
Key Points
-
Highlights the fact that stark inequalities exist in relation to deprivation and negative behaviours
-
Highlights the behaviours of young people with respect to their reported alcohol use and smoking habits.
-
Considers reported tooth brushing habits and behaviours in boys and girls by age, sex and country of residence.
Abstract
Background The 2013 Children's Dental Health Survey is the fifth in a series of national surveys.
Aim To describe the oral health behaviours in children and adolescents in England, Wales and Northern Ireland.
Method A representative sample of children (aged 5, 8 12 and 15 years) in England, Wales and Northern Ireland were invited to participate in dental examinations. Children and parents were also invited to complete a questionnaire about oral health behaviours.
Results Overall, the majority of children and young people reported good oral health behaviours. For example, more than three quarters of the 12- and 15-year-olds reported brushing their teeth twice a day or more often. However, a sizeable proportion of the sample reported less positive behaviours. Nearly 30% of 5-year-olds first started to brush their teeth after the age of one year. Among 15-year-olds, 11% were current smokers and 37% reported that they currently drank alcohol. Sixteen percent of 12-year-olds reported to consume drinks containing sugar four or more times a day. Of particular concern was the marked differences that existed by level of deprivation. Children living in lower income households (eligible for free school meals) were less likely to brush their teeth twice a day, more likely to start brushing after six months, more likely to be a smoker and more likely to consume frequent amounts of sugary drinks.
Conclusion Despite some encouraging overall patterns of good oral health behaviours, a sizeable proportion of children and young people reported behaviours that may lead to poorer oral and general health. Preventive support should be delivered in clinical dental settings to encourage positive oral health behaviours. Public health strategies are also needed to reduce inequalities in oral health behaviours among children and young people.
Similar content being viewed by others


Introduction
The 2013 Children's Dental Health (CDH) Survey is the fifth in a decennial series of national surveys of children's oral health that have been carried out in the UK since 1973. These surveys have delivered valuable data relating to children's oral health providing useful insights into disease patterns and trends, and use of dental services.
An innovation of the 2013 survey was the development and introduction of a pupil questionnaire administered to 12- and 15-year-olds, which collected a range of data including information on their oral health behaviours. Collecting data directly from young people provides them with an opportunity to express their views, experiences and behaviours. This data therefore complements the traditional clinical information gathered through the clinical examination and the questionnaire data collected from the parents. This paper describes the oral health related behaviours, for 5 and 8-year-olds as reported by their parents, and for the 12- and 15-year-olds through their own self-reports.
It is well established that a range of common risk behaviours are linked to the general and oral health of individuals and populations.1,2Diet, smoking, alcohol consumption and oral hygiene practices are known risk factors for poor oral health and general health. Many of these health related behaviours are initiated in childhood and adolescence, and track into adulthood.3,4
This paper presents data relating to children's oral health behaviours including tooth brushing and other oral hygiene practices, diet habits including drink and snack consumption, alcohol use and smoking. The aim of this paper is to describe the oral health related behaviours of children participating in the 2013 Child Dental Health Survey, and to highlight any significant trends from previous surveys.
Methodology
The 2013 CDH Survey was based on a representative sample of children aged 5, 8, 12 and 15 years, attending government maintained and independent schools in England, Wales and Northern Ireland. Alongside the clinical data collected at the dental examinations, one of the strengths of the 2013 CDH Survey was the measurement of behavioural and attitudinal information collected about the children involved in the survey through the use of questionnaires. The 'pupil' questionnaire for 12- and 15-year-olds aimed to complement the questionnaires sent to parents. Full details of the survey sampling, response rates, examination protocols and statistical methods can be found elsewhere.5
Development of the content for the 2013 survey questionnaires began with the parent questionnaire used in the 2003 survey, together with the views collected from a stakeholder consultation exercise involving a diverse range of participants including consultants and specialists from a number of dental specialties, school teachers, parents and older children. The consortium was aware of the need for the questionnaire to be short and accessible in light of declines in response rates to other surveys. Both the pupil and parent questionnaire underwent the same development process which included cognitive testing and piloting.
The pupil questionnaire was administered at the same time as the dental examination and the parental questionnaire was posted to parents of all children who had a dental examination. Parental consent was obtained for 5- and 8-year-olds before the dental examination, with the child being allowed to opt out on the day. Consent for 12- and 15-year-olds was obtained on the day of the examination by the pupil themselves, with parents able to opt-out their child in advance.
The pupil questionnaire, completed by the young people themselves, collected a range of information on their perceptions and behaviours relevant to oral health, and health more generally. This approach allowed the collection of self-reported data on risk factors for oral health, such as sugar, alcohol and tobacco consumption. The parent questionnaire collected, for all age groups, information on their child's oral health hygiene practices and the parental perceptions of the child's oral health. The final pupil and parent questionnaires can be found in the 2013 CDH Survey Technical Report.5
The questionnaire data was analysed by age, sex, country of residence and level of deprivation. The 2013 CDH Survey used children's eligibility for free school meals (FSM's) as a proxy for income deprivation for those living in low-income families. It is important to note that only children living in low-income families were eligible for FSM's at the time the survey was conducted. Where statistically significant differences between groups are reported, the 5% threshold (P <0.05) was used. The survey was ethically favourably reviewed by University College London Ethics Committee (Project ID: 2000/003).
Results
Questionnaire response
The pupil questionnaire for 12- and 15-year-olds achieved a response rate of 99.6%. The overall response rate for the parent questionnaire was 43%. The response rate for parents was higher among those with 5 and 8-year-old children where written consent had already been provided for the dental examination. Item non-response in both the parent and pupil questionnaires was generally below 2%.
Tooth brushing
Overall around three quarters of older children reported brushing their teeth twice a day (77% for 12-year-olds and 81% for 15-year-olds), with parents reporting similar patterns in the five and eight-year-old age groups (82% and 84% respectively) (Table 1). Parental reports of tooth brushing behaviour were similar to child self-reports, so self-reports are reported when available (12- and 15-year-olds).
In all age groups, girls were significantly more likely to brush twice daily than boys. In terms of free school meal eligibility, across all age groups children were less likely to brush twice a day if they were eligible for free school meals. In particular, significant differences were seen at 5 years of age, with 69% brushing twice a day among those eligible for free meals and 85% among those not eligible. Minimal differences were found in reported tooth brushing practices across the three countries.
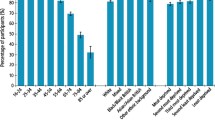
Interesting trends in tooth brushing practices were found over a 30 year period across all age groups in England, Wales and Northern Ireland (Fig. 1). The percentage of children reported to brush twice a day has increased in all age groups since 1983, although the increase more recently was not as pronounced as from 1983 to 1993. For example, among 5-year-olds, just over half (53%) reported to brush twice daily in 1983, compared with three quarters (75%) in 1993. In 2003 just under 80% reported to brush twice daily and this increased to 83% in 2013. Only among the younger groups (5- and 8-year-olds) was there a significant increase in reported tooth brushing frequency from 2003 to 2013.

Percentage of children reported by parents to brush their teeth twice a day (England, Wales and Northern Ireland 1983-2013)
About a quarter of children (21%) first had their teeth brushed when they were less than six months old, with around 50% between six months and a year, and a quarter of children (25%) where the age of tooth brushing was delayed until the child was over the age of one year. Negligible differences were found for the age of first starting tooth brushing by sex and country of residence (Table 2). However, in terms of income deprivation, for those eligible for free school meals at age five, only one in ten (12%) had started to brush before the age of six months compared to nearly a quarter (23%) among those not eligible for free meals.
Other oral hygiene practices
The use of other oral hygiene aids was first reported in the 2003 survey and provides a useful indication of the range of hygiene practices and aids used. As well as a brush (manual or electric) and toothpaste, the majority of children (with the exception of 5-year-olds) also used other oral hygiene products, with rates of product use increasing as children got older. Not unexpectedly, the use of mouthwashes, chewing gum and dental floss was higher for older children.
Mouthwash was the most common oral hygiene aid reportedly used. Twenty-two percent of children aged five years, 57% of those aged eight, 60% of those aged 12 years and 67% of those aged 15 years reported using mouthwash. The electric toothbrush was used by approximately 40% of children, regardless of age group. Chewing gum was used by 8% of 5-year-olds, 20% of 8-year-olds, 31% of 12-year-olds, and 34% of 15-year-olds.
Few differences were found between use of hygiene aids and age, sex and country of residence. However, girls at age 15 were significantly more likely to use dental floss and chewing gum than boys at the same age. In terms of income deprivation, children eligible for free school meals were significantly more likely to solely rely on a toothbrush and toothpaste, and less likely to use an electric toothbrush at ages 5, 8 and 15 years, than their more affluent counterparts.
Alcohol use and smoking
For the first time, the 2013 CDH Survey asked questions relating to alcohol and smoking in the self-complete 12 and 15-year-old questionnaire (Table 3). The proportion of 12-year-olds smoking was low at 7%, however more than one in ten (11%) 15-year-olds reported they were a current smoker and 29% stated having ever smoked a cigarette. In both age groups no significant differences were found by sex. However, among 12-year-olds those eligible for free school meals were significantly more likely to report being a current smoker and having ever smoked than those not eligible. No significant differences in smoking by deprivation were found at age 15.However, some significant differences between smoking and countries were found. Fifteen-year-olds in Wales were significantly less likely to ever having smoked, compared with England and Northern Ireland, and 12-year-old children in Wales and Northern Ireland reported less current smoking than those in England.
A third (29%) of 12-year-olds reported having ever drunk alcohol and this increased to nearly three quarters among the 15-year-olds (72%). At age 12 only 3% reported being a current drinker but this increased to 39% among the 15-year-olds. Associations by sex were found for 12-year-olds, with boys significantly more likely to have ever drunk alcohol than girls. A significant relationship was also found between alcohol consumption and country of residence, with Northern Ireland having rates of current drinking significantly lower among both 12- and 15-year-olds than England and Wales, with 40% of 15-year-olds in England, 46% in Wales reporting being a current drinking and in contrast to only 28% in Northern Ireland. Contrary to what was observed for other health behaviours, at age 15 children not eligible for free school meals were significantly more likely to report themselves as a current drinker and having ever drunk alcohol than those eligible for free school meals.
Drinks and snacks consumption
Dietary sugar is an important risk factor for dental caries and obesity.6 The pupil questionnaire included a range of drinks and snacks that were relatively high in sugar, for example, sweets and soft drinks, and some items that were sugar free, for example, water. Respondents were asked to answer how often they consumed these items throughout the day. Table 4 indicates the percentages of 12- and 15-year-olds consuming a range of drinks and snacks four or more times a day. Sugary drinks included consumption of coke or other soft drinks or squashes and energy (sports) drinks. Sugary snacks included consumption of sweets and cakes or biscuits.
Sixteen percent of 12-year-olds and 14% of 15-year-olds consumed drinks containing sugar including energy drinks, four or more times a day. (Table 4) Significant differences were found in consumption of sugary drinks by level of deprivation. Children who were eligible for free school meals were twice as likely than those not eligible to report consuming sugary drinks this frequently. For example, among 12-year-olds 26% of children who were eligible for free school meals reported drinking sugary drinks four or more times per day in contrast to only 13% of children not eligible for free meals.
Approximately a third of both 12- and 15-year-olds reported consuming sugary snacks four or more times per day. Sugary snack consumption did not vary significantly by sex, deprivation level or country of residence.
Discussion
This paper has highlighted some important findings on oral health behaviours among a national sample of children and adolescents. More than three quarters of older children, reported brushing their teeth twice a day or more often, with girls more likely to do so than boys. Approximately a quarter of children were reported to have started tooth brushing after the age of 12 months. Along with a toothbrush and toothpaste, other dental aids were used by the majority of children, with mouthwash being the most commonly reported, and 40% of children were reported to be using an electric toothbrush. Among 15-year-olds, 11% said that they currently smoked and 37% that they drank alcohol. 16% of 12-year-olds and 14% of 15-year-olds reported to consume drinks containing sugar, including energy drinks, four or more times a day.
Since 1983 there has been a consistent improvement in reported rates of tooth brushing frequency by age, sex and country of residence. While it is encouraging to see the frequency of reported tooth brushing twice daily has increased over recent decades, there are still about 20% of children who are brushing less than twice a day. Only 21% of children had tooth brushing initiated before the age of six months, a worrying finding as Public Health England clearly recommends that tooth brushing be started around the six month period.
Sugary drink consumption has recently become a highly debated and topical issue in terms of both oral and general health. With the popularity of sugary drinks among teenagers, health professionals are concerned about the health implications, including obesity and dental caries. The recent World Health Organization6 and UK Scientific Advisory Committee on Nutrition (SACN)7 have both recommended that free sugars should account for no more than 5% of total energy intake – our findings that around 15% of young people consumed sugary drinks four or more times a day, is certainly alarming.
Many of the health behaviours investigated in this paper, varied by level of deprivation as measured by free school meal eligibility. Those eligible for free school meals were less likely to brush twice a day, more likely to consume sugary drinks, be a current smoker or have ever smoked cigarettes, be less likely to use an electric toothbrush or be more likely to rely solely on a toothbrush and toothpaste. Those eligible for free school meals were also less likely to start brushing their teeth before the age of six months. These statistically significant social differences in oral health behaviours provide up to date information on oral health inequalities from a nationally representative sample of children and adolescents.
There are very few other studies in the UK that have investigated behaviours relating to oral health, and this is a major strength of the 2013 CDH survey. However the 'Smoking, drinking and drug use among young people survey' was carried out in 20128 and reported broadly similar results for smoking and alcohol use among 12- and 15-year-olds. The Smoking, Drinking and Drug Use Survey reported that 9% of 12-year-olds reported having ever smoked as compared to the 7% reported in the 2013 CDH Survey. When comparing adolescent drinking, 18% of 12-year-olds and 74% of 15-year-olds in the Smoking, Drinking and Drug Use survey reported to ever had a drink compared to the 29% of 12-year-olds and 72% of 15-year-olds in the 2013 CDH Survey.
A major strength of the 2013 CDH Survey is the introduction of the novel pupil questionnaire. For the first time in the decennial dental health surveys we have information directly from children and young people themselves. Questions on smoking, alcohol and sugary drink and snack consumption are a welcome introduction and provide a new insight into oral health-related behaviours, while tooth brushing and oral hygiene questions, having been asked previously, provide us with useful trend data.
The results of this study must, however, be interpreted with a degree of caution, as both the parental and pupil questionnaires were self-reported, and therefore the answers given may reflect what the respondent feels they should do, and not what they actually do. This social desirability bias could lead to over reporting of perceived 'good behaviours' and under reporting of so-called 'bad behaviours'.9 It should also be remembered that consent methodology have changed since the previous survey in 2003, with procedures moving from an opt-out to an opt-in consent process. This could account for the lower response rates for the five and eight-year-old children's examinations, which in turn impacts upon the accuracy of the results, with potentially more bias occurring as those with worse oral health are more likely to opt out. Another limitation would be the use of the proxy measure used for deprivation, in the form of eligibility for free school meals. This measure is not a measure of socioeconomic position but a simple indicator of deprivation.
Conclusion
Overall, the majority of children and young people reported good oral health behaviours and some encouraging trends were evident. However, a sizeable proportion of the sample reported less positive behaviours. For example, nearly 30% of five years had not started tooth brushing by the age of one, 10% of 15-year-olds were current smokers and nearly 40% were current drinkers, and 16% of 12-year-olds consumed sugary drinks four or more times per day. Of particular concern, however, was the stark social inequalities evident across the sample. Children living in deprived households (eligible for free school meals) were less likely to brush their teeth twice a day, more likely to start brushing after six months, more likely to be a smoker and more likely to consume frequent amounts of sugary drinks.
The results of the 2013 CDH Survey highlight the on-going need for preventive care delivered in clinical settings, together with broader public health measures to promote healthy behaviours and reduce oral health inequalities. It is essential that the dental profession works with other agencies and sectors to promote positive oral health behaviours among children and adolescents.
References
World Health Organization. Global health risks: mortality and burden of disease attributable to selected major risks. Geneva: World Health Organization, 2009.
Sheiham A, Watt R G . The common risk factor approach: a rational basis for promoting oral health. Community Dent Oral Epidemiol 2000; 28: 399–406.
Paavola M, Vartiainen E, Haukkala A . Smoking, alcohol use, and physical activity: A 13-year longitudinal study ranging from adolescence into adulthood. J Adolesc Health 2004; 35: 238–244.
Kelder S H, Perry C L, Klepp K I, Lytle L L . Longitudinal tracking of adolescent smoking, physical activity, and food choice behaviours. Am J Public Health 1994; 84: 1121–1126.
Anderson T, Thomas C, Ryan R, Dennes M, Fuller E . Children's Dental Health Survey 2013 Technical Report England, Wales and Northern Ireland. London: Health and Social Care Information Centre, 2015.
World Health Organization. Guideline: Sugars intake for adults and children. Geneva: World Health Organization, 2014.
Scientific Advisory Committee on Nutrition. Carbohydrates and Health London: TSO, 2015.
Fuller E, Henderson H, Nass L, Payne C, Phelps A, Ryley A . Smoking, drinking and drug use among young people in England in 2012. London: Health and Social Care Information Centre, 2013.
Randall D M, Fernandes M F . The social desirability response bias in ethics research. J Bus Ethics 1991; 10: 805–817.
Acknowledgements
The authors wish to thank the children and young people who took part in the research as well as their parents and guardians. In addition, the authors express gratitude to the dental examining teams, field workers from the Office for National Statistics, staff in the schools visited and the individuals involved in the consortium for their invaluable contributions. The 2013 CDHS was commissioned by the Health and Social Care Information Centre (HSCIC) and the research was carried out by a consortium led by the Office for National Statistics. We particularly extend our thanks to Tom Anderson of the ONS Social Survey Division and the wider ONS research team.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Porter, J., Ravaghi, V., Hill, K. et al. Oral health behaviours of children in England, Wales and Northern Ireland 2013. Br Dent J 221, 263–268 (2016). https://doi.org/10.1038/sj.bdj.2016.646
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2016.646
