
Abstract
Trends in the incidence of classic Kaposi's sarcoma in the Jewish population in Israel for the period between 1960 and 1998 were analysed. World standardised incidence rates of 20.7 and 7.5 per million among men and women, respectively, were calculated. The highest incidence rates were displayed by men originated from Africa and by Asian-born women.
Similar content being viewed by others

Main
Kaposi's sarcoma (KS) is a multifocal vascular tumour that predominantly presents as a multipigmented sarcoma of the skin. Classic Kaposi's sarcoma (CKS) is known as a clinicoepidemiological indolent variant of the disease primarily affecting the elderly (Sarid et al, 1999; Antman and Chang, 2000). Kaposi's sarcoma-associated herpesvirus (KSHV), also known as human herpesvirus 8 (HHV-8), is believed to be a major causative factor for all clinical variants of KS (Chang et al, 1994; Ablashi et al, 2002). In general, the seroprevalence rates of KSHV in different geographical regions correlate with the incidence rates of CKS (Gao et al, 1996; Chatlynne and Ablashi, 1999; Schulz, 1999; Antman and Chang, 2000). Yet, genetic and/or environmental cofactors affecting the risk of CKS after KSHV infection probably play an important role, and thus may modify the relationship between the seroprevalence of KSHV and incidence of KS (Ariyoshi et al, 1998; Goedert et al, 2002; Grossman et al, 2002).
The objective of the present study was to investigate the trends in the incidence of CKS in Israeli Jews between 1960 and 1998. The analysis of the trends of CKS in Jews living in Israel is unique, Israel being one of the countries with the highest incidence of CKS in the world, and a migration center for Jews from various countries of origin.
Methods
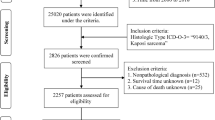
All KS cases reported to the population-based Israel Cancer Registry (ICR) between 1960 and 1998 were identified under skin cancer and sarcoma codes according to the International Classification of Diseases for Oncology Version 2 (ICD-O-2) morphology code 9140 (World Health Organization, 1979). ICR covers the entire Israeli population, and data quality is estimated to be high (Steinitz, 1989; Parkin et al, 1997). All recorded diagnoses were manually checked for registration accuracy; no misclassifications were found. No cases were reported on post mortem. KS cases that were diagnosed among immigrants before their arrival to Israel, among the Arab population, and in nonresidents were excluded. To identify the AIDS-associated KS, the ICR file was linked with the national HIV-seropositive and AIDS registries; 60 HIV-seropositive KS cases were excluded. The registry of HIV and AIDS cases in Israel is incomplete, due to the mandatory identification requirement. Yet, we believe that the majority of AIDS-KS cases are diagnosed and reported following their application for medical care.
ICR is linked to the Israel Population Registry, and receives information of date and country of birth, gender, immigration and mortality. Therefore, data retrieved from the ICR included these records, date of CKS diagnosis and topographical ICD-O codes. Using population data from the Population Registry at the National Bureau of Statistics (Central Bureau of Statistics, 1960–1998), age-, sex- and country of origin-specific incidence rates were calculated, as were age-standardised incidence rates, using the world standard population as a reference. Linear regression multivariate analysis was used to model incidence rates with respect to calendar period, age at diagnosis, gender and country or continent of origin (Breslow and Day, 1987).
Results
A total of 2107 cases of CKS (1475 men, 632 women, M/F=2.33) were registered in the entire Israeli Jewish population, during the 39-year study period (1960–1998).
Overall, the age-standardised incidence rates of CKS (±s.d.) in the Jewish population were 20.7 (±9.3) per million among men and 7.5 (±3.4) per million in women. The gender incidence ratio was 2.76 (RR=2.76 (20.7/7.5); 95% CI 1.57–3.95) and was rather constant during the study period (range 2.3–3.4). The total number of CKS cases for both genders combined for consecutive 10-year periods of diagnosis was 81 (3.8% of total cases) between 1960 and 1969, steeply increased to 396 cases between 1970 and 1979 (18.8%), followed by 574 cases (27.2%) between 1980 and 1989. A second substantial increase was observed during the period between 1990 and 1998, with 1056 new cases (50.1%). No significant trend in incidence was observed during other periods (Table 1).
A significant trend of increase in the mean age at diagnosis, in both genders, was evident. This might be due to the extended lifespan. In men, the mean age (±s.d.) increased from 64.9 (±13.2) to 69.5 (±13.9) during the period between 1960 and 1998 (P<0.01). In women, there was an even more pronounced increase in the mean age at diagnosis (±s.d.), from 51.9 (±18.1) to 73.5 (±12.7) (P<0.01). The age-specific rates increased from 10.2 per million in men and 2.5 per million in women in the age group of 35–44, to 300.8 per million in men and 119.2 per million in women in the age group of 75 or more. Among the age group of 0–24, the rates per million were 0.6 and 0.2 in males and females, respectively, with no cases recorded below 5 years of age (Table 2). The substantial increase with age in the age-specific rates of CKS cases is consistent with other reports (Cottoni et al, 1996; Hjalgrim et al, 1996; Brenner et al, 2002).
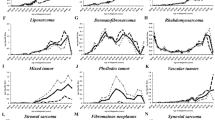
Immigrants born in Asia, Africa, Europe and America exhibited a strong increase in incidence rates during the late 1960s and the early 1970s, and during the early 1990s. Israel-born Jews demonstrated a similar increase in incidence during the late 1960s and the early 1970s but failed to show the second strong increase during the 1990s.
Analysis of CKS incidence rates by continent of origin revealed highly significant (P<0.01) differences in incidence rates (Table 3). Overall, the Jews born in Africa demonstrated the highest incidence rates in men and the second for women, followed by high rates in Asian-born Jews. Few cases were registered for Jews originating from America.
Standardised ratio and relative risks (RRs) for specific representative countries of origin could be calculated only for the period between 1980 and 1994, with Jews born in Israel taken as reference (Table 4). Prior to and after 1980–1994, the data received from the Population Registry were gathered as groups of countries that could not be separated. In men, the highest incidence rate was observed among immigrants from Romania. In women, the highest incidence rate was observed among immigrants from Iraq.
Discussion
The present study, based on 2107 registered CKS cases among Jewish residents of Israel, has found an age-standardised incidence rate of CKS (±s.d.) of 20.7 (±9.3) per million among men and 7.5 (±3.4) per million in women. Similar rates of CKS were reported, for much narrower calendar periods, from Sardinia (Cottoni et al, 1996) and Sicily (Geddes et al, 1994). A rather constant gender ratio of 2.33 was found, which is in agreement with previous population-based surveys (Biggar et al., 1984; Dictor and Attewell, 1988; Grulich et al., 1992; Geddes et al, 1994).
Here we report higher rates compared with those previously reported for the Israeli Jewish population for the period 1961–1989 (16.9 per million in men and 6.3 per million in women), in which a total of 1098 cases of CKS were analysed (Iscovich et al, 1998). The higher rates described in our study can be explained by the addition of 1009 new CKS cases and by the vast changes in the Jewish population composition with the mass migration of approximately 1 000 000 new immigrants from the Former Soviet Union (FSU) during the late 1980s and the 1990s.
The present study demonstrates two steep rises in incidence. A similar pattern of increase in incidence rates during the early 1970s was described (Hjalgrim et al, 1996; Dictor and Attewell, 1988). Improved registration is likely to have played a certain role, but it cannot be the sole explanation for this finding. Differences in immigration patterns in Israel may provide another explanation. During the 1950s through the late 1960s, there were large immigration waves from Iraq and North African countries, and during the late 1960s and early 1970s there were large immigration waves from Eastern Europe.
The increase in incidence rates during the early 1990s can be explained by the fact that CKS is a slowly developing disease, and similar to other chronic diseases, migrants are more likely to be diagnosed with such disorders, as a result of entering a new health system. An additional explanation for this increase might be the aging of the population that arrived with the large immigration waves to Israel during the 1950s and the 1960s. Moreover, this could also be explained by the massive immigration wave from the FSU. Interestingly, the majority of the newly diagnosed cases of CKS between 1990 and 1998 were among Jews of East European origin, whereas CKS incidence rates between 1990 and 1998 were higher for Jews originating from Africa and Asia, despite the much lower number of newly diagnosed cases among them.
The significant difference in incidence rates by countries of origin suggests an important role for geographical differences in the prevalence of KSHV (Chatlynne and Ablashi, 1999; Schulz, 1999). Variation in KSHV seroprevalence among Israeli populations was found to be strongly associated with the country of birth (Davidovici et al, 2001). The highest rates of anti-KSHV antibodies were found in those born in North African countries, and the lowest rates were found in those born in Europe or North America (Davidovici et al, 2001). These findings correlate with the particularly high incidence of CKS observed in our study among North African Jewish immigrants in Israel.
In summary, our study supports an important role for the country of origin, which, together with environmental conditions, is likely to be of importance in influencing the exposure of individuals to KSHV, and may also be implicated in establishing the risk for the development of CKS. Furthermore, it could be possible that the seroprevalence rates of KSHV and CKS incidence rates among the various Israeli subpopulations reflect the situation in the countries of origin, and thus our population may serve as an ‘indicator population’. Still, since CKS that was originally described in Jews of eastern European descent is also highly prevalent in Jews from Asia and Africa, it may suggest that infection with KSHV had been relatively more prevalent among Jews before the Diaspora of Jewish people that started more than 2500 years ago.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Ablashi DV, Chatlynne LG, Whitman Jr JE, Cesarman E (2002) Spectrum of Kaposi's sarcoma-associated herpesvirus, or human herpesvirus 8, diseases. Clin Microbiol Rev 15: 439–464
Antman K, Chang Y (2000) Kaposi's sarcoma. N Engl J Med 342: 1027–1038
Ariyoshi K, Schim vdL, Cook P, Whitby D, Corrah T, Jaffar S, Cham F, Sabally S, O'Donovan D, Weiss RA, Schulz TF, Whittle H (1998) Kaposi's sarcoma in the Gambia, West Africa is less frequent in human immunodeficiency virus type 2 than in human immunodeficiency virus type 1 infection despite a high prevalence of human herpesvirus 8. J Hum Virol 1: 193–199
Biggar RJ, Horm J, Fraumeni Jr JF, Greene MH, Goedert JJ (1984) Incidence of Kaposi's sarcoma and mycosis fungoides in the United States including Puerto Rico, 1973–81. J Natl Cancer Inst 73: 89–94
Brenner B, Weissmann-Brenner A, Rakowsky E, Weltfriend S, Fenig E, Friedman-Birnbaum R, Sulkes A, Linn S (2002) Classical Kaposi sarcoma: prognostic factor analysis of 248 patients. Cancer 95: 1982–1987
Breslow NE, Day NE (1987) Statistical Methods in Cancer Research. Vol. II – The Design and Analysis of Cohort Studies 82: 1–406. Lyon: IARC Sci Publ
Central Bureau of Statistics: Annual Statistics Abstracts of Israel, series 11–49 (1960–1998). Jerusalem: Central Bureau of statistics
Chang Y, Cesarman E, Pessin MS, Lee F, Culpepper J, Knowles DM, Moore PS (1994) Identification of herpesvirus-like DNA sequences in AIDS-associated Kaposi's sarcoma. Science 266: 1865–1869
Chatlynne LG, Ablashi DV (1999) Seroepidemiology of Kaposi's sarcoma-associated herpesvirus (KSHV). Semin Cancer Biol 9: 175–185
Cottoni F, De Marco R, Montesu MA (1996) Classical Kaposi's sarcoma in north-east Sardinia: an overview from 1977 to 1991. Br J Cancer 73: 1132–1133
Davidovici B, Karakis I, Bourboulia D, Ariad S, Zong J, Benharroch D, Dupin N, Weiss R, Hayward G, Sarov B, Boshoff C (2001) Seroepidemiology and molecular epidemiology of Kaposi's sarcoma-associated herpesvirus among Jewish population groups in Israel. J Natl Cancer Inst 93: 194–202
Dictor M, Attewell R (1988) Epidemiology of Kaposi's sarcoma in Sweden prior to the acquired immunodeficiency syndrome. Int J Cancer 42: 346–351
Gao SJ, Kingsley L, Li M, Zheng W, Parravicini C, Ziegler J, Newton R, Rinaldo CR, Saah A, Phair J, Detels R, Chang Y, Moore PS (1996) KSHV antibodies among Americans, Italians and Ugandans with and without Kaposi's sarcoma. Nat Med 2: 925–928
Geddes M, Franceschi S, Barchielli A, Falcini F, Carli S, Cocconi G, Conti E, Crosignani P, Gafa L, Giarelli L (1994) Kaposi's sarcoma in Italy before and after the AIDS epidemic. Br J Cancer 69: 333–336
Goedert JJ, Vitale F, Lauria C, Serraino D, Tamburini M, Montella M, Messina A, Brown EE, Rezza G, Gafa L, Romano N (2002) Risk factors for classical Kaposi's sarcoma. J Natl Cancer Inst 94: 1712–1718
Grossman Z, Iscovich J, Schwartz F, Azizi E, Klepfish A, Schattner A, Sarid R (2002) Absence of Kaposi sarcoma among Ethiopian immigrants to Israel despite high seroprevalence of human herpesvirus 8. Mayo Clin Proc 77: 905–909
Grulich AE, Beral V, Swerdlow AJ (1992) Kaposi's sarcoma in England and Wales before the AIDS epidemic. Br J Cancer 66: 1135–1137
Hjalgrim H, Melbye M, Pukkala E, Langmark F, Frisch M, Dictor M, Ekbom A (1996) Epidemiology of Kaposi's sarcoma in the Nordic countries before the AIDS epidemic. Br J Cancer 74: 1499–1502
Iscovich J, Boffetta P, Winkelmann R, Brennan P, Azizi E (1998) Classic Kaposi's sarcoma in Jews living in Israel, 1961–1989: a population-based incidence study. AIDS 12: 2067–2072
Parkin DM, Whelan SL, Ferlay J, Raymond L, Young J (1997) Cancer Incidence in Five Continents, Vol. VII, 143: 1–1240. Lyon: IARC Sci Publ
Sarid R, Olsen SJ, Moore PS (1999) Kaposi's sarcoma-associated herpesvirus: epidemiology, virology, and molecular biology. Adv Virus Res 52: 139–232
Schulz TF (1999) Epidemiology of Kaposi's sarcoma-associated herpesvirus/human herpesvirus 8. Adv Cancer Res 76: 121–160
Steinitz R, Parkin D, Young J, Bieber C, Katz L, Steinitz RPDMYJLBCAaKL (1989), In Cancer Incidence in Jewish Migrants to Israel, 1961–1981 98: 1–311. Lyon: IARC Sci. Publ
World Health Organization: International Classification of Diseases for Oncology, version (1979). Geneva: World Health Organization
Acknowledgements
This study was supported by the Israel Cancer Association and by the Middle East Cancer Consortium (MECC).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Guttman-Yassky, E., Bar-Chana, M., Yukelson, A. et al. Epidemiology of classic Kaposi's sarcoma in the Israeli Jewish population between 1960 and 1998. Br J Cancer 89, 1657–1660 (2003). https://doi.org/10.1038/sj.bjc.6601313
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6601313
Keywords
This article is cited by
-
Classic Kaposi's sarcoma in morocco: clinico -epidemiological study at the national institute of oncology
BMC Dermatology (2011)
-
Seroprevalence of Human herpesvirus 8 (HHV-8) and incidence of Kaposi's sarcoma in Iran
Infectious Agents and Cancer (2011)
-
Classic Kaposi's sarcoma in Italy, 1985–1998
British Journal of Cancer (2005)
