
Abstract
Design:
To describe a case of retroperitoneal lymphocele as an extremely rare complication after lumbar spine fracture.
Objective:
To discuss the possible mechanism of development of retroperitoneal lymphocele following blunt trauma to the ureter and lumbar spine.
Setting:
Fukui University Hospital, Fukui, Japan.
Results:
A 71-year-old man presented with severe intractable low back pain caused by a huge retroperitoneal lymphocele, which was considered to be related to an occult L4 vertebral fracture and a blunt ureteral injury. The retroperitoneal lymphocele also caused significant instability at L3–4 level, thus requiring surgical resection followed by interbody fusion.
Conclusion:
Physicians should be aware that such unusual retroperitoneal lymphocele might develop even after a blunt ureteral injury or a minor lumbar spine fracture.
Similar content being viewed by others


Introduction
Retroperitoneal lymphocele, a rare condition, develops infrequently in association with abdominal trauma, renal transplantation, and abdominal aortic surgery as well as lumbar spine surgery. An extensive occlusion in the lymphatic duct adjacent to the lumbar spine may result in the development of the rare clinical condition. However, in the majority of cases, such complication may not occur in patients with lumbar spine fracture or fracture dislocation.
We describe an unusual surgical case of retroperitoneal lymphocele following blunt ureteral and lumbar spine injuries, which caused the significant symptomatic spinal instability.
Case presentation
A 71-year-old previously healthy man sustained a blunt trauma to the right-side abdominal and lumbar spine areas in a traffic accident. The patient was transferred to the local hospital. Clinical examination suggested right ureteral injury, but no surgical exploration followed. The radiograph did not show distinctive evidence of a lumbar spine fracture or fracture dislocation because there were highly degenerative changes in the injured area (Figure 1). Therefore, the diagnosis of lumbar spine fracture at the L4 level was made afterward. However, abdominal discomfort continued, and repeated imaging showed urine collection within and outside the right-side kidney as well as the formation of a cystic lesion contiguous with the vertebral column at the L3–L4 level. At 1 month after the injury, a small-incision laparotomy was performed on the right side under the tentative diagnosis of retroperitoneal abscess without any distinctive evidence of a pyogenic lesion, but no major abnormalities were found in the right-side ureter or the retroperitoneal space. The patient was transferred to the Orthopaedic Service of our University Hospital 2 months after the injury because of increasing abdominal and lower back pain.

Lateral plain radiograph showing L4 vertebral fracture (arrow)
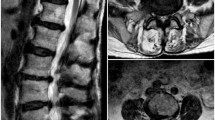
On admission, the patient complained of significant intractable low back pain and was unable to ambulate because of the pain. Neurological status was normal, and blood tests as well as blood chemistry were normal. The radiographs demonstrated the abnormal widening of the intervertebral disc space at the L3–4 level anteriorly (Figure 2). Magnetic resonance imaging revealed right-side hydronephrosis and a large fluid collection (Figure 3a) at the L3–L4 level. The cystic lesion within the iliopsoas muscle appeared contiguous with a similar lesion within the intervertebral disc space and vertebral bodies (Figure 3b). A provisional diagnosis of the right-side ureteral injury and an iliopsoas abscess at L3–L4 levels was made.

Lateral plain radiograph showing abnormal anterior widening of the intervertebral disc space at the L3–4 level, with prominent osteophytes. 3, L3 vertebra

Magnetic resonance imaging (TR, 4000 ms; TE, 80 ms) showed a large cystic fluid collection within the iliopsoas muscle at the L3–L4 and hydronephrosis on the right. (a) The intra-muscular cystic lesion seems to be connected to a similar intradiscal mass (arrow). (b) The cystic lesion invaded the degenerated intervertebral disc (arrow). 3, L3 vertebra
The patient underwent an operation, 6 days after admission; the right-sided retroperitoneal approach was used. Blunt dissection of the ureter was performed to the level of the kidney. The right-side ureter was significantly adhered to the retroperitoneal tissue between the level distal to the kidney and L3–L4 vertebrae. However, no obvious rupture of the ureter was apparent, so that the end-to-end suture of the ureter was considered to be impossible. Thus, the ureter was repaired using intraureteral catheterization. The iliopsoas muscle, which was anterior to the ureter, showed partial bulging at the L3–L4 level. Careful blunt dissection of the muscle fibers disclosed the presence of a cyst, which contained abundant fluid with the content consistent with that of serum (Figure 4a). No pus was drained from the cystic lesion. Complete resection of the intramuscular cyst was followed by thorough resection of the cystic and granulation tissue within the intervertebral disc at the L3–4 level (Figure 4b). The significant instability at the L3–L4 level was evident possibly due to the extensively developed granulation tissue within the intervertebral disc. Autologous iliac bone grafting followed without usage of artificial implants, because a pyogenic condition was not completely excluded despite no evidence of it in blood tests. The external fixation was obtained using a thoracolumbosacral orthosis. Histopathological examination demonstrated that the cyst wall contained dense fibrous tissue, aggregates of chronic inflammatory cells, but no endothelial cell lining and scarce muscle fibers (Figure 5). The final diagnosis was retroperitoneal lymphocele.

Intraoperative photographs. (a) The right-side iliopsoas muscle showed local bulging (arrow). (b) A cystic lesion within the disc space was resected (arrow). 3, L3 vertebra. 4, L4 vertebra

A photomicrograph showing the cyst wall contained dense fibrous tissue, no endothelial cell lining, and aggregates of chronic inflammatory cells (Hematoxylin and eosin × 25)
The postoperative course was uneventful. Resolution of low back pain was prompt. The patient was allowed to walk on the third postoperative day and was discharged 2 weeks later. The patient returned to work 2 months after surgery, and a bone graft union was completed 3 months postoperatively. At the 1-year follow-up, the patient was doing very well without any low back pain or renal dysfunction.
Discussion
Almost all lumbar vertebral injuries are treated without any concern for injury to the abdominal lymphatic duct.1 The lymphatic duct nest is very complex and the fluid is believed to flow very well even in the presence of partial obstruction.2 A major injury or an operation to the abdominal lymphatic duct may cause a large cystic lesion.3, 4, 5, 6 A small lymphatic fluid collection could develop after compression fractures of the lumbar spine without dislocation. However, it is abnormal that a huge lymphocele lesion developed to the extent of causing vertebral erosion with symptomatic spinal instability despite the absence of major osseous vertebral injury.
Considering the development of a huge retroperitoneal lymphocele, one must think carefully about the following: the presence of blunt ureteral injury and minimal leakage of urine, a significant cicatrix formation at the level of ureteral injury, the possible presence of a minor lymphatic duct injury, and a large anterior vertebral osteophyte.
The major rupture of the right-side ureter was absent at the time of injury, but the initial laparotomy enhanced scar formation at the site of the blunt injury. The cicatrix tissue was considered to be the cause of hydronephrosis on the right-side kidney. Furthermore, the cicatrix tissue affected the normal lymphatic fluid flow. Reviewed carefully, the radiographs taken at the time of trauma revealed a minor end plate fracture at the anterior column of L4. Furthermore, a large osteophyte formation in the anterior part of the L3 and L4 levels was noted. It is possible that the right-side lymphatic duct injury occurred at that level, and a significantly developed cicatrix tissue proximal to the suspected lymphatic duct injury site could have affected the lymphatic fluid flow, resulting in the development of the lymphocele. The lymphocele also invaded the degenerated intervertebral disc to erode the disc tissue. Thus, the lymphocele with its lesion developing in the shape of an hourglass contributed to the mechanical and symptomatic instability at the L3–L4 level.
The gold standard method for detecting a lymph leak is lymphangiography; however, it is an invasive procedure associated with some risks, including skin necrosis, infection, and pulmonary embolization.7 The recommended treatment of the retroperitoneal lymphocele is tapping and drainage of the retroperitoneal collection.8, 9 In our patient, however, as mentioned above, the L3–L4 level was considered to be significantly unstable before surgery and there was a suspicion of the occult ureteral injury causing hydronephrosis. Therefore, the surgical strategy should include repair of the ureter when the obvious rupture is present, lumbar spine stabilization at the L3–L4 level, and resection of the lymphocele lesion. In thoracic duct injury, a low-fat diet is maintained to decrease the flow of lymph. Lymph drainage above the cisterna chyli is rich in chylomicrons and has a creamy white appearance because of the contribution of gastrointestinal lymphatics. Lymph is then transported via the thoracic duct to the venous system. Below the cisterna chyli, lymph is serous in nature, has a clear yellow color, and has a significantly lower triglyceride content. In our case, the serous that had a clear yellow color was drained. Therefore a low-fat diet was not administered, because it would do little to decrease the flow of lymph arising primarily from the lower extremities.
Although the current case is extremely rare, one should be aware of possible complications such as retroperitoneal lymphocele following a blunt trauma to the abdominal area.
References
Hanson D, Mirkovic S . Lymphatic drainage after lumber surgery. Spine 1997; 8: 956–958.
Mizuno K, Matsuda M, Kuzuya A . Retroperitoneal lymphocele following ruptured abdominal aortic aneurysm repair. Jpn J Vasc Surg 2003; 12: 541–544.
Garrett H, Richardson J, Howard H . Retroperitoneal lymphocele after abdominal aortic surgery. J Vasc Surg 1989; 10: 245–253.
Hart AKE et al. Thoracic duct injury during anterior cervical discectomy: a rare complication. J Neurosurg 1998; 88: 151–154.
Stubbe F, Terpstra J . Chylous ascites after resection of an abdominal aortic aneurysm. Arch Chir Neerl 1979; 31: 111–113.
Jeffrey S, Jack P . The rationale for surgical treatment of mesenteric and retroperitoneal cysts. Am Surg 1994; 60: 432–435.
Allan DO . Treatment of a retroperitoneal lymphocele after lumber fusion surgery with intralesional povidone iodine: Technical case report. Neurosurgery 1999; 45: 658–661.
Kinouth J et al. Primary lymphedema. Clinical and lymphangiographic studies of a series of 107 patients in which the lower limbs were affected. Br J Surg 1957; 45: 1–10.
Blessios G et al. Laparoscopic management of large retroperitoneal lymphoceles complicating aortic surgery. Surg Endosc 2002; 16: 218.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Sato, R., Kobayashi, S., Uchida, K. et al. Retroperitoneal lymphocele associated with lumbar spine fracture: report of an unusual case. Spinal Cord 43, 687–690 (2005). https://doi.org/10.1038/sj.sc.3101775
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101775
Keywords
This article is cited by
-
Delayed lymphocele formation following lateral lumbar interbody fusion of the spine
European Spine Journal (2017)
