
Abstract
Objective:
To retrospectively determine if a negative 16S ribosomal RNA (rRNA) polymerase chain reaction (PCR) (PCR(−)) could lead to a decrease in the number of antibiotic doses and neonatal intensive care unit (NICU) length of stay (LOS) for infants admitted to the NICU for presumed early-onset sepsis (EOS) with negative blood culture results (BC(−)).
Study design:
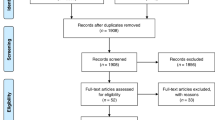
Analysis included 419 infants, greater than 35 weeks gestational age, with PCR(−), BC(−) and LOS>48 h. Both the investigators and clinical care team were unaware of the PCR results. The actual number of antibiotic doses (AAD) administered was compared to an estimated number of antibiotics doses (EAD) that would have been given until PCR(−) results were available by 18 h. The number of antibiotic doses saved was calculated as (AAD−EAD). The actual NICU LOS in hours (aLOS) for a subset of infants who remained in the hospital primarily for antibiotic therapy was compared to an estimated LOS (eLOS) if infants with PCR(−) were discharged from the NICU when clinically stable. The number of hours saved was calculated as (aLOS−eLOS).
Results:
Approximately eight antibiotic doses and 85 NICU hours per infant could be saved using PCR(−) results available at 18 h.
Conclusions:
Use of 16S rRNA PCR could decrease the number of antibiotics doses and NICU LOS for infants admitted for EOS. This may facilitate: (1) earlier NICU discharge; (2) parental satisfaction; and (3) decreased health care costs.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Escobar GJ . The neonatal ‘sepsis work-up’: personal reflections on the development of an evidence-based approach toward newborn infections in a managed care organization. Pediatrics 1999; 103 (Suppl E): 360–373.
DaSilva O, Ohlsson A, Kenyon C . Accuracy of leukocyte indices and C-reactive protein for diagnosis of neonatal sepsis: a critical review. Pediatr Infect Dis J 1995; 14: 362.
Fowlie PW, Schmidt B . Diagnostic tests for bacterial infection from birth to 90 days: a systematic review. Arch Dis Child Fetal Neonatal Ed 1998; 78: F92–F98.
Mehr S, Doyle LW . Cytokines as markers of bacterial sepsis in newborn infants: a review. Pediatr Infect Dis J 2000; 19: 879–887.
Malik A, Hui CPS, Pennie RA, Kirpalani H . Beyond the complete blood cell count & c-reactive protein: a systematic review of modern diagnostic tests for neonatal sepsis. Arch Pediatr Adolesc Med 2003; 157: 511–516.
Aronson MD, Bor DH . Blood cultures. Ann Intern Med 1987; 106: 246–253.
Kellogg JA, Ferrentino FL, Goodstein MH, Liss J, Shapiro SL, Bankert DA . Frequency of low level bacteremia in infants from birth to two months of age. Pediatr Infect Dis J 1997; 16: 381–385.
Schelonka RL, Chai MK, Yoder BA, Hensley D, Brockett RM, Ascher DP . Volume of blood required to detect common neonatal pathogens. J Pediatr 1996; 129: 275–278.
Squire E, Favara B, Todd J . Diagnosis of neonatal bacterial infection: hematologic and pathologic findings in fatal and nonfatal cases. Pediatrics 1979; 64: 60–64.
Ehrlich G . PCR-based protocols for the detection of specific organisms. In: Ehrlich GD, Greenberg SJ (eds). PCR-based Diagnostics in Infectious Disease. Blackwell Scientific Publications Inc: Cambridge, MA, 1994, pp 335–688.
Jordan JA, Durso MB . Comparison of a 16S rRNA PCR assay and an automated blood culture system in the detection of neonatal bacteremia. JCM 2000; 38: 2574–2578.
Greisen K, Loeffelholz M, Purohit A, Leong D . PCR primers and probes for the 16S rRNA gene of most species of pathogenic bacteria, including bacteria found in cerebrospinal fluid. J Clin Microbiol 1994; 32: 335–351.
Jordan JA, Durso MB . Comparison of 16S rRNA gene PCR and BACTEC 9240 for detection of neonatal bacteremia. J Clin Microbiol 2000; 38: 2574–2578.
Gerdes JS . Diagnosis and management of bacterial infections in the neonate. Pediatr Clin N Am 2004; 51: 939–959.
Pierce JR, Merenstein GB, Stocker JD . Immediate postmortem cultures in an intensive care nursery. Pediatr Infect Dis J 1984; 3: 510–513.
Schelonka RL, Yoder BA, Bradley A . The WBC count and differential: its uses and misuses. Contemp Obstet Gynecol 1996; 13: 124–166.
Santana Reyes C, Garcia-Munoz F, Reyes D, Gonzalez G, Dominguez C, Domenech E . Role of cytokines (interleukin-1β, 6, 8, tumour necrosis factor-α, and soluble receptor on interleukin-2) and C-reactive protein in the diagnosis of neonatal sepsis. Acta Pediatr 2003; 92: 221–227.
Philip AGS, Mills PC . Use of C-reactive protein in minimizing antibiotic exposure experience with infants initially admitted to a well-baby nursery. Pediatrics 2000; 106 (1): 4–8.
Madan A, Adams MM, Philip AGS . Frequency and timing of symptoms in infants screened for sepsis: effectiveness of a sepsis-screening pathway. Clin Pediatr 2003; 42 (1): 11–18.
Acknowledgements
This work was supported by the NIH Grant # HD38559. The authors gratefully acknowledge assistance in data collection by Mary Kish, RNC and database management by AI Johnson, MHA.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brozanski, B., Jones, J., Krohn, M. et al. Use of polymerase chain reaction as a diagnostic tool for neonatal sepsis can result in a decrease in use of antibiotics and total neonatal intensive care unit length of stay. J Perinatol 26, 688–692 (2006). https://doi.org/10.1038/sj.jp.7211597
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jp.7211597
Keywords
This article is cited by
-
RT-PCR detection of respiratory pathogens in newborn children admitted to a neonatal medium care unit
Pediatric Research (2013)
