
Abstract
Background:
Sedentary behaviour (SB) is an important risk factor for a number of chronic diseases. Although gaps remain in our knowledge of the elements of SB most associated with reduced health outcomes, measuring SB is important, especially in less active patient populations where treatment-related changes may be seen first in changes in SB.
Methods:
We review current published work in the measurement of SB to make recommendations for SB measurement in clinical studies.
Results:
To help move our understanding of the area forward, we propose a set of derived measures of SB that can be easily understood and interpreted.
Conclusion:
Although there is more work required to determine and validate the most clinically relevant and sensitive measures of SB, there is enough understanding of how to measure SB to enable its inclusion in study protocols.
Similar content being viewed by others



Introduction
Sedentary behaviour (SB) is defined as participation in activities such as sitting and reclining during waking hours that do not substantially increase energy expenditure.1 Recent systematic reviews have indicated that SB is associated with increased risk of chronic disease morbidity and mortality, often independent of physical activity (PA).2, 3, 4, 5, 6 Long periods of sitting are associated with increased health risks including reduced pulmonary oxygen uptake, reduced blood flow and nerve signalling, reduced fat metabolism and reduced concentration.7 These can lead to a higher risk of chronic diseases including cardiovascular disease, diabetes, kidney and liver disease. As a result, more recent public health recommendations focus on both moderate-to-vigorous PA and SB.8 Healy et al.9 showed that introducing regular interruptions in sedentary time had positive health benefits, being associated with reduced waist circumference and body mass index and improved triglyceride and plasma glucose profiles in a cohort of subjects from the Australian Diabetes, Obesity and Lifestyle (AusDiab) Study. This finding, however, has been difficult to reproduce and it is unclear whether total sedentary time, or length of sedentary bouts, is the more important risk factor.
Measuring SB using accelerometers
Initial characterisation of SB using accelerometers has focussed on periods of inactivity, and specifically periods of time where activity is recorded below a defined threshold, for example, <100 counts per minute (c.p.m.), based on the Actigraph GT3X accelerometer (ActiGraph, Pensacola, FL, USA).10 Accelerometer counts measure the frequency and intensity of accelerations and decelerations, and values are specific to each brand of monitor. Other approaches have defined SB based on energy expenditure, such as METs <1.5. Neither measure, however, differentiates sitting from quiet standing, although these are very different physiologically.11 Quiet standing is valuable to health in breaking up periods of SB. Differentiating between standing and sitting/lying is an important element of understanding and quantifying SB. For this reason, activity-based thresholds have limited value: the 100 c.p.m. threshold, for example, has been reported as only 50% accurate in detecting sedentary time in laboratory studies.12 Triaxial accelerometers have the potential to act as inclinometers to help identify body posture, dependent on wear location. Accelerometers worn on the thigh (Figure 1) provide greater ability to robustly distinguish between standing (thigh vertical) and sitting/lying (thigh horizontal) in comparison with the waist or the wrist. However, the ability to accurately detect posture via other wear positions may improve with newer devices that combine inclinometers and gyroscopes with accelerometers, although extensive supporting data has yet to be reported. Differentiating between sleep and wakeful lying is also an important consideration, although this may be beyond the scope of many accelerometer data algorithms.

Example of posture detection using a thigh-worn accelerometer: the ActivPAL (PAL Technologies, Glasgow, UK) worn under a Tegaderm dressing providing permanent waterproof attachment for a number days without removal. (a) The ActivPAL device. (b) ActivPAL thigh placement worn beneath a Tegaderm dressing. (c) Daily posture and activity summary from the ActivPAL device: 10 June 2015, worn by the author (BB): sitting/lying (yellow), quiet standing (green), stepping (red).
Accelerometer-derived outcome measures
Total sedentary time accumulated may not measure all features of SB that impact health risks. Healy et al.9 indicated that the manner in which sedentary time is accumulated influences health outcomes. However, defining clinically relevant SB bout and bout-break lengths are gaps in current research knowledge.13 In sedentary populations, small improvements in overall health status that improve the ability and motivation to perform modest discretionary activities may be better observed in the number of sedentary breaks in addition to cumulative sedentary time.
Tieges et al.14 reported three measures to describe SB from accelerometer data in their study of 96 stroke patients:
-
1
Total sedentary time (h per day), defined as uninterrupted periods of lying/sitting, expressed as a percentage of the waking wear time.
-
2
Weighted median sedentary bout length (min)—the length of the sedentary bout corresponding to 50% of daily accumulated sedentary time. For example, if 10 h of sedentary time is recorded, this measure would represent the length of the bout that contains the 5 h time-point when bouts are ordered cumulatively from smallest to largest (Figure 2).
Figure 2 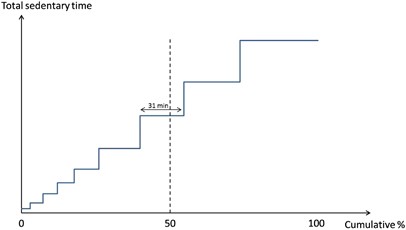
Calculating the weighted median sedentary bout length. Sedentary bouts are ordered from shortest to longest. The weighted median is represented by the length of the bout containing the 50% total sedentary time-point (in this example, 31 minutes).
-
3
Fragmentation index (/h)—the ratio of the number of sedentary bouts divided by total sedentary time.

Because the majority of sedentary bouts are very short, the mean is drawn towards the distribution tail and is an unreliable average measure. The median bout, conversely, is dominated by the large number of short bouts and has a value close to the minimum bout duration. The weighted median, however, offers a superior measure of centrality, which Chastin et al.15 identified as sensitive to detecting changes in SB following interventions in elderly volunteers and office workers.
The fragmentation index is a summary measure intended to describe the pattern of accumulation of sedentary time.14 A higher value indicates a greater number of shorter bouts, as opposed to a smaller number of prolonged periods. The fragmentation index is the inverse of the mean and may have undesirable properties—for example, the same value of 1.0 is returned for a subject with a single 1-h sedentary bout or with ten 1-h bouts.13 While an artificial illustration, it is clear that the fragmentation index can only be interpreted alongside total sedentary time.
In their study of sensitivity of different derived SB outcomes measures, Chastin et al.15 also investigated three additional statistics:
-
1
Total number of sedentary bouts (/day).
-
2
Mean period of sedentary bouts (min), the time interval between bouts.
-
3
α, the scaling parameter of the frequency distribution of bout duration, assumed to follow a power-law model.16
The properties of the power-law probability distribution are well described.17 The probability density function is represented by Equation (1), where xmin is the minimum bout length and α is the exponent of the distribution, or scaling parameter, which represents the steepness at which the distribution decays from its peak density at xmin. A lower value of α is associated with distributions that extend further and decay less rapidly, indicating subjects that tend to accumulate sedentary time with a larger proportion of longer bouts (Figure 3a).

Properties of the power-law probability distribution. (a) Effect of the scaling parameter α on the probability density function. (b) Calculation of the median from the cumulative density function.

While the scaling parameter itself is difficult to interpret, understandable outcome measures can be derived from the power-law distribution parameters including the median bout length (Equation (2) and Figure 3b) and the proportion of bouts exceeding a defined length (Equation (3)). This latter measure may be useful in assessing progress against SB interventions such as introducing standing breaks.


Use of the scale parameter, α, and its associated explanatory metrics depends on the validity of the assumed power-law distribution. Chastin and Granat16 report a good fit of this distribution in their study of 126 healthy, sedentary and chronic disease subjects, but more evidence through other data sets is needed.
Byrom and Rowe13 propose additional measures to describe SB in clinical studies, but acknowledge that more research is needed to identify the most clinically relevant measures:
-
1
Total sedentary time per day (h), standardised to a 16 h waking wear interval.
-
2
Maximum sedentary bout length per day (min).
-
3
Number of postural transitions (lying/sitting to standing/walking) per day, standardised to a 16 h waking wear interval.
The maximum bout length, while likely to be clinically relevant, may exhibit high intrasubject variability, which may limit its utility. Postural transitions are difficult to estimate using traditional inactivity measurements such as c.p.m. <100, or METs<1.5.
Importantly, accelerometer algorithms should be optimised to detect relevant postural transitions. One pediatric study found that varying the algorithm’s minimum sitting/upright period used to define transitions from 10 to 1 s did not affect the measurement of total sitting time, but did affect the number of breaks in sitting estimated.18 It concluded that a 2 s minimum sitting/upright period was optimal for estimation of breaks in sitting in children. More work in larger data sets and other subject populations is required to provide robust recommendations, but it is likely that this interval can be increased in adults and more sedentary patient populations. In the absence of other data, it may be sensible to use a value of 10 s in line with the ActivPAL default specification.19
In this review, we have considered SB as an independent variable. In reality, SB is a component of the sleep-SB-PA continuum of behaviours. New compositional analysis approaches that relate the composite of SB, light-intensity PA and moderate-to-vigorous PA to health outcomes have shown early promise in explaining other risk indicators,20 but these approaches have not yet been used in any vigour.
Recommendations
Reviewing measures previously reported, we make preliminary recommendations on accelerometer properties and outcome measure selection when studying SB.
Accelerometer properties
Accelerometers should be triaxial and provide raw acceleration data to enable postprocessing where necessary. Thigh-worn accelerometers are recommended to enable robust estimation of posture in addition to PA, although this may change with improvements of algorithms associated with wrist- and waist-worn accelerometers. The ActivPAL is currently regarded as the gold standard for measuring SB.21 In the absence of comprehensive data, we recommend postural changes to be defined using a minimum sitting/upright period of 10 s in adults.
Derived measures of SB
More research is required to determine the most clinically relevant SB measures. To help move our understanding of the area forward, we propose a set of derived measures that can be easily understood, interpreted and translated into targets (Table 1). Measures must be clinically relevant, and be able to detect change. Chastin et al.15 report Cohen d statistics, a measure of effect size relative to baseline standard deviation, for a number of SB measures using data from two small SB intervention studies. These values provide an indication of the sample size required to detect changes observed.22 While the data sets assessed did not provide a consistent picture of sensitivity to detecting change, Chastin et al.15 concluded the weighted median was consistently more sensitive than total sedentary time.
Conclusions
SB is an important risk factor for a number of chronic diseases, and its impact may be independent of moderate-to-vigorous PA. In sedentary populations such as the obese, treatment-related improvements resulting in increased ability or motivation to move around may be seen first in changes in SB as opposed to PA measures. These may correspond to important quality-of-life improvements.
Measuring SB is important in clinical research to develop health guidelines and in assessing treatment effects. It is acknowledged that more research is needed to better understand the specific properties of SB that relate to diminished health outcomes. This will lead to a greater ability to identify the most clinically relevant and sensitive measures to describe SB and its impact on health. Despite this, there is enough understanding of how to measure SB to enable its inclusion in clinical study protocols.
References
Sedentary Behaviour Research Network. Letter to the editor: standardized use of the terms 'sedentary' and 'sedentary behaviours'. Appl Physiol Nutr Metab 2012; 37: 540–542.
Healy GN, Dunstan DW, Salmon J, Shaw JE, Zimmet PZ, Owen N . Television time and continuous metabolic risk in physically active adults. Med Sci Sports Exerc 2008; 40: 639–645.
Chinapaw MJ, Proper KI, Brug J, van Mechelen W, Singh AS . Relationship between young peoples’ sedentary behaviour and biomedical health indicators: a systematic review of prospective studies. Obes Rev 2011; 12: e621–e632.
Grontved A, Hu FB . Television viewing and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: a meta-analysis. JAMA 2011; 305: 2448–2455.
Proper KI, Singh AS, van Mechelen W, Chinapaw MJ . Sedentary behaviors and health outcomes among adults: a systematic review of prospective studies. Am J Prev Med 2011; 40: 174–182.
Thorp AA, Owen N, Neuhaus M, Dunstan DW . Sedentary behaviours and subsequent health outcomes in adults. A systematic review of longitudinal studies, 1996–2011. Am J Prev Med 2011; 41: 207–215.
Dalkilinç M . Why sitting is bad for you. TEDEd 2015. Available at: http://ed.ted.com/lessons/why-sitting-is-bad-for-you-murat-dalkilinc (accessed on 30 June 2016).
UK Department of Health. Start active, stay active: a report on physical activity for health from the four home countries’ chief medical officers. Department of Health Report, July 2011.
Healy GN, Dunstan DW, Salmon J, Cerin E, Shaw JE, Zimmet PZ et al. Breaks in sedentary time: beneficial associations with metabolic risk. Diabetes Care 2008; 31: 661–666.
Freedson PS, Melanson E, Sirard J . Calibration of the Computer Science and Applications, Inc. Accelerometer. Med Sci Sports Exerc 1998; 30: 777–781.
Hamilton MT, Hamilton DG, Zderic TW . Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes 2007; 56: 2655–2667.
Steeves JA, Bowles HR, McClain JJ, Dodd KW, Brychtya RJ, Wang J et al. Ability of thigh-worn ActiGraph and activPAL monitors to classify posture and motion. Med Sci Sports Exerc 2015; 47: 952–959.
Byrom B, Rowe DA . Measuring free-living physical activity in COPD patients: deriving methodology standards for clinical trials through a review of research studies. Control Clin Trials 2016; 47: 172–184.
Tieges G, Mead M, Allerhand Z, Duncan F, van Wijck F, Fitzsimons C et al. Sedentary behavior in the first year after stroke: a longitudinal cohort study with objective measures. Arch Phys Med Rehab 2015; 96: 15–23.
Chastin SFM, Winkler EAH, Eakin EG, Gardiner PA, Dunstan DW, Owen N et al. Sensitivity to change of objectively-derived measures of sedentary behaviour. Meas Phys Educ Exerc Sci 2015; 19: 138–147.
Chastin SFM, Granat MH . Methods for objective measure, quantification and analysis of sedentary behaviour and inactivity. Gait Posture 2010; 31: 82–86.
Newman MEJ . Power laws, Pareto distributions and Zipf’s law. Contemp Phys 2005; 46: 323–351.
Alghaeed Z, Reilly JJ, Chastin SFM, Martin A, Davies G, Paton JY . The influence of minimum sitting period of the ActivPAL on the measurement of breaks in sitting in young children. PLoS One 2013; 8: e71854.
Oliver M, Schofield GM, Badland HM, Shepherd J . Utility of accelerometer thresholds for classifying sitting in office workers. Prev Med 2010; 51: 357–360.
Chastin SFM, Palarea-Albaladejo J, Dontje ML, Skelton DA . Combined effects of time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: a novel compositional data analysis approach. PLoS One 2015; 10: e0139984.
Baumgartner TA, Jackson AS, Mahar MT, Rowe DA (eds). Measurement for Evaluation in Kinesiology, 9th edn. Jones and Bartlett Learning LLC: Burlington, ON, Canada, 2016, pp 157–158.
Cohen J . Statistical Power Analysis for the Behavioral Sciences, 2nd edn. Lawrence Erlbaum: Hillsdale, NJ, USA, 1988.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/4.0/
About this article

Cite this article
Byrom, B., Stratton, G., Mc Carthy, M. et al. Objective measurement of sedentary behaviour using accelerometers. Int J Obes 40, 1809–1812 (2016). https://doi.org/10.1038/ijo.2016.136
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijo.2016.136
This article is cited by
-
Associations of objectively measured physical activity, sedentary time and cardiorespiratory fitness with adipose tissue insulin resistance and ectopic fat
International Journal of Obesity (2023)
-
Cultural adaptation, translation and validation of the Spanish version of Past-day Adults’ Sedentary Time
BMC Public Health (2021)
-
Validity and reliability of subjective methods to assess sedentary behaviour in adults: a systematic review and meta-analysis
International Journal of Behavioral Nutrition and Physical Activity (2020)
-
Temporal trends in leisure-time sedentary behavior among adolescents aged 12-15 years from 26 countries in Asia, Africa, and the Americas
International Journal of Behavioral Nutrition and Physical Activity (2020)
-
Dose-response relation of self-reported and accelerometer-measured physical activity to perceived health in middle age—the Northern Finland Birth Cohort 1966 Study
BMC Public Health (2019)
