
Abstract
Frequency of a BRAFV600E mutation in anaplastic thyroid carcinoma, which is thought to be derived mainly from papillary carcinoma by multi-step carcinogenesis, is much lower than that in papillary carcinomas. To clarify this phenomenon, we analysed BRAFV600E mutation in 20 cases of anaplastic carcinoma and 13 accompanying differentiated carcinomas. Among twenty cases of anaplastic carcinomas, nine and four accompanied papillary and follicular carcinomas, respectively. BRAFV600E mutation was found in four (20%) cases. BRAFV600E mutation was found in three of nine (33.3%), none of four and one of seven (14.3%) anaplastic carcinomas with papillary carcinoma, follicular carcinoma and without differentiated components, respectively. All three papillary carcinomas accompanied by anaplastic carcinoma with a BRAFV600E mutation were also shown to have a BRAFV600E mutation. In summary, BRAFV600E mutation was occasionally observed in anaplastic carcinomas with papillary carcinoma, and the low frequency of BRAFV600E mutation in anaplastic carcinoma was thought to be due to the low frequency of anaplastic carcinomas with papillary carcinoma. These findings raise a question about the classical model of anaplastic transformation and suggest some roles of thyroid cancer stem cells in the generation of anaplastic carcinoma.
Similar content being viewed by others
Main
Thyroid carcinomas are thought to be generated from normal thyroid follicular cells (thyrocytes) by multi-step carcinogenesis (Farid et al, 1994). According to this hypothesis, anaplastic carcinomas are generated from both follicular and papillary carcinomas by genomic changes, such as mutations in TP53. Follicular carcinomas are generated from follicular adenomas, while papillary carcinomas are derived from some unknown precursor cells that are generated from normal thyrocytes. Recently, a somatic point mutation in the BRAF gene has been identified as the most common genetic event in papillary thyroid carcinoma (Kimura et al, 2003). Most of the tumours with a mutation harboured a thymine-to-adenine transversion at nucleotide position 1799, which results in a valine-to-glutamic acid substitution at residue 600 (V600E). Previous reports indicated that BRAF mutations in thyroid tumours are generally restricted to papillary carcinoma, and usually there is no mutation in other types of well-differentiated thyroid cancers, including follicular carcinoma, Hürthle carcinoma and medullary carcinoma, as well as in benign thyroid tumours. The frequency of the mutations in papillary carcinomas is ranged from 29 to 83% of papillary carcinoma (Xing, 2005).
It remains controversial whether this gene is also mutated in anaplastic thyroid carcinomas. In iodine-sufficient areas such as Japan, papillary carcinoma accounts for 90% of thyroid differentiated carcinomas and follicular carcinoma is rare (Hay, 1990). When multi-step carcinogenesis is taken into account, a considerable number of anaplastic carcinomas with BRAF mutations should be found. In previous reports, however, the frequency of the BRAF mutation was only about 10% on average and ranged from 0 to 63% (Fukushima et al, 2003; Namba et al, 2003; Nikiforova et al, 2003; Begum et al, 2004; Soares et al, 2004; Xing et al, 2004; Quiros et al, 2005). Among these studies, some reported that the BRAF mutation is found frequently only in anaplastic carcinomas with a papillary carcinoma component, although these studies have examined only four or five cases. A study examining a larger number of samples is essential to clarify the role of the BRAF mutation in anaplastic carcinoma.
Considering these facts, we examined BRAFV600E mutation in 20 anaplastic carcinomas and 13 accompanying differentiated carcinomas and found a low frequency of BRAFV600E mutation in anaplastic carcinomas due to the low frequency of anaplastic carcinomas accompanied by papillary carcinoma.
Materials and methods
Twenty anaplastic carcinomas were used in this study. Among these cases, nine accompanied papillary carcinoma and four accompanied follicular carcinoma. Twenty papillary carcinomas without an undifferentiated component were also examined. These tumours were surgically resected at Kuma Hospital after obtaining the patient's informed consent. The experimental protocol was approved by the local ethical committee. Paraffin-embedded tissues were microdissected to separately study well-differentiated and anaplastic areas within the same tumour nodule. For microdissection, 8 μm sections from a paraffin-embedded tissue were put on glass slides and weakly stained with haematoxylin and eosin. The areas of interest (approximately up to 0.5 cm2) were microdissected using the AS LMD (Leica, Tokyo, Japan). Genomic DNA was isolated using a QIAamp DNA Mini Kit (Qiagen, Tokyo, Japan). Ten microlitres of DNA extracted from each tumour sample was examined by direct sequencing after amplification by polymerase chain reaction (PCR). To avoid carryover contamination, Platinum Quantitative PCR SuperMix-UDG (Invitrogen Japan, Tokyo, Japan) was used for PCR amplification. Fifty microlitres of PCR mixture contained 0.5 μ M of each primer, 1 μl of 50 mM magnesium chloride, 10 μl of extracted DNA and 25 μl of Platinum Quantitative PCR SuperMix-UDG. The primers used were
BRF: 5′-ACTCTTCATAATGCTTGCTCTGATAG -3′ and
BRR: 5′-CTGATGGGACCCACTCCA -3′
The PCR conditions were 50°C for 2 min, 95°C for 2 min and 40 cycles of 95°C for 15 s and 60°C for 1 min. The PCR products were separated on agarose gel and extracted with a QIAquick Gel Extraction Kit (Qiagen). Purified fragments were sequenced using a BigDye Terminator Cycle Sequencing FS Ready Reaction Kit with an ABI PRISM 310 Genetic Analyzer (Applied Biosystems, Tokyo, Japan).
Results
The results of the mutation analysis are summarised in Tables 1 and 2. BRAFV600E mutation was found in 4 (20%) of 20 anaplastic carcinomas and in 9 (45%) of 20 papillary carcinomas without an anaplastic carcinoma examined as controls.
Among the 20 cases of anaplastic carcinomas, 9 and 4 were accompanied by papillary and follicular carcinomas, respectively. BRAFV600E mutation was found in three of nine (33.3%) anaplastic carcinomas accompanied by papillary carcinoma, none of four anaplastic carcinomas accompanied by follicular carcinoma and one of seven (14.3%) anaplastic carcinomas without differentiated components. All three papillary carcinomas accompanied by anaplastic carcinoma with a BRAFV600E mutation were also shown to have a BRAFV600E mutation, whereas there was no BRAFV600E mutation in follicular carcinomas with anaplastic carcinoma.
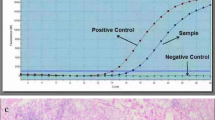
In case 9, a BRAFV600E mutation was found only in papillary carcinoma but not in coexisting anaplastic carcinoma (Figure 1). However, whether these two tumours were derived from the same precursor was not clear, since a thick connective tissue separated the two.

Haematoxylin and eosin-stained section and the results of sequencing analysis in case 9. Upper and lower panels show high (× 200) and low magnification of a section, respectively. Areas indicated by white arrows were microdissected and the sequence of the BRAF gene was analysed. A heterozygous missense mutation (T1799A/V600E) was identified in exon 15 in a papillary carcinoma sample (left) but not in a coexisting anaplastic carcinoma sample (left).
Discussion
The results of previous studies on the frequency of a BRAFV599R mutation in papillary and anaplastic carcinomas in the Japanese population are summarised in Table 3. The frequency of a BRAFV599R mutation in anaplastic carcinomas is about half of that in papillary carcinomas. It has generally been thought that most anaplastic carcinomas are derived from papillary carcinomas by accumulation of genomic damage, but if this hypothesis is true, then the present observations are difficult to explain. One possible explanation is that papillary carcinoma with BRAFV599R mutation shows a better prognosis without proceeding to anaplastic transformation. However, this theory conflicts with some previous studies showing papillary carcinomas with BRAFV599R mutation show a poor prognosis (Xing et al, 2005). Another explanation is that follicular carcinomas are more likely to transform into an anaplastic carcinoma than papillary carcinoma. In fact, nine cases of anaplastic carcinoma with a papillary component showed a high frequency of BRAFV599R mutation. This might be partly true, since even though both follicular and anaplastic carcinomas are rare in iodine-sufficient countries like Japan, many cases of anaplastic carcinoma accompanying a follicular carcinoma have been reported (Yokozawa et al, 1996; Asakawa and Kobayashi, 2002). However, in our study, there were only four cases of anaplastic carcinomas with a follicular carcinoma, which is not sufficient to explain the decreased frequency. Seven of twenty anaplastic carcinomas did not demonstrate any differentiated components and BRAFV599R mutation was detected in only one of these cases. This seems to be the major cause of the decreased frequency of a BRAFV599R mutation in anaplastic carcinomas.
The origin of anaplastic carcinoma is quite puzzling. In multi-step carcinogenesis, malignant transformation is caused by the accumulation of genomic damage in cancer cells. It is thought that anaplastic carcinoma arises by malignant transformation of coexisting papillary carcinoma. However, our present findings indicate that papillary carcinoma with BRAF mutation, which comprises a considerable percentage of differentiated thyroid carcinomas, might not be the major origin of anaplastic carcinoma. Similar phenomena are observed in other genes. Rearrangement of the RET and PAX8-PPARγ1 gene is found frequently in papillary and follicular carcinomas, respectively, but not in anaplastic carcinomas (Tallini et al, 1998; Kroll et al, 2000).
Considering these discrepancies, a new hypothesis of thyroid carcinogenesis, fetal cell carcinogenesis, in which cancer cells are derived from the remnants of fetal thyroid cells, instead of normal thyroid follicular cells, has been presented (Takano, 2004, 2007; Takano and Amino, 2005). In this hypothesis, the origins of anaplastic carcinoma are not differentiated carcinoma cells but certain kinds of fetal thyroid cells, possibly cells with a close relationship with thyroid stem cells. It is noted that in this hypothesis, the role of BRAF mutation is the prevention of immature fetal thyroid cells, namely thyroblasts that are the origins of papillary carcinomas, from differentiating into follicle-forming cells, such as follicular tumour cells or thyrocytes.
In multi-step carcinogenesis (Figure 2), the present data are explained as follows. A thyrocyte is transformed into a papillary carcinoma cell by a BRAF mutation and it is further transformed into an anaplastic carcinoma cell by a TP53 mutation. A thyrocyte without BRAF mutation is transformed into a follicular carcinoma cells and is further transformed into an anaplastic carcinoma cell by a TP53 mutation. A considerable number of anaplastic carcinomas are derived from some unknown precursors, which remain silent for many years without proliferation.

Anaplastic transformation in multi-step carcinogenesis and fetal cell carcinogenesis. In multi-step carcinogenesis (A), anaplastic carcinoma cells are generated by three pathways. A thyrocyte is transformed into a papillary carcinoma cell by a BRAF mutation, then further transformed into an anaplastic carcinoma cell. A thyrocyte without a BRAF mutation is transformed into a follicular carcinoma cells, then further transformed into an anaplastic carcinoma cell. Anaplastic carcinomas are also generated from some unknown precursors. In fetal cell carcinogenesis (B), both anaplastic and differentiated carcinoma cells are generated from thyroid cancer stem cells. A thyroid cancer stem cell with a BRAF mutation can generate anaplastic or papillary carcinoma cells but not follicular carcinoma cells, since a BRAF mutation blocks the papillary carcinoma cell from differentiating into a follicular carcinoma cell.
In fetal cell carcinogenesis, the present data are explained as follows. Both anaplastic carcinoma cells and differentiated carcinomas cells are derived from the same origin, probably thyroid cancer stem cells. In other words, thyroid cancer stem cells can produce either anaplastic carcinoma cells or differentiated cancer cells. Since a BRAF mutation blocks a papillary carcinoma cell from differentiating into follicular cells, a thyroid cancer stem cell with BRAF mutation produces anaplastic carcinoma cells and papillary carcinoma cells, but not follicular carcinoma cells. On the contrary, thyroid cancer stem cells without BRAF mutation produce anaplastic carcinoma cells and follicular carcinoma cells, since the papillary carcinoma cells that were produced further differentiate immediately into follicular cells. Occasionally, thyroid cancer stem cells maintain an undifferentiated property and proliferate without producing differentiated carcinoma cells, resulting in the formation of anaplastic carcinoma without differentiated components. Late onset of anaplastic carcinoma is easily understood when the origin of anaplastic carcinoma is a thyroid stem cell, since a stem cell can stay silent without proliferation for many years (Reya et al, 2001). Similarly, the possibility that thyroid cancer stem cells are the unknown origin of anaplastic carcinoma might also be taken into consideration in multi-step carcinogenesis.
It will be a direct proof of fetal cell carcinogenesis hypothesis when a BRAF mutation is observed only in coexisting papillary carcinoma but not in anaplastic carcinoma. Case 9 is such a case. However, the relation of these two tumours is not clear, since they were separated by a connective tissue. At least in this case, anaplastic carcinoma is not derived from coexisting papillary carcinoma but from an unknown origin. Analysing more cases in the same way may lead to the finding of similar cases with discrepant genetic alternation, since a relatively small number of cases were engaged in our and previous studies, due to the rarity of anaplastic carcinoma.
Although the mechanism of anaplastic transformation has not been understood, the recent advances in cancer research, the elucidation of cancer stem cells, may provide new perspectives that will contribute to clarifying the nature of anaplastic carcinoma. The present study may facilitate an understanding of the relation between anaplastic carcinoma and coexisting differentiated carcinomas.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Asakawa H, Kobayashi T (2002) Multistep carcinogenesis in anaplastic thyroid carcinoma: a case report. Pathology 34: 94–97
Begum S, Rosenbaum E, Henrique R, Cohen Y, Sidransky D, Westra WH (2004) BRAF mutations in anaplastic thyroid carcinoma: implications for tumor origin, diagnosis and treatment. Mod Pathol 17: 1359–1363
Farid NR, Shi Y, Zou M (1994) Molecular basis of thyroid cancer. Endocr Rev 15: 202–232
Fukushima T, Suzuki S, Mashiko M, Ohtake T, Endo Y, Takebayashi Y, Sekikawa K, Hagiwara K, Takenoshita S (2003) BRAF mutations in papillary carcinomas of the thyroid. Oncogene 22: 6455–6457
Hay ID (1990) Papillary thyroid carcinoma. Endocrinol Metab Clin North Am 19: 545–576
Kimura ET, Nikiforova MN, Zhu Z, Knauf JA, Nikiforov YE, Fagin JA (2003) High prevalence of BRAF mutations in thyroid cancer: genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma. Cancer Res 63: 1454–1457
Kroll TG, Sarraf P, Pecciarini L, Chen CJ, Mueller E, Spiegelman BM, Fletcher JA (2000) PAX8-PPARgamma1 fusion oncogene in human thyroid carcinoma [corrected]. Science 289: 1357–1360
Namba H, Nakashima M, Hayashi T, Hayashida N, Maeda S, Rogounovitch TI, Ohtsuru A, Saenko VA, Kanematsu T, Yamashita S (2003) Clinical implication of hot spot BRAF mutation, V599E, in papillary thyroid cancers. J Clin Endocrinol Metab 88: 4393–4397
Nikiforova MN, Kimura ET, Gandhi M, Biddinger PW, Knauf JA, Basolo F, Zhu Z, Giannini R, Salvatore G, Fusco A, Santoro M, Fagin JA, Nikiforov YE (2003) BRAF mutations in thyroid tumors are restricted to papillary carcinomas and anaplastic or poorly differentiated carcinomas arising from papillary carcinomas. J Clin Endocrinol Metab 88: 5399–5404
Quiros RM, Ding HG, Gattuso P, Prinz RA, Xu X (2005) Evidence that one subset of anaplastic thyroid carcinomas are derived from papillary carcinomas due to BRAF and p53 mutations. Cancer 103: 2261–2268
Reya T, Morrison SJ, Clarke MF, Weissman IL (2001) Stem cells, cancer, and cancer stem cells. Nature 414: 105–111
Soares P, Trovisco V, Rocha AS, Feijao T, Rebocho AP, Fonseca E, Vieira de Castro I, Cameselle-Teijeiro J, Cardoso-Oliveira M, Sobrinho-Simoes M (2004) BRAF mutations typical of papillary thyroid carcinoma are more frequently detected in undifferentiated than in insular and insular-like poorly differentiated carcinomas. Virchows Arch 444: 572–576
Takano T (2004) Fetal cell carcinogenesis of the thyroid: a hypothesis for better understanding of gene expression profile and genomic alternation in thyroid carcinoma. Endocr J 51: 509–515
Takano T, Amino N (2005) Fetal cell carcinogenesis: a new hypothesis for better understanding of thyroid carcinoma. Thyroid 15: 432–438
Takano T (2007) Fetal cell carcinogenesis of the thyroid: theory and practice. Sem Cancer Biol 17: 233–240
Tallini G, Santoro M, Helie M, Carlomagno F, Salvatore G, Chiappetta G, Carcangiu ML, Fusco A (1998) RET/PTC oncogene activation defines a subset of papillary thyroid carcinomas lacking evidence of progression to poorly differentiated or undifferentiated tumor phenotypes. Clin Cancer Res 4: 287–294
Xing M (2005) BRAF mutation in thyroid cancer. Endocr Relat Cancer 12: 245–262
Xing M, Vasko V, Tallini G, Larin A, Wu G, Udelsman R, Ringel MD, Ladenson PW, Sidransky D (2004) BRAF T1796A transversion mutation in various thyroid neoplasms. J Clin Endocrinol Metab 89: 1365–1368
Xing M, Westra WH, Tufano RP, Cohen Y, Rosenbaum E, Rhoden KJ, Carson KA, Vasko V, Larin A, Tallini G, Tolaney S, Holt EH, Hui P, Umbricht CB, Basaria S, Ewertz M, Tufaro AP, Califano JA, Ringel MD, Zeiger MA, Sidransky D, Ladenson PW (2005) BRAF mutation predicts a poorer clinical prognosis for papillary thyroid cancer. J Clin Endocrinol Metab 90: 6373–6379
Yokozawa T, Fukata S, Kuma K, Matsuzuka F, Kobayashi A, Hirai K, Miyauchi A, Sugawara M (1996) Thyroid cancer detected by ultrasound-guided fine-needle aspiration biopsy. World J Surg 20: 848–853;discussion 853
Acknowledgements
This research was supported by the Ministry of Education, Culture, Sports, Science and Technology of Japan, Grant-in-Aid for Scientific Research C, 2006-7, No.18590531, Research Grant of the Princess Takamatsu Cancer Research Fund 04-23606 and Foundation for Promotion of Cancer Research in Japan. We thank Shinji Morita (Kuma Hospital) for assistance with the pathological examinations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Takano, T., Ito, Y., Hirokawa, M. et al. BRAFV600E mutation in anaplastic thyroid carcinomas and their accompanying differentiated carcinomas. Br J Cancer 96, 1549–1553 (2007). https://doi.org/10.1038/sj.bjc.6603764
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6603764
Keywords
This article is cited by
-
Targeted therapy with vemurafenib in BRAF(V600E)-mutated anaplastic thyroid cancer
Thyroid Research (2023)
-
Surgical resection of the primary tumor prevents an undesirable locoregional condition and improves the quality of life in patients with anaplastic thyroid cancer
Surgery Today (2022)
-
Systemtherapie des anaplastischen Schilddrüsenkarzinoms
Die Onkologie (2022)
-
Primary Versus Secondary Anaplastic Thyroid Carcinoma: Perspectives from Multi-institutional and Population-Level Data
Endocrine Pathology (2021)
-
Coexisting well-differentiated and anaplastic thyroid carcinoma in the same primary resection specimen: immunophenotypic and genetic comparison of the two components in a consecutive series of 13 cases and a review of the literature
Virchows Archiv (2021)
