA motor score (UEMS and LEMS) and the upper extremity function scale were assessed using the Mann–Whitney test. Spearman’s correlation coefficients were used to assess the relationships between age, UEMS and LEMS at 3 days after injury, and to assess the relationship between age, UEMS, LEMS and the upper extremity function scale at 6 months. All statistical analyses were conducted using JMP software (version 8; SAS Institute, Cary, NC, USA); P-values of <0.05 were considered significant.
Results
The means for ASIA motor scores, UEMS and LEMS for all patients at 3 days after injury were 37.6±29.8, 13.3±12.0 and 24.3±19.8, respectively. The relationship between the modified Frankel grade at 3 days and the upper extremity function scale at 6 months is shown in Table 3. Out of 12 patients, 7 (58%) who were Frankel grade A, B1 or B2 at 3 days after injury were unable to bring their hand to their mouth (grade A) at 6 months. Only 4 out of 14 patients (29%) who were Frankel grade C1 at 3 days after injury were able to use their fingers (grades C and D) at 6 months, whereas 21 out of 22 patients (95%) who were Frankel grade C2 at 3 days were able to use their fingers (grades C and D) at 6 months. Thus, most of these patients with CSCI (95%) were able to use a spoon at 6 months if they were able to flex their hip and knee from a supine position 3 days after injury. Significant differences were found between those with Frankel grades C1 and C2 in their ability to use their fingers (P<0.001), which indicated that the ability to perform hip and knee flexion from a supine position at 3 days is an important factor for an important prognostic factor.
The relationship between the lowest level of residual cervical motor function at 3 days and the upper extremity function scale at 6 months is shown in Table 4. Only 7 out of 24 patients (29%) with residual C5 level functions at 3 days were able to use their fingers at 6 months, whereas 6 out of 7 patients (86%) with residual C7 level functions, and 18 out of 19 patients (95%) with residual C8 level functions, were able to use their fingers. Therefore, most of these patients (86%) could use a spoon at 6 months if they had some active elbow extension range at 3 days. By comparing finger movement ability, we observed a significant difference between the residual level of cervical motor functions at the C6 level or higher and at the C7 level or lower (P<0.001), indicating that elbow extension at 3 days after injury is an important prognostic factor.
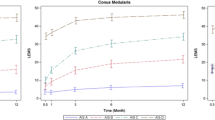
Factors affecting upper extremity functional recovery are shown in Table 5. We observed significant differences for the age at injury, the UEMS and the LEMS determined 3 days after injury between patients who were unable (grades A and B) or able to use their fingers (grades C–E) at 6 months after injury. This indicates that younger patients and patients with higher UEMS and LEMS at 3 days significantly improved their finger movement ability. Spearman’s rank correlation coefficients revealed a weak correlation (ρ=−0.25) between age at 3 days and the upper extremity function scale at 6 months (Figure 2a), a strong correlation (ρ=0.74) between UEMS at 3 days and the upper extremity function scale at 6 months (Figure 2b) and a strong correlation (ρ=0.81) between LEMS at 3 days and the upper extremity function scale at 6 months (Figure 2c).

The correlation between age at injury and the upper extremity function scale (a), between UEMS at 3 days and the upper extremity function scale (b) and between LEMS at 3 days and the upper extremity function scale (c).
Seven patients were unable to raise their hands to their mouth (grade A) at 6 months. These patients required full support to perform this movement because they had severe paralysis (four patients), severe contracture with pain at the shoulder (three patients) or dementia (two patients). One of the patients had a combination of severe paralysis, severe contracture with pain and dementia.
Discussion
We observed the potential for functional recovery in patients with CSCI without major bone injury following nonsurgical treatment.2, 6 Nevertheless, few studies document the prognosis for paralysis, especially for the upper extremities.9, 10 Ishida and Tominaga9 reported that a favorable prognosis for upper extremity recovery can be predicted following nonsurgical treatment in patients with acute central cervical cord injury. Our study demonstrated that >95% of patients with CSCI who were able to flex their hip and knee from a supine position at 3 days after injury were able to use a spoon at 6 months. Furthermore, >86% of our patients with CSCI who had some active elbow extension range at 3 days could use a spoon at 6 months. We suggest that these results can aid physicians and therapists in setting rehabilitation goals for patients with CSCI.
Many studies report positive predictors for lower extremity functional recovery in patients with CSCI, but not for upper extremity functional recovery.10, 15 In previous studies, severe initial neurological damage and an older age were associated with a poor functional outcome.9, 16, 17 Our study showed that a younger age and a high UEMS and LEMS at 3 days after injury predicted improved upper extremity functions. Our findings are similar to those from other studies in that the total ASIA motor score was predictive of outcomes.9, 16, 17 We, however, extend the previous findings and report that both initial UEMS and LEMS can predict upper extremity function. These results are of interest because, to our knowledge, no previous study reports a relationship between initial upper extremity paralysis and its functional recovery. We found a strong correlation between UEMS at 3 days and functional recovery of upper extremities at 6 months. Our results indicate that upper extremity motor recovery might be similar to that for the lower extremities with regard to the recovery from pyramidal tract injury.
We included only patients with C3–4 CSCI without major bone injury in the present study for three reasons. First, these patients were not treated surgically.2, 6 Second, these patients allowed a more simple assessment of finger function as only paralysis resulting from spinal cord damage was considered, rather than the injured nerve root. Finally, because CSCI without major bone injury occurs predominantly at C3–4, this CSCI patient subgroup is larger than the other subgroups with injuries at other spinal levels. Thus, CSCI without major bone injury at C3–4 was considered an appropriate criterion for evaluating upper extremity function.
Patients with CSCI with C3–4 injury would be expected to be able to raise their hand to their mouth because deltoid and bicep muscle functions are usually preserved, at least to some extent. We observed, however, that 7 out of 60 patients were unable to raise their hand to their mouth at 6 months, and these patients required full support during the movement. Although rehabilitation for these patients began as soon as possible following injury, three patients with a grade A had severe contracture in their shoulders that was accompanied by pain. Diong et al.18 reported that the incidence of shoulder contracture 1 year after spinal cord injury was 43%. This type of contracture is associated with CSCI, and injury at C3–4 might result in shoulder pain, as well as muscle weakness.
The present study has some limitations. First, this was a retrospective study and was based on a small number of patients. Second, the degree of paralysis differs according to the spinal level of the injury, and we did not examine all levels of CSCI. Therefore, further study is needed to evaluate injury at other spinal levels.
Conclusions
We observed upper extremity functional recovery in patients with CSCI without major bone injury, and without surgical treatment. Our study demonstrates that hip and knee flexion from a supine position, and some observable elbow extension at 3 days after the injury, predicted a positive prognosis for upper extremity function at 6 months after injury. A younger age and higher UEMS and LEMS scores at 3 days were also factors affecting functional recovery.
Data archiving
There were no data to deposit.
References
Maeda T, Ueta T, Mori E, Yugue I, Kawano O, Takao T et al. Soft-tissue damage and segmental instability in adult patients with cervical spinal cord injury without major bone injury. Spine 2012; 37: E1560–E1566.
Kawano O, Ueta T, Shiba K, Iwamoto Y . Outcome of decompression surgery for cervical spinal cord injury without bone and disc injury in patients with spinal cord compression: a multicenter prospective study. Spinal Cord 2010; 48: 548–553.
Harrop JS, Sharan A, Ratliff J . Central cord injury: pathophysiology, management, and outcomes. Spine J 2006; 6: 198S–206S.
Koyanagi I, Iwasaki Y, Hida K, Akino M, Imamura H, Abe H . Acute cervical cord injury without fracture or dislocation of the spinal column. J Neurosurg 2000; 93: 15–20.
Shimada K, Tokioka T . Sequential MRI studies in patients with cervical cord injury but without bony injury. Paraplegia 1995; 33: 573–578.
Okada S, Maeda T, Ohkawa Y, Harimaya K, Saiwai H, Kumamaru H et al. Does ossification of the posterior longitudinal ligament affect the neurological outcome after traumatic cervical cord injury? Spine 2009; 34: 1148–1152.
Anderson KD . Targeting recovery: priorities of the spinal cord-injured population. J Neurotraum 2004; 21: 1371–1383.
Snoek GJ, IJzerman MJ, Hermens HJ, Maxwell D, Biering-Sorensen F . Survey of the needs of patients with spinal cord injury: impact and priority for improvement in hand function in tetraplegics. Spinal Cord 2004; 42: 526–532.
Ishida Y, Tominaga T . Predictors of neurologic recovery in acute central cervical cord injury with only upper extremity impairment. Spine 2002; 27: 1652–1658.
Marino RJ, Burns S, Graves DE, Leiby BE, Kirshblum S, Lammertse DP . Upper- and lower-extremity motor recovery after traumatic cervical spinal cord injury: an update from the national spinal cord injury database. Arch Phys Med Rehab 2011; 92: 369–375.
Association ASI. International Standards for Neurological Classification of Spinal Cord Injury, Revised 2002. American Spinal Injury Association: Chicago, IL. 2002.
Frankel HL, Hancock DO, Hyslop G, Melzak J, Michaelis LS, Ungar GH et al. The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. I. Paraplegia 1969; 7: 179–192.
Ueta TSK, Shirasawa K . Cervical cord injuries with no evidence of bony spine damage. Spine Spinal Cord 1997; 10: 581–590 (in Japanese).
Fukuda F, Ueta T . Prediction of prognosis using modified Frankel classification in cervical spinal cord injured patients. JJRM 2001; 38: 29–33 (in Japanese).
Marino RJ, Ditunno JF Jr., Donovan WH, Maynard F Jr . Neurologic recovery after traumatic spinal cord injury: data from the Model Spinal Cord Injury Systems. Arch Phys Med Rehab 1999; 80: 1391–1396.
Tow AM, Kong KH . Central cord syndrome: functional outcome after rehabilitation. Spinal Cord 1998; 36: 156–160.
Dai L, Jia L, Ni B, Yuan W, Liu H, Hou T et al. Diagnosis and treatment of acute central cervical cord injury. Chin Med J 1998; 111: 351–353.
Diong J, Harvey LA, Kwah LK, Eyles J, Ling MJ, Ben M et al. Incidence and predictors of contracture after spinal cord injury—a prospective cohort study. Spinal Cord 2012; 50: 579–584.
Acknowledgements
We thank Mr R Watanabe, OT, and Mr K Iwahashi, OT, for their suggestions with regard to rehabilitation of the upper extremities.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Hayashi, T., Kawano, O., Sakai, H. et al. The potential for functional recovery of upper extremity function following cervical spinal cord injury without major bone injury. Spinal Cord 51, 819–822 (2013). https://doi.org/10.1038/sc.2013.90
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2013.90
Keywords
This article is cited by
-
Traumatic cervical spinal cord injury after cervical laminoplasty for ossification of posterior longitudinal ligament: a case series
Spinal Cord (2022)
-
A prediction model of functional outcome at 6 months using clinical findings of a person with traumatic spinal cord injury at 1 month after injury
Spinal Cord (2020)
-
Progression of local kyphosis after conservative treatment for compressive cervical spine fracture with spinal cord injury
Journal of Orthopaedic Surgery and Research (2019)
-
The neurological outcome of radiotherapy versus surgery in patients with metastatic spinal cord compression presenting with myelopathy
Archives of Orthopaedic and Trauma Surgery (2018)
-
Risk factors for severe dysphagia in acute cervical spinal cord injury
Spinal Cord (2017)
