Abstract
This retrospective study was designed to review the relative frequency and prognostic significance of extramedullary infiltrates in children with acute myeloid leukaemia (AML). The registration data and initial discharge summaries were reviewed for all children diagnosed with AML, and registered by the Dutch Childhood Leukaemia Study Group (DCLSG). Between 1972 and 1998, 477 children were diagnosed with AML. Of these patients, 120 (25.1%) had extramedullary leukaemia (EML) at diagnosis. Four categories of EML were found: skin, soft tissue or bone, gingival infiltration and central nervous system (CNS) involvement. Patients who presented with gingival infiltrates, were older than those without EML or those in the other EML subgroups, had a high initial WBC count and a high proportion of M4/M5 morphological variants. This type of presentation could indicate a special biological entity. Univariate analysis of prognostic factors in patients treated after 1985 with intensive protocols showed that initial WBC count and the presence of favourable cytogenetic findings were significant. The presence of EML at diagnosis had no significant effect on event-free survival. In a stepwise multiple regression analysis only favourable cytogenetic findings remained significant.
Similar content being viewed by others
Introduction
Children with acute myeloid leukaemia (AML) often exhibit extramedullary infiltrates at diagnosis.1 The incidence of extramedullary leukaemia (EML) is reported to be between 20 and 40%.23 Sometimes, EML precedes the diagnosis of bone marrow involvement by weeks or months and poses a considerable therapeutic dilemma.4 The most common manifestations of EML are skin infiltrates, soft tissue or bone involvement, gingival infiltration and central nervous system (CNS) involvement. Testicular involvement is very rare in AML. The soft tissue tumours are also referred to as chloromas or in recent literature as granulocytic sarcomas or myeloblastomas.1
EML is more common in infants with AML,56789 and EML is also more common in the myelo-monocytic or monoblastic variants of AML (FAB M4 and M5), than in other morphological subtypes.310
There is considerable controversy about the prognostic significance of extramedullary involvement in AML. While some groups found that it conferred a poorer prognosis,1112 in other studies this does not seem to be the case.313
The chloromatous manifestation of AML seems to be more common in Africa and Asia, although it is not clear, whether genetic or socio-economic factors are responsible.1415 Blast cells from patients with myeloblastoma often exhibit the 8;21 chromosomal translocation.1617 Although the 8;21 translocation is generally associated with a relatively better prognosis, the presence of EML may compromise this prognostic advantage.1
Recently, Schwyzer et al18 reported from South Africa that AML with a myeloblastoma (chloroma) at diagnosis is associated with the 8;21 translocation and that these children have a better prognosis than those without myeloblastoma and t(8;21). Others reported an inferior prognosis for patients with myeloblastoma.1419
The controversies in the literature, concerning the incidence and prognostic significance of EML, prompted us to review retrospectively the population-based data of the DCLSG over the years 1972–1998, for the presence and prognostic significance of EML.
Patients and methods
Since 1972, children with leukaemia have been registered by the Dutch Childhood Leukaemia Study Group (DCLSG). This national registry is estimated to be 97% complete.20 Bone marrow and peripheral blood samples and smears of children suspected of having leukaemia are sent to the laboratory of the DCLSG for confirmation and classification of diagnosis and relapse. The diagnosis and FAB subtype was determined with May–Grünwald-Giemsa stained smears and additional stains, including Sudan-B-Black, myeloperoxidase, α-naphtyl acetate esterase with and without sodium fluoride. FAB classification was not available for the first 56 patients. The diagnosis of AML required the presence of >30% blast cells in the bone marrow and that leukaemic cells show morphological and cytochemical characteristics of myeloid or monocytic differentiation. Cytogenetic data were available for 170 of the 260 patients reported on a national level since 1989. Centralized phenotyping for AML patients was started in 1987.
Registration data and initial discharge summaries were reviewed for the presence of EML in all children with AML, aged 0–16 years, who were registered by the DCLSG from April 1972 to December 1998. EML was defined as a clinically obvious infiltrate in soft tissues, skin, muscles or bone, gingiva, cerebrospinal fluid or brain. CNS leukaemia was diagnosed on the basis of >5/μl blast cells in the CSF without blood contamination or as a leukaemic infiltration of the brain as evidenced by cranial CT scan. Complete remission was defined as <5% blast cells in the bone marrow, normal haematopoiesis and the absence of blast cells in the peripheral blood. Relapse was defined as a return of leukaemic blast cells in the bone marrow (>20%) and/or return of the EML.
Treatment protocols
A number of treatment protocols were used during the 26-year period of this retrospective study. Between 1972 and 1980 institutional protocols were used. From 1980 to 1982 patients received high-dose Ara-C, 6-thioguanine and daunorubicine induction, but no maintenance therapy. Those with HLA-identical siblings proceeded to bone marrow transplantation (BMT).21 From 1982 to 1985 induction treatment was individually ‘tailored’ on the basis of cells in S-phase. Patients entering remission went on to BMT or received the VAPA-10 protocol as maintenance.22 From 1985, treatment strategies were based on the BFM protocols, and the first national BFM-based AML study started in 1987.23 From 1997, the DCLSG has participated in the current UK MRC-12 AML Study.
Statistical methods
One-way ANOVA or two-sided t-test was used to test the differences between means of continuous variables. Pearson's chi-square test was applied to categorical variables with post-hoc comparisons. Event-free survival was calculated with the Kaplan–Meier method from the time of diagnosis to the first event (relapse or death of any cause) or censoring (date of last follow-up). Patients who did not achieve remission were considered as treatment failure on day 1.
The statistical difference between survival curves was calculated with the log-rank test. Cox regression was used for multivariate analysis. All statistical tests were carried out using SPSS for Windows (version 8). As the intensity of treatment is the most important determinant of prognosis, only patients diagnosed after 1 January 1985 were included in the analysis of event-free survival. Patients with an overlap (two forms of EML) were excluded from the subgroup analyses.
Results and discussion
There is conflicting information in the literature on the relative frequency of EML at diagnosis in AML. Some authors reported a frequency of 38–42%.212 This is rather more than the 25.1% found in our large, retrospective study. From April 1972 to December 1998, 477 consecutive patients (0–16 years old) were diagnosed with de novo AML and registered by the DCLSG. Of these patients, 120 had EML at presentation.
There is also little agreement in the literature over what constitutes an EML. While some authors include, for example, CNS leukaemia or hepatosplenomegaly, others do not.24 Among the patients reported here, 35 (7.3%) had soft tissue or bone involvement, 30 (6.3%) gingival infiltrates, 30 (6.3%) had CNS involvement and six (1.2%) had skin infiltrates. Nineteen patients (4%) had double sites of EML (Table 1). The localisation of the myeloblastoma was as follows; orbit 35, jaw four, mastoid one, breast one, upper extremity two, pancreas two, paraspinal one, buttocks two, lower extremities one. No isolated EMLs were found in the registry, all children with an EML had BM infiltration at diagnosis. The length of the pre-diagnostic history of soft tissue swelling varied between a few days and a few weeks.
Characteristics in patients with or without EML are summarised in Table 2. The four types of EML found in this study correspond to the most frequently reported forms. Although the relative frequency of their occurrence varies between reported studies, these differences are not remarkable.122526
When patients were split into two age groups, infants (age <1 year) with EML tended to fall into the myeloblastoma and CNS-positive group, had more skin infiltrates but there was only one infant with gingival infiltration. This corresponds to the higher mean age in the gingival infiltration group. Infants had a higher relative proportion of monoblastic leukaemia (FAB-M5) and presented less often with M1, M2 or M3 morphology. The event-free survival of infants was not significantly worse than that of children above 1 year of age.
In a univariate analysis of prognostic factors, initial WBC count and favourable cytogenetic findings (defined as: t(8;21) or t(15;17) or inv16 or trisomy 21) were significant factors (Table 3). In a stepwise multiple regression analysis only favourable cytogenetics remained significant (P = 0.033).
Myeloblastoma is often associated with FAB-M2 morphology and the 8;21 chromosomal translocation.116 While this translocation is generally associated with a better prognosis, the presence of EML (or more likely a molecular event behind it) might jeopardise this positive effect.1619 Genetic or socio-economic factors may further complicate this interaction. While children in Turkey and India had a poor outcome when presenting with orbital myeloblastoma,1415 their counterparts in South Africa seemed to have fared much better,18 and in most European or US studies and in a recent study from Saudi Arabia, the presence of myeloblastoma at diagnosis had no influence on survival.3121324
A possible explanation for the more infiltrative behaviour of leukaemic cells in EML could be an altered cell surface phenotype. Hurwitz et al27 reported in children with AML that the coexpression of CD19 and CD56 antigens is specific for the t(8;21) and suggested that the expression of the CD56 N-CAM neuronal adhesion molecule could explain the higher incidence of granulocytic sarcomas in patients with the above translocation. Seymour et al28 confirmed the coexpression of CD56 and CD19 in adult patients, but found a much smaller incidence of CD56 expression in the M2 cell type and no correlation with EML. Again, the same phenotype and morphology may mean something quite different in children than in adults.
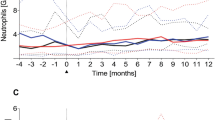
Perhaps even more puzzling are our findings in children with gingival infiltrates. Gingival hypertrophy seems to be a special form of EML, where local microanatomic characteristics could play an additional role to that of the myeloid blast cells.29 Patients with gingival infiltrates in our series were older at diagnosis, had a high WBC count and a very high proportion of myelo-monocytic or monoblastic morphology (Table 2). Their EFS seems poorer than those, for example, with a myeloblastoma (Figure 1) but because of the small numbers one can draw no conclusions on this issue. Nevertheless, this observation calls attention to the need to prospectively investigate these patients, who may well require more intensive treatment in the future.

Kaplan–Meier estimate of event-free survival for patients with and without extra-medullary infiltrates at diagnosis. Logrank test for EFS, P = 0.85.
Primary myeloblastoma, preceding the clinical diagnosis of AML should be treated with systemic chemotherapy, just as when they occur simultaneously.1 Permanent local control at sites of EML can be achieved without local therapy such as irradiation.24 The most important therapeutic question is whether patients with EML should receive more intensive treatment than others. Similarly to others, we found no significant difference in the EFS of patients with or without EML. In current studies, patients with EML at diagnosis are not allocated to a different or more intensive treatment arm. Analysis of the clinical and biological data from ongoing collaborative studies may throw more light on the pathomechanism and prognostic significance of EML in AML, particularly in patients with the t(8;21) karyotype.
References
Byrd JC, Edenfield WJ, Shields DJ, Dawson NA . Extramedullary myeloid cell tumors in acute nonlymphocytic leukemia: a clinical review J Clin Oncol 1995 13: 1800–1816
Creutzig U, Harbott J, Sperling C, Ritter J, Zimmermann M, Löffler H, Riehm H, Schellong G, Ludwig WD . Clinical significance of surface antigen expression in children with acute myeloid leukemia: results of study AML-BFM-87 Blood 1995 86: 3097–3108
Ravindranath Y, Steuber CP, Krischner J, Civin CI, Ducore J, Vega R, Pitel P, Inoue S, Bleher E, Sexauer C, Hutter J, Vietti T . High-dose cytarabine for intensification of early therapy of childhood acute myeloid leukemia: a Pediatric Oncology Group study J Clin Oncol 1991 9: 572–580
Luckit J, Bain B, Matutes E, Min T, Pinkerton R, Catovsky D . Teaching cases from the Royal Marsden and St Mary's Hospitals: an orbital mass in a young girl Leuk Lymphoma 1998 28: 621–622
Creutzig U, Schaaff A, Ritter J, Jobke A, Kaufmann U, Schellong G . Akute myeloische Leukämie bei Kindern unter 2 jahren: Untersuchungen und Behandlungsergebnisse bei 23 Kindern der AML-Therapiestudie BFM-78 Klin Pädiat 1984 196: 130–134
Vormoor J, Ritter J, Creutzig U, Boos J, Heyen P, Ludwig W-D, Harbott J, Löffler H, Schellong G . Acute myelogenous leukaemia in children under 2 years – experiences of the West German AML studies BFM-78, -83 and -87 Br J Cancer 1992 66: (Suppl.) 63–67
Van Wering ER, Kamps WA . Acute leukemia in infants Am J Pediatr Hematol Oncol 1986 8: 220–224
Pui CH, Kalwinsky DK, Schell MJ, Mason CA, Mirro J, Dahl GV . Acute non-lymphoblastic leukemia in infants: clinical presentation and outcome J Clin Oncol 1988 6: 1008–1013
Ribeiro RC, Raimondi SC, Srivastava DK, Tong X, Behm FG, Razzouk BI, Evans WE, Pui CH . Prognostic factors for very young children with acute myeloid leukemia Blood 1999 94: 501a
Grier HE, Gelber RD, Camitta BM, Delorey MJ, Link MP, Price KN, Leavitt PR, Weinstein HJ . Prognostic factors in childhood acute myelogenous leukemia J Clin Oncol 1987 5: 1026–1032
Gehan EA, Smith TL, Freireich EJ, Bodey G, Rodriguez V, Speer J, McCredie K . Prognostic factors in acute leukemia Semin Oncol 1976 3: 271–282
Woods WG, Kobrinsky N, Buckley J, Neudorf S, Sanders J, Miller L, Barnard D, Benjamin D, DeSwarte J, Kalousek D, Shina D, Hammond GD, Lange BJ . Intensively timed induction therapy followed by autologous or allogeneic bone marrow transplantation for children with acute myeloid leukemia or myelodysplatic syndrome: A Childrens Cancer Group pilot study J Clin Oncol 1993 11: 1448–1457
Amadori S, Testi AM, Arico M, Comelli A, Giuliano M, Madon E, Masera G, Rondelli R, Zanesco L, Mandelli F . Prospective comparative study of bone marrow transplantation and postremission chemotherapy for childhood acute myelogenous leukemia J Clin Oncol 1993 11: 1046–1054
Cavdar AO, Babacan E, Gozdasoglu S, Kilicturgay K, Arcasoy A, Cin S, Ertem U, Erten J . High risk subgroup of acute myelomonocytic leukemia (AMML) with orbito-ocular granulocytic sarcoma (OOGS) in Turkish children Acta Haematol 1989 81: 80–85
Shome DK, Gupta NK, Prajapati NC, Raju GMK, Choudhury P, Dubey AP . Orbital granulocytic sarcomas (myeloid sarcomas) in acute nonlymphocytic leukemia Cancer 1992 70: 2298–2301
Tallman MS, Hakimian D, Shaw JM, Lissner GJ, Russel EJ, Variakojis D . Granulocytic sarcoma is associated with the 8;21 translocation in acute myeloid leukemia J Clin Oncol 1993 4: 690–697
Byrd JC, Weiss RB . Recurrent granulocytic sarcoma: an unusual variation of acute myelogenous leukemia associated with 8;21 chromosomal translocation and blast expression of the neural cell adhesion molecule Cancer 1994 73: 2107–2112
Schwyzer R, Sherman GG, Cohn RJ, Poole JE, Willem P . Granulocytic sarcoma in children with acute myeloblastic leukemia and t(8;21) Med Pediatr Oncol 1998 31: 144–149
Byrd JC, Weiss RB, Arthur DC, Lawrence D, Baer MR, Davey F, Trikha ES, Caroll AJ, Tantravahi R, Qusiyeh M, Patil SR, Moore JO, Mayer RJ, Schiffer CA, Bloomfield CD . Extramedullary leukemia adversely affects hematologic complete remission rate and overall survival in patients with t(8;21) (q22;q22): Results from cancer and leukemia group B8461 J Clin Oncol 1997 15: 466–475
Schouten LJ, van der Does-van den Berg A, Otter R, Coebergh JWW . Accuracy and completeness of the registration of childhood leukaemia in The Netherlands, 1989–1992 Eur J Cancer 1997 33: 891–894
Van der Does-van den Berg A, Hählen K, Colly LP . Treatment of acute nonlymphocytic leukemia with high-dose cytosine arabinoside, 6-thioguanine, and doxorubicin without maintenance therapy Pediatr Hematol Oncol 1988 5: 93–102
Hählen K, Van der Does-van den Berg A, Colly LP, Smets LA, Taminiau JAJM, Vossen JM . Treatment of childhood acute nonlymphoblastic leukemia with individually scheduled high doses of cytarabine: preliminary results of study ANLL-82 of the Dutch Childhood Leukemia Study Group (DCLSG). In: Büchner T, Schellong G, Hiddemann W, Urbanitz D, Ritter J (eds) Haematology and Blood Transfusion Vol 30: Springer: Berlin 1987 pp 389–392
Hählen K, Bökkerink J, Van der Does-van den Berg A, van Leeuwen EF, Postma A . Six months of intensive chemotherapy for childhood ANLL: preliminary results of the study ANLL-87 of the Dutch Childhood Leukemia Study Group. In: Büchner T, Hiddémann W, Wormann B, Schellong G, Ritter J (eds) Acute Leukemias IV Springer: Berlin 1994 pp 486–489
Jenkin RD, Al-Shabanah M, Al-Nasser A, El-Solh H, Al Sudairy R, Mustafa MM, Al Fawaz I, Gray A, da Cunha M, Ayas M, Al Mahr M, Kofide A, Mahgoub AN, Rifai S, Bekgaumi A, Al Jefri A, Al Musa A, Sabbah R . Extramedullary myeloid tumors in children: the limited value of local treatment J Pediatr Hematol Oncol 2000 22: 34–40
Creutzig U, Ritter J, Schellong G (BFM Study Group) . Identification of two risk groups in children with acute myelogenous leukemia after therapy intensification in study AML-BFM-83 as compared with study AML-BFM-78 Blood 1990 75: 1932–1940
Ebb DH, Weinstein HJ . Diagnosis and treatment of childhood acute myelogenous leukemia Pediatr Clin North Amer 1997 44: 847–862
Hurwitz CA, Raimondi SC, Head D, Krance R, Mirro J, Kalwinsky DK, Ayers GD, Behm FG . Distinctive immunophenotypic features of t(8;21) (q22;q22) acute myeloblastic leukemia in children Blood 1992 80: 3182–3188
Seymour JF, Pierce SA, Kantrajian HM, Keating MJ, Estey EH . Investigation of karyotypic, morphologic and clinical features in patients with acute myeloid leukemia blast cells expressing the neural cell adhesion molecule (CD56) Leukemia 1994 8: 823–826
Barrett AP . Leukemic cell infiltration of the gingiva J Periodont 1986 57: 579–581
Acknowledgements
We are indebted to Dr C Uiterwaal and Mr P Westers for their advice on data collection and statistical analysis and to colleagues in the DCLSG for referring their patients. Members of the DCLSG Board are: Prof WA Kamps, Dr JPM Bökkerink, Dr ESJM de Bont, Dr JA Rammeloo, Dr H van den Berg, Dr B Granzen, Prof PM Hoogerbrugge, Dr R Pieters, Dr T Révész, Dr ETh Korthof, Prof AJP Veerman.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bisschop, M., Révész, T., Bierings, M. et al. Extramedullary infiltrates at diagnosis have no prognostic significance in children with acute myeloid leukaemia. Leukemia 15, 46–49 (2001). https://doi.org/10.1038/sj.leu.2401971
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.leu.2401971
Keywords
This article is cited by
-
Central Nervous System Involvement in Adults with Acute Leukemia: Diagnosis, Prevention, and Management
Current Oncology Reports (2022)
-
Myeloid sarcoma is associated with poor clinical outcome in pediatric patients with acute myeloid leukemia
Journal of Cancer Research and Clinical Oncology (2020)
-
Clinical characteristics of pediatric patients with myeloid sarcoma without bone marrow involvement in Japan
International Journal of Hematology (2018)
-
Risk factors and clinical outcomes of acute myeloid leukaemia with central nervous system involvement in adults
BMC Cancer (2015)
-
Acute myeloid leukemia with mediastinal myeloid sarcoma refractory to acute myeloid leukemia therapy but responsive to l-asparaginase
International Journal of Hematology (2012)
