
Abstract
Objective
:To compare clinical outcomes of premature infants on synchronized nasal intermittent positive pressure ventilation (SNIPPV) vs nasal intermittent positive pressure ventilation (NIPPV) in the neonatal intensive care unit. Use of NIPPV in the neonatal intensive care unit has shown promise with better clinical outcomes in premature neonates. It is not known if synchronization makes a significant clinical impact when using this technique.
Study Design:
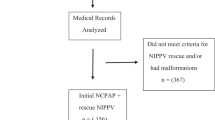
Retrospective data were obtained (1/04 to 12/09) of infants who received NIPPV anytime during their stay in the neonatal intensive care unit. SNIPPV (Infant Star with StarSync) was utilized from 2004 to 2006, whereas NIPPV (Bear Cub) was used from 2007 to 2009. Bronchopulmonary dysplasia (BPD) was defined using the NIH consensus definition. Unadjusted associations between potential risk factors and BPD/death were assessed using the χ2 or Wilcoxon rank-sum test. Adjusted analyses were performed using generalized linear mixed models, taking into account correlation among infants of multiple gestation.
Result:
There was no significant difference in the mean gestational age and birth weight in the two groups: SNIPPV (n=172; 27.0w; 1016 g) and NIPPV (n=238; 27.7w; 1117 g). There were no significant differences in maternal demographics, use of antenatal steroids, gender, multiple births, small for gestational age or Apgar scores in the two groups. More infants in the NIPPV group were given resuscitation in the delivery room (SNIPPV vs NIPPV: 44.2 vs 63%, P<0.001). Use of surfactant (84.4 vs 70.2%; P<0.001) was significantly higher in the SNIPPV group. There were no differences in the rate of patent ductus arteriosus, intraventricular hemorrhage, periventricular leukomalacia, retinopathy of prematurity and necrotizing enterocolitis in the two groups. After adjusting for the significant variables, use of NIPPV vs SNIPPV (odds ratio 0.74; 95% confidence interval: 0.42, 1.30) was not associated with BPD/death.
Conclusion:
These data suggest that use of SNIPPV vs NIPPV is not significantly associated with a differential impact on clinical outcomes.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Bhandari V . Nasal intermittent positive pressure ventilation in the newborn: review of literature and evidence-based guidelines. J Perinatol 2010; 30: 505–512.
Friedlich P, Lecart C, Posen R, Ramicone E, Chan L, Ramanathan R . A randomized trial of nasopharyngeal-synchronized intermittent mandatory ventilation versus nasopharyngeal continuous positive airway pressure in very low birth weight infants after extubation. J Perinatol 1999; 19: 413–418.
Barrington KJ, Bull D, Finer NN . Randomized trial of nasal synchronized intermittent mandatory ventilation compared with continuous positive airway pressure after extubation of very low birth weight infants. Pediatrics 2001; 107: 638–641.
Bhandari V, Gavino RG, Nedrelow JH, Pallela P, Salvador A, Ehrenkranz RA et al. A randomized controlled trial of synchronized nasal intermittent positive pressure ventilation in RDS. J Perinatol 2007; 27: 697–703.
Khalaf MN, Brodsky N, Hurley J, Bhandari V . A prospective randomized, controlled trial comparing synchronized nasal intermittent positive pressure ventilation versus nasal continuous positive airway pressure as modes of extubation. Pediatrics 2001; 108: 13–17.
Moretti C, Giannini L, Fassi C, Gizzi C, Papoff P, Colarizi P . Nasal flow-synchronized intermittent positive pressure ventilation to facilitate weaning in very low-birthweight infants: unmasked randomized controlled trial. Pediatr Int 2008; 50: 85–91.
Kugelman A, Feferkorn I, Riskin A, Chistyakov I, Kaufman B, Bader D . Nasal intermittent mandatory ventilation versus nasal continuous positive airway pressure for respiratory distress syndrome: a randomized, controlled, prospective study. J Pediatr 2007; 150: 521–526.
Sai Sunil Kishore M, Dutta S, Kumar P . Early nasal intermittent positive pressure ventilation versus continuous positive airway pressure for respiratory distress syndrome. Acta Paediatr 2009; 98: 1412–1415.
Kiciman NM, Andreasson B, Bernstein G, Mannino FL, Rich W, Henderson C et al. Thoracoabdominal motion in newborns during ventilation delivered by endotracheal tube or nasal prongs. Pediatr Pulmonol 1998; 25: 175–181.
Moretti C, Gizzi C, Papoff P, Lampariello S, Capoferri M, Calcagnini G et al. Comparing the effects of nasal synchronized intermittent positive pressure ventilation (nSIPPV) and nasal continuous positive airway pressure (nCPAP) after extubation in very low birth weight infants. Early Hum Dev 1999; 56: 167–177.
Aghai ZH, Saslow JG, Nakhla T, Milcarek B, Hart J, Lawrysh-Plunkett R et al. Synchronized nasal intermittent positive pressure ventilation (SNIPPV) decreases work of breathing (WOB) in premature infants with respiratory distress syndrome (RDS) compared to nasal continuous positive airway pressure (NCPAP). Pediatr Pulmonol 2006; 41: 875–881.
Ehrenkranz RA, Walsh MC, Vohr BR, Jobe AH, Wright LL, Fanaroff AA et al. Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia. Pediatrics 2005; 116: 1353–1360.
Papile LA, Burstein J, Burstein R, Koffler H . Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr 1978; 92: 529–534.
Volpe JJ . Intracranial hemorrhage: Germinal matrix-intraventricular hemorrhage of the premature infant In: Volpe JJ (ed). Neurology of the Newborn. 4th edn. WB Saunders: Philadelphia, 2001, pp 435–447.
Bell MJ, Ternberg JL, Feigin RD, Keating JP, Marshall R, Barton L et al. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg 1978; 187: 1–7.
Anonymous. An international classification of retinopathy of prematurity. Pediatrics 1984; 74: 127–133.
Santin R, Brodsky N, Bhandari V . A prospective observational pilot study of synchronized nasal intermittent positive pressure ventilation (SNIPPV) as a primary mode of ventilation in infants > or =28 weeks with respiratory distress syndrome (RDS). J Perinatol 2004; 24: 487–493.
Bhandari V, Finer NN, Ehrenkranz RA, Saha S, Das A, Walsh MC et al. Synchronized nasal intermittent positive-pressure ventilation and neonatal outcomes. Pediatrics 2009; 124: 517–526.
Khorana M, Paradeevisut H, Sangtawesin V, Kanjanapatanakul W, Chotigeat U, Ayutthaya JK . A randomized trial of non-synchronized nasopharyngeal intermittent mandatory ventilation (nsNIMV) vs. nasal continuous positive airway pressure (NCPAP) in the prevention of extubation failure in pre-term <1,500 grams. J Med Assoc Thai 2008; 91 (Suppl 3): S136–S142.
Kumar M, Avasthi S, Ahuja S, Malik GK, Singh SN . Unsynchronized nasal intermittent positive pressure ventilation to prevent extubation failure in neonates: a randomized controlled trial. Indian J Pediatr 2011; 78: 801–806.
Dumpa V, Northrup V, Bhandari V . Type and timing of ventilation in the first postnatal week is associated with bronchopulmonary dysplasia/death. Am J Perinatol 2011; 28: 321–330.
Chang HY, Claure N, D’Ugard C, Torres J, Nwajei P, Bancalari E . Effects of synchronization during nasal ventilation in clinically stable preterm infants. Pediatr Res 2011; 69: 84–89.
Owen LS, Morley CJ, Dawson JA, Davis PG . Effects of non-synchronised nasal intermittent positive pressure ventilation on spontaneous breathing in preterm infants. Arch Dis Child Fetal Neonatal Ed; e-pub ahead of print 20 Feruary 2011.
Garland JS, Nelson DB, Rice T, Neu J . Increased risk of gastrointestinal perforations in neonates mechanically ventilated with either face mask or nasal prongs. Pediatrics 1985; 76: 406–410.
De Paoli AG, Davis PG, Lemyre B . Nasal continuous positive airway pressure versus nasal intermittent positive pressure ventilation for preterm neonates: a systematic review and meta-analysis. Acta Paediatr 2003; 92: 70–75.
Acknowledgements
Biostatistical collaboration (KK, VN) was provided through CTSA Grant Number UL1 RR024139 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH. Information on Re-engineering the Clinical Research Enterprise can be obtained from the NIH website.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Journal of Perinatology website
Supplementary information
Rights and permissions
About this article
Cite this article
Dumpa, V., Katz, K., Northrup, V. et al. SNIPPV vs NIPPV: does synchronization matter?. J Perinatol 32, 438–442 (2012). https://doi.org/10.1038/jp.2011.117
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jp.2011.117
