
Abstract
Study design:
Case–control study.
Objectives:
To assess serum myostatin levels, bone mineral density (BMD), appendicular skeletal muscle mass (ASMM) and serum sclerostin levels in chronic spinal cord injured (SCI) patients and healthy controls.
Setting:
SCI centre in Italy.
Methods:
Blood samples, whole-body bioelectrical impedance analysis and BMD measurement with the ultrasound technique at the calcaneus level were taken from patients suffering from chronic SCI (both motor complete and incomplete) and healthy control subjects.
Results:
A total of 28 SCI patients and 15 healthy controls were enrolled. Serum myostatin levels were statistically higher (P<0.01) in SCI patients compared with healthy controls. Similar results were found comparing both the motor complete and the motor incomplete SCI subgroups to healthy controls. Serum sclerostin was significantly higher in patients with SCI compared with healthy controls (P<0.01). BMD, stiffness and mean T-score values in SCI patients were significantly lower than those in healthy controls. Serum myostatin concentrations in the motor complete SCI subgroups correlated only with serum sclerostin levels (r2=0.42; P=0.001) and ASMM (r2=0.70; P=0.002) but not in healthy controls.
Discussion:
Serum myostatin and serum sclerostin are significantly higher in chronic SCI patients compared with healthy controls. They are potential biomarkers of muscle and bone modifications after SCI. This is the first study reporting an increase in serum myostatin in patients suffering from chronic SCI and a correlation with ASMM.
Similar content being viewed by others

Introduction
Both animal and human models show that unloading is the main determinant of osteoporosis after spinal cord injury (SCI), a condition known to increase the risk of fractures, mainly at distal femur and proximal tibia.1 The Wingless and Int signaling pathway has been identified as one of the key regulators of mechanical load responses2, 3, 4, 5 that is involved in osteoporosis after SCI. Moreover, sclerostin, a powerful selective inhibitor of Wingless and Int signaling produced by osteocytes, is able to induce a reduction in osteoblast activity and proliferation ultimately resulting in the loss of bone mass.6 Recently, Morse et al.6,7 found a strong correlation between bone mineral density (BMD) and serum sclerostin in patients with SCI, suggesting its possible use as a biomarker complementary or in alternative to dual X-ray absorptiometry (DXA), to assess osteoporosis and to monitor its treatment in patients with chronic SCI.
Pathological muscle modifications after SCI can be as severe as those observed at the bone level, with a relevant impact on disability and comorbidities.8 However, research about muscle modifications after SCI is still at its beginnings, and the pathophysiology, diagnosis and treatment of these changes are still unclear.9 Recently, the evidence of a biochemical cross-talk between the muscle and bone has been postulated, overtaking the previous hypothesis of a simple mechanical correlation between these two tissues.10, 11 In vitro studies suggest the possible existence of a biunivocal cross-talk between the bone and muscle, indicating that factors produced by osteocytes could target muscle and that muscle-derived soluble factors could target bone.12 It is likely that, although osteocytes and sclerostin are responsible for cross-talk between bone and muscle, satellite cells (at skeletal muscle level) could have a role in the opposite way.12, 13, 14, 15 Myostatin is a powerful inhibitor of overall muscle differentiation and growth both in vivo and in vitro.16 As the inhibition of myostatin pathway facilitates muscle growth, myostatin could be used as a possible biomarker to monitor the evolution of muscular modifications in SCI patients and could also represent a potential therapeutical target.14, 17 However, to date, possible modifications of serum myostatin levels in SCI patients have not been described yet.
In light of these considerations, the aim of our work is to assess, in a population of chronic SCI patients, the serum myostatin concentration. Secondarily, assuming the previously described biochemical cross-talk between the bone and muscle tissue and the key role of osteocytes, we investigated a possible correlation between serum myostatin levels, serum sclerostin levels, appendicular skeletal muscle mass (ASMM) and BMD in this population.
Materials and methods
Subjects
Twenty-eight patients suffering from chronic SCI were consecutively enrolled from the Physical and Rehabilitation Unit of the AOU ‘Maggiore della Carità’ in Novara (Italy).
Demographical data are summarized in Table 1. Inclusion criteria were the following: (1) SCI; (2) a grade from A to C on the American Spinal Injury Association (AIS) Impairment Scale18; (3) neurological level of lesion from C5 to T12; (4) age>18; and (5) time from lesion >2 years (24 months). The exclusion criteria were as follows: concomitant diabetes; oral anticoagulation; other concomitant chronic neurological pathologies (of central and/or peripheral nervous system and/or neuromuscular diseases), use of drugs acting on the bone (bisphosphonates, corticosteroids, lithium, anticonvulsant drugs, parathyroid hormone analogs, estrogens, calcium and vitamin D) and muscle (statins) metabolism. Moreover, 15 healthy controls were enrolled and the inclusion criteria were the following: absence of SCI and/or any other neurological pathologies; absence of musculoskeletal pathologies; absence of functional limitations (such as gait limitation); age>18; control subjects should not have any intense physical activity at least in the 24 h before serum sample collection. The exclusion criteria were the same as those of patients suffering from SCI. All study participants signed informed consent forms and the Institutional Review Board approved the study, which was conducted in accordance with the Declaration of Helsinki guidelines.
Study procedure
All patients at baseline underwent a physical examination by a trained physician and sensory–motor impairment was determined using the AIS impairment scale.19, 20 According to the AIS score, patients were divided in two groups: complete motor (AIS A, B) and incomplete motor (AIS C).
For patients with SCI, the level of disability was measured with the SCIM-III scale.21 After enrollment, all patients underwent blood sample and BMD measurement in the same morning.
Biochemical markers, appendicular muscle and bone mass
Blood samples were collected at the same hour in the morning in fasting conditions. Samples were centrifuged for 15 min at 3000 r.p.m. at 4 °C and stored at −80 °C until final analysis.
Serum plasma iodized calcium, phosphate, creatinine, 1–84 parathyroid hormone (PTH), 25(OH) Vitamin D (25(OH)D), insulin-like growth factor I, C reactive protein, osteocalcin and Beta-Crosslaps (CTX) were measured in the laboratory analysis of our Hospital.
Myostatin was quantified by the Elisa assay (MyBioSource, San Diego, CA, USA, MBS703668; normal range: 0.625–20 ng ml−1; minimum detectable dose 0.312 ng ml−1). Serum sclerostin was measured using the SOST Elisa Kit (Biomedica Gruppe, Vienna, Austria; normal range: 0–240 pmol l−1; detection limit: 2.6 pmol l−1 and a unit conversion of 1 pg ml−1=0.044 pmol l−1).
Whole-body tetrapolar bioelectrical impedance analysis (BIA) was performed using an alternating sinusoidal electric current of 400 mA at a single operating frequency of 50 kHz (BIA 101 Anniversary Sport Edition—ASE—Akern Srl; Florence, Italy). The device's precision was 1% for resistance (Rz) and 5% for reactance (Xc). BIA was performed with subjects supine with their limbs slightly away from their body, after an overnight fast, and bladder voiding. To avoid inter-observer errors, all BIA measurements were taken by the same investigator (MI). Active electrodes (BIATRODES Akern Srl; Florence, Italy) were placed on the right side on conventional metacarpal and metatarsal lines, recording electrodes in standard positions at the right wrist and ankle.22 All resistance measurements were normalized for stature (height in centimeters squared/Rz) to obtain the resistive index (RI).
Appendicular muscle mass (ASMM) was obtained using a validated equation.23 Then, the ASMM index (ASMMI) value was obtained using the following calculation: ASMM/height2.24
BMD of patients and healthy controls was measured with calcaneus ultrasonography (Achilles Express 2001 GE Medical System, Lunar Corporation—Madison, WI, USA), obtaining data about T-score and stiffness.
Statistical analysis
Statistical analyses were performed using the GraphPad 4 package, version 4.0 (GraphPad Software, Inc., San Diego, CA, USA). Because of the small sample size, we assumed a non-gaussian distribution of the considered variables. After enrollment, patients were divided into two subgroups, depending on motor completeness of the lesion (complete and incomplete). Differences between single variables in different groups were evaluated with the Mann–Whitney U-test. A type I error level of 0.05 was chosen. The Bonferroni correction for multiple comparisons was applied considering three variables, which resulted in a new alpha-error level of 0.017. Relationships between serum myostatin values and the other variables were analyzed with linear regression using Pearson’s correlation coefficients. Regression lines were compared using confidence intervals. A P<0.017 was considered statistically significant.
Results
Demographic characteristics of SCI patients with SCI and healthy controls are resumed in Table 1. Patients with SCI showed statistically significant differences regarding smoke, age and history of previous fractures at any site compared with healthy controls, whereas all the other demographical variables showed no statistical difference.
Serum myostatin levels were statistically higher (P<0.01) in patients suffering from SCI compared with healthy controls (Figure 1a). Similar results were found comparing both patients with motor complete and motor incomplete SCI to healthy controls (Figure 1a).

Differences between serum myostatin (a) and sclerostin (b) in all groups. Data are presented as mean±s.d. *P<0.017 SCI Tot vs CT; **P<0.017 SCI complete vs CT; ***P<0.017 SCI incomplete vs CT; #P<0.017 SCI complete vs SCI incomplete. SCI, spinal cord Injured; CT, healthy controls.
Serum sclerostin was significantly higher in SCI patients compared with healthy controls (P<0.01) as shown in Figure 1b.
Regarding other biochemical variables, parathyroid hormone and C reactive protein serum values showed statistically significant differences between the two groups (Table 2). However, the mean values in both groups were in the normality range. 25(OH)D serum levels were significantly higher in healthy controls compared with patients with SCI. However, the mean value in the control group was far from the normality level and only 20% of healthy controls showed values of 25(OH)D higher than 30 ng ml−1. On the contrary, 50% of SCI patients showed 25(OH)D values<10 ng ml−1.
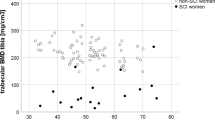
BMD, stiffness and mean T-score values in SCI patients were significantly lower than those in healthy controls. Interestingly, we also observed a statistically significant difference between the motor complete and incomplete subgroups regarding these variables.
Serum myostatin concentrations in the motor complete SCI subgroup (n=22) correlated only with serum sclerostin levels (r2=0.42; P=0.001; Figure 2a). None of the other instrumental, biochemical or demographical variables considered showed any correlation with serum myostatin concentrations.

(a) Correlation between serum myostatin and serum sclerostin levels in motor complete SCI subgroup (n=22)—r2=0.42; P=0.0012. (b) Correlation between serum myostatin and ASMMI in motor complete SCI subgroup (n=10)—r2=0.70; P=0.002. SCI, spinal cord injured; ASMMI, appendicular skeletal muscle mass index.23, 24
Thus, unlike previous studies on bone biomarkers like sclerostin in SCI patients,7 any correction of serum myostatin for any variable considered in this study was needed.
Moreover, 10 patients with motor complete SCI (AIS A and B) and seven healthy controls performed whole-body BIA evaluation. Mean ASSMI in patients with SCI was inferior to those of healthy subjects (7.29±1.97 vs 8.01±0.95 Kg m−2). This difference was not statically significant, but the sample size of this subgroup was extremely small. We found a strong correlation between serum myostatin concentrations and ASMMI in patients with complete SCI (r2=0.70; P=0.002) but not in healthy controls, as shown in Figure 2b.
Discussion
Our data point out a statistically significant difference in serum myostatin concentration in SCI patients compared with healthy controls; thus, SCI patients, considering both motor complete and incomplete subgroups, showed higher serum values of myostatin compared with healthy controls. To our knowledge, this is the first study investigating serum myostatin levels in SCI patients.
Similarly, we observed a significative increase in serum sclerostin levels in chronic SCI patients compared with healthy subjects, confirming findings described in a previous study.7 Moreover, the differences at the bone tissue level between SCI patients and healthy controls were confirmed also by a huge statistically significant reduction in BMD measured at the calcaneus level between these two groups. Finally, serum myostatin correlated only with serum sclerostin (r2=0.42) and ASMMI (r2=0.70) in SCI but not in healthy controls. Circulating biomarkers have been advocated as a useful surrogate measure for diagnosis, therapeutic monitoring and research purposes, considering that they can be easily and noninvasively obtained and that they have a low economic cost.25 This is the case of BMD measured with the DXA technique, which is the gold standard for osteoporosis, but in a condition like SCI, as we will discuss later, can present some important technical and accuracy issues.1, 2
Myostatin and muscular modifications
In patients suffering from SCI, the main feature of underlesional muscle tissue is the atrophy of muscle fibers, in conjunction with a transformation of their fiber type, leading to a reduction in slow-twitch fibers (type I) and an increase in fast-twitch fibers (type IIA and IIX).26 Mohr et al.27 showed that conversion of quadriceps myosin to myosin heavy chain IIA was almost complete by 3 years in SCI patients. These modifications, and particularly the severe muscle atrophy in chronic complete SCI, are a major contributor to comorbidity risk factors such as diabetes, obesity, lipid disorders and cardiovascular diseases.8
Myostatin is a member of the transforming growth factor superfamily, mainly expressed in satellite cells and is a powerful inhibitor of muscular regulating factors and overall muscle differentiation and growth both in vivo and in vitro.16 Our findings suggest that, in SCI patients, independently from the level and completeness of the lesion, myostatin serum levels are significantly higher than those in healthy controls; this could partially explain the severe pathological muscular modifications observed.
Being SCI the extreme pathological unloading condition in humans, our results are intriguing as myostatin, a factor selectively produced by satellite cells in the muscle microenvironment, is an attractive candidate biomarker to monitor the muscular modifications in these patients as well as a possible pharmacological target to prevent muscle loss not only after SCI but also in other pathological conditions (that is, prolonged bed immobilization or absence of gravity). To date, bimagrumab, a selective anti-type II activin receptor monoclonal antibody preventing myostatin activity, has shown to be effective in humans with inclusion body myositis28, possibly becoming in the near future a therapeutic option to prevent muscular modifications in SCI and other pathological conditions.
Previous studies showed a strong relation existing between unloading and muscle cross-sectional area reduction in both the acute29 and sub-acute30 phases of SCI. Moreover, myostatin messenger RNA expression has been investigated in different conditions like HIV and chronic stroke, showing a significant increase compared with healthy subjects. At present time, serum myostatin concentrations after SCI in humans have not been published, and only few studies, with contrasting results, investigated this issue on animal models.31, 32 To date, only one study investigated myostatin messenger RNA expression in muscular biopsies in patients with chronic SCI, finding a reduction of 46% compared with healthy subjects. However, the authors did not find a statistical difference regarding myostatin concentration measured by western blotting.33 The main difference with our work is that, in previous studies, the authors measured myostatin expression and concentration at the muscular microenvironment level, without evaluating serum myostatin concentrations. Thus, the differences found by Léger et al. regarding myostatin concentration and expression at the local level could not reflect those at the circulating level. Our results integrate these molecular data, showing that myostatin concentration is increased in SCI patients even at the systemic level if compared with healthy controls, and this difference is similar in both motor complete and incomplete patients. Moreover, Léger et al. had a smaller sample size than ours, and, the time from lesion ranged from 3 months to 30 years, whereas in our study we only enrolled patients 24 months from SCI. This could have determined an enrollment bias, putting on the same level acute and chronic patients, considering that Castro et al. previously observed a peak of skeletal muscle mass reduction only 6 months after SCI.30
As the inhibition of the myostatin pathway could be a key target to facilitate muscle growth, our data support the hypothesis that myostatin could be a possible biomarker to monitor the evolution of muscular modifications in SCI patients and a potential target for therapeutic purposes.
Sclerostin
In our study, both motor complete and incomplete SCI patients showed statistically significant higher values of serum sclerostin compared with healthy subjects. Our results are somehow conflicting with those obtained by Morse et al.,6 which is the only study in literature investigating serum sclerostin levels in patients suffering from SCI. They proposed a model in which serum sclerostin is increased in the acute and sub-acute phase (up to 6 months) after SCI and even reduced in the chronic phase compared with healthy controls.6 Morse et al. enrolled a larger population than ours; however, considering the complete SCI subgroup only, the sample size was similar. Moreover, in our opinion, the two study populations show some differences regarding both age (40.5 years vs 55.8 years) and time from lesion (8 years vs 22 years). Furthermore, the age of control group was different in the two studies (28.4 years vs 61.7 years). These could be, in our opinion, relevant differences between our study and that by Morse et al.6 considering that sclerostin has been demonstrated to increase with age34 and that the way authors performed age correction has not been clearly explained. However, even though the differences found in our study could lie in the younger age of patients enrolled (both SCI and healthy controls), the results showed no correlation between serum sclerostin and age. Nevertheless, our data could have important therapeutic implications, suggesting that anti-sclerostin antibodies35, 36, 37 could be a valid option even in chronic phase after SCI, as serum sclerostin levels are still elevated during this phase.
BMD
Patients with SCI enrolled in our study showed statistically significant lower BMD values than healthy controls. This difference was present in both complete and incomplete patients, with a lesser magnitude in the second subgroup. Our data are similar to those previously obtained by Warden et al.38 with ultrasound technique and Jiang et al.39
DXA measurement of BMD is the gold standard for the diagnosis of osteoporosis.40 However, this technique could not be so easy to perform in SCI patients because of several factors limiting correct scan positioning (paresis, contractures, spasms and amputation) or the presence of scan artifacts due to heterotopic ossifications, joint replacement or metal rods.2 Moreover, fracture risk prediction by bone density category after SCI has not well been defined yet, and fractures are most common at distal sites (knee and tibia), which are not routinely included in standard clinical DXA scans.
For these reasons, we choose to measure BMD with the heel quantitative ultrasound technique, being easier (patients can sit on their wheelchair during measurement) and faster compared with DXA. Finally, the quantitative ultrasound technique has shown an excellent reproducibility and a strong correlation with osteoporotic fracture risk at both vertebral and femoral site.2, 41, 42, 43
Correlations
As emerges in Figures 2a and b, serum myostatin positively correlated with serum sclerostin and ASMMI. Regarding serum myostatin and sclerostin we choose to perform the correlation only in the subgroup of patients suffering from motor complete SCI because of the low number of patients in the motor incomplete group, finding a good correlation between these two variables (r2=0.42; P=0.001). Our data about the supposed correlation between sclerostin and myostatin should be taken cautiously, considering the small sample size. However, assuming the hypothesis of a biochemical cross-talk between the bone and muscle tissue,12 which could partially explain the mechanisms underlying the observed modifications in these two tissues after SCI, myostatin could be one of the responsible of this cross-talk by the muscle side. However, this is just an hypothesis, and further studies are needed to deeply investigate this possible cross-talk in which other mediators could be involved.
Interestingly, serum myostatin concentrations correlated also with ASMMI. Considering the low number of patients performing this evaluation (n=10), the correlation found was strong (r2=0.70; P=0.002), and this correlation was absent in healthy controls. As previously noted, this finding should be taken cautiously, considering the small sample size; however, it shows that serum myostatin could be a useful marker to monitor skeletal muscle modifications in SCI patients. This consideration is also supported by the fact that, similarly to bone tissue, other muscular imaging techniques to quantify muscle mass like DXA may have underestimated in the past the degree of muscle atrophy associated with SCI.44, 45 However, previous studies showed that skeletal fat-free muscle mass from magnetic resonance imaging and from DXA were very strongly related and can accurately predict thigh skeletal muscle mass in men with long-term, complete SCI but only if appropriate regression equations are developed.45 However, at present time, equations specific to patients suffering from SCI have not been developed yet.
Study limitations
This study has some limitations. First, the population sample size was relatively small, mainly for the motor incomplete group. Another limit of this study is that we do not have data about the muscle microenvironment to correlate with those obtained at the circulating level.
Conclusions
Muscular modifications in chronic SCI patients are a growing issue, considering their impact on vascular risk factors (that is, diabetes, obesity, lipid disorders and cardiovascular disease) in these patients and the overall disability and health-care costs.9 It should be remembered that cardiovascular diseases are becoming the primary cause of death among SCI patients.46 Moreover, in light of all the research to improve neural repair after SCI, it is imperative that we understand whether deleterious musculoskeletal adaptations after chronic SCI can be reversed.47 Then, in contrast with bone tissue modifications after SCI, those at the muscle level, and the underlying pathological mechanisms, have been little analyzed.
In this study, according to the previous hypothesis of a biochemical more than functional relation between the bone and muscle, we showed that serum myostatin, a powerful inhibitor of muscle proliferation selectively produced by satellite cells, is significantly higher in patients suffering from chronic SCI compared with healthy controls, finding also a strong correlation between serum myostatin concentrations and ASMMI in SCI patients but not in healthy controls. Moreover, we confirmed previously published data about serum sclerostin in SCI patients, and, we also found out a correlation between serum sclerostin and myostatin, giving some evidence about a possible biochemical cross-talk involving osteocytes and sclerostin from the bone side and satellite cells and myostatin on the muscle side.
In conclusion, our results are encouraging, suggesting myostatin as a potential biomarker of muscular modifications and a potential therapeutic target to prevent these pathological modifications not only in SCI patients but also in other pathological unloading conditions.
Data archiving
There were no data to deposit.
References
Morse LR, Battaglino RA, Stolzmann KL, Hallett LD, Waddimba A, Gagnon D et al. Osteoporotic fractures and hospitalization risk in chronic spinal cord injury. Osteoporos Int 2009; 20: 385–392.
Morse LR, Geller A, Battaglino RA, Stolzmann KL, Matthess K, Lazzari AA et al. Barriers to providing dual energy x-ray absorptiometry services to individuals with spinal cord injury. Am J Phys Med Rehabil 2009; 88: 57–60.
Khosla S . Minireview: the OPG/RANKL/RANK system. Endocrinology 2001; 142: 5050–5055.
Hauschka PV, Lian JB, Cole DE, Gundberg CM . Osteocalcin and matrix Gla protein: vitamin K-dependent proteins in bone. Physiol Rev 1989; 69: 990–1047.
Patterson-Buckendahl P . Osteocalcin is a stress-responsive neuropeptide. Endocr Regul 2011; 45: 99–110.
Morse LR, Sudhakar S, Danilack V, Tun C, Lazzari A, Gagnon DR et al. Association between sclerostin and bone density in chronic spinal cord injury. J Bone Miner Res 2012; 27: 352–359.
Morse LR, Sudhakar S, Lazzari AA, Tun C, Garshick E, Zafonte R et al. Sclerostin: a candidate biomarker of SCI-induced osteoporosis. Osteoporos Int 2013; 24: 961–968.
Garshick E, Kelley A, Cohen SA, Garrison A, Tun CG, Gagnon D et al. A prospective assessment of mortality in chronic spinal cord injury. Spinal Cord 2005; 43: 408–416.
Carda S, Cisari C, Invernizzi M . Sarcopenia or muscle modifications in neurologic diseases: a lexical or patophysiological difference? Eur J Phys Rehabil Med 2013; 49: 119–130.
Schoenau E . From mechanostat theory to development of the ‘Functional Muscle-Bone-Unit’. J Musculoskelet Neuronal Interact 2005; 5: 232–238.
Cianferotti L, Brandi ML . Muscle-bone interactions: basic and clinical aspects. Endocrine 2014; 45: 165–177.
Mo C, Romero-Suarez S, Bonewald L, Johnson M, Brotto M . Prostaglandin E2: from clinical applications to its potential role in bone- muscle crosstalk and myogenic differentiation. Recent Pat Biotechnol 2012; 6: 223–229.
Brotto M . Editorial: welcome to our Recent Patents on Biotechnology Special Edition on skeletal muscle diseases!. Recent Pat Biotechnol 2012; 6: 155–156.
Brotto M, Abreu EL . Sarcopenia: pharmacology of today and tomorrow. J Pharmacol Exp Ther 2012; 343: 540–546.
Huang J, Hsu YH, Mo C, Abreu E, Kiel DP, Bonewald LF et al. METTL21C is a Potential Pleiotropic Gene for Osteoporosis and Sarcopenia Acting through the Modulation of the NFkappaB Signaling Pathway. J Bone Miner Res 2014; 29: 1531–1540.
Marimuthu K, Murton AJ, Greenhaff PL . Mechanisms regulating muscle mass during disuse atrophy and rehabilitation in humans. J Appl Physiol 2011; 110: 555–560.
Lang T, Streeper T, Cawthon P, Baldwin K, Taaffe DR, Harris TB . Sarcopenia: etiology, clinical consequences, intervention, and assessment. Osteoporos Int 2009; 21: 543–559.
American Spinal Injury Association International Standards for Neurological Classification of Spinal Cord Injury. Revised 2011. American Spinal Injury Association: Atlanta, GA, USA. 2011.
Ditunno JF Jr., Young W, Donovan WH, Creasey G . The international standards booklet for neurological and functional classification of spinal cord injury. American Spinal Injury Association. Paraplegia 1994; 32: 70–80.
Kirshblum SC, Memmo P, Kim N, Campagnolo D, Millis S . American Spinal Injury Association. Comparison of the revised 2000 American Spinal Injury Association classification standards with the 1996 guidelines. Am J Phys Med Rehabil 2002; 81: 502–505.
Invernizzi M, Carda S, Milani P, Mattana F, Fletzer D, Iolascon G et al. Development and validation of the Italian version of the Spinal Cord Independence Measure III. Disabil Rehabil 2010; 32: 1194–1203.
Lukaski HC, Johnson PE, Bolanchuk WW, Lykken GI . Assessment of fat-free mass using bioelectrical impedance measurement of the human body. Am J Clin Nutr 1985; 41: 810–817.
Kyle UG, Genton L, Hans D, Pichard C . Validation of a bioelectrical impedance analysis equation to predict appendicular skeletal muscle mass (ASMM). Clin Nutr 2003; 22: 537–543.
Melton LJ 3rd, Khosla S, Crowson CS, O’Connor MK, O’Fallon WM, RIggs BL . Epidemiology of sarcopenia. J Am Geriatr Soc 2000; 48: 625–630.
Fleming TR, Powers JH . Biomarkers and surrogate endpoints in clinical trials. Stat Med 2012; 31: 2973–2984.
Grimby G, Broberg C, Krotkiewska I, Krotkiewski M . Muscle fiber composition in patients with traumatic cord lesion. Scand J Rehabil Med 1976; 8: 37–42.
Mohr T, Andersen JL, Biering-Sorensen F, Galbo H, Bangsbo J, Wagner A et al. Long-term adaptation to electrically induced cycle training in severe spinal cord injured individuals. Spinal Cord 1997; 35: 1–16.
Amato AA, Sivakumar K, Goyal N, Davis WS, Salajegheb M, Praestgaard J et al. Treatment of sporadic inclusion body myositis with bimagrumab. Neurology 2014; 83: 2239–2246.
Giangregorio L, McCartney N . Bone loss and muscle atrophy in spinal cord injury: epidemiology, fracture prediction, and rehabilitation strategies. J Spinal Cord Med 2006; 29: 489–500.
Castro MJ, Apple DF Jr., Hillegass EA, Dudley GA . Influence of complete spinal cord injury on skeletal muscle cross-sectional area within the first 6 months of injury. Eur J Appl Physiol Occup Physiol 1999; 80: 373–378.
Drummond MJ, Glynn EL, Lujan HL, Dicarlo SE, Rasmussen BB . Gene and protein expression associated with protein synthesis and breakdown in paraplegic skeletal muscle. Muscle Nerve 2008; 37: 505–513.
Zhang D, Liu M, Ding F, Gu X . Expression of myostatin RNA transcript and protein in gastrocnemius muscle of rats after sciatic nerve resection. J Muscle Res Cell Motil 2006; 27: 37–44.
Léger B, Senese R, Al-Khodairy AW, Dériaz O, Gobelet C, Giacobino J-P et al. Atrogin-1, MuRF1, and FoXO, as well as phosphorylated GSK-3β and 4E-BP1 are reduced in skeletal muscle of chronic spinal cord-injured patients. Muscle Nerve 2009; 40: 69–78.
Mirza FS, Padhi ID, Raisz LG, Lorenzo JA . Serum sclerostin levels negatively correlate with parathyroid hormone levels and free estrogen index in postmenopausal women. J Clin Endocrinol Metab 2010; 95: 1991–1997.
Lewiecki EM . Sclerostin: a novel target for intervention in the treatment of osteoporosis. Discov Med 2011; 12: 263–273.
Lewiecki EM . Sclerostin monoclonal antibody therapy with AMG 785: a potential treatment for osteoporosis. Expert Opin Biol Ther 2011; 11: 117–127.
Papapoulos SE . Targeting sclerostin as potential treatment of osteoporosis. Ann Rheum Dis 2011; 70 (): i119–i122.
Warden SJ, Bennell KL, Matthews B, Brown DJ, McMeeken JM, Wark JD . Quantitative ultrasound assessment of acute bone loss following spinal cord injury: a longitudinal pilot study. Osteoporos Int 2002; 13: 586–592.
Jiang SD, Dai LY, Jiang LS . Osteoporosis after spinal cord injury. Osteoporos Int 2006; 17: 180–192.
NOF. National Osteoporosis Foundation Clinician's Guide to Prevention and Treatment of Osteoporosis http://nof.org/hcp/clinicians-guide 2013.
Hollaender R, Hartl F, Krieg MA, Tyndall A, Geuckel C, Buitrago-Tellez C et al. Prospective evaluation of risk of vertebral fractures using quantitative ultrasound measurements and bone mineral density in a population-based sample of postmenopausal women: results of the Basel Osteoporosis Study. Ann Rheum Dis 2009; 68: 391–396.
Khaw KT, Reeve J, Luben R, Bingham S, Welch A, Wareham N et al. Prediction of total and hip fracture risk in men and women by quantitative ultrasound of the calcaneus: EPIC-Norfolk prospective population study. Lancet 2004; 363: 197–202.
Gonnelli S, Cepollaro C, Montagnani A, Martini S, Gennari L, Mangeri M et al. Heel ultrasonography in monitoring alendronate therapy: a four-year longitudinal study. Osteoporos Int 2002; 13: 415–421.
Spungen AM, Wang J, Pierson RN Jr, Bauman WA . Soft tissue body composition differences in monozygotic twins discordant for spinal cord injury. J Appl Physiol 2000; 88: 1310–1315.
Modlesky CM, Bickel CS, Slade JM, Meyer RA, Cureton JK, Dudley GA . Assessment of skeletal muscle mass in men with spinal cord injury using dual-energy X-ray absorptiometry and magnetic resonance imaging. J Appl Physiol 2004; 96: 561–565.
Osterthun R, Post MW, van Asbeck FW, van Leeuwen CM, van Koppenhagen CF . Causes of death following spinal cord injury during inpatient rehabilitation and the first five years after discharge. A Dutch cohort study. Spinal Cord 2014; 52: 483–488.
Shields RK, Dudley-Javoroski S . Musculoskeletal adaptations in chronic spinal cord injury: effects of long-term soleus electrical stimulation training. Neurorehabil Neural Repair 2007; 21: 169–179.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest
Rights and permissions
About this article

Cite this article
Invernizzi, M., Carda, S., Rizzi, M. et al. Evaluation of serum myostatin and sclerostin levels in chronic spinal cord injured patients. Spinal Cord 53, 615–620 (2015). https://doi.org/10.1038/sc.2015.61
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2015.61
This article is cited by
-
Association of serum sclerostin levels with marrow adiposity in postmenopausal women with glucocorticoid-induced osteoporosis
BMC Endocrine Disorders (2024)
-
Endocrinological and inflammatory markers in individuals with spinal cord injury: A systematic review and meta-analysis
Reviews in Endocrine and Metabolic Disorders (2022)
-
Association of serum bone- and muscle-derived factors with age, sex, body composition, and physical function in community-dwelling middle-aged and elderly adults: a cross-sectional study
BMC Musculoskeletal Disorders (2019)
-
Mitochondrial health and muscle plasticity after spinal cord injury
European Journal of Applied Physiology (2019)
-
Osteoporosis in Veterans with Spinal Cord Injury: an Overview of Pathophysiology, Diagnosis, and Treatments
Clinical Reviews in Bone and Mineral Metabolism (2019)
