
Key Points
-
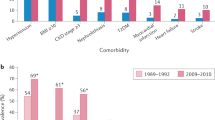
Epidemiological studies have repeatedly shown that hyperuricaemia and gout are independent risk factors for cardiovascular disease
-
Longitudinal studies have shown that serum uric acid (SUA) level is an independent risk factor for the onset and progression of kidney disease
-
The mechanisms underlying these comorbidities probably involve low-grade systemic inflammation and xanthine oxidase activity, as well as the direct deleterious effect of hyperuricaemia
-
In some patients, lowering SUA levels might decrease blood pressure and ameliorate kidney function
-
Xanthine oxidase inhibition could ameliorate cardiovascular and renal comorbidities, through its dual roles in lowering SUA levels and scavenging free radicals during uric acid formation
-
Whether reducing the systemic inflammation associated with gout might improve cardiovascular or renal outcomes remains to be determined
Abstract
Epidemiological and experimental studies have shown that hyperuricaemia and gout are intricately linked with hypertension, metabolic syndrome, chronic kidney disease and cardiovascular disease. A number of studies suggest that hyperuricaemia and gout are independent risk factors for the development of these conditions and that these conditions account, in part, for the increased mortality rate of patients with gout. In this Review, we first discuss the links between hyperuricaemia, gout and these comorbidities, and present the mechanisms by which uric acid production and gout might favour the development of cardiovascular and renal diseases. We then emphasize the potential benefit of urate-lowering therapies on cardiovascular and renal outcomes in patients with hyperuricaemia. The mechanisms that link elevated serum uric acid levels and gout with these comorbidities seem to be multifactorial, implicating low-grade systemic inflammation and xanthine oxidase (XO) activity, as well as the deleterious effects of hyperuricaemia itself. Patients with asymptomatic hyperuricaemia should be treated by nonpharmacological means to lower their SUA levels. In patients with gout, long-term pharmacological inhibition of XO is a treatment strategy that might also reduce cardiovascular and renal comorbidities, because of its dual effect of lowering SUA levels as well as reducing free-radical production during uric acid formation.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
Feig, D. I., Kang, D. H. & Johnson, R. J. Uric acid and cardiovascular risk. N. Engl. J. Med. 359, 1811–1821 (2008).
Richette, P. & Bardin, T. Gout. Lancet 375, 318–328 (2010).
Bardin, T. & Richette, P. Definition of hyperuricemia and gouty conditions. Curr. Opin. Rheumatol. 26, 186–191 (2014).
Kuo, C. F. et al. Significance of serum uric acid levels on the risk of all-cause and cardiovascular mortality. Rheumatology (Oxford) 52, 127–134 (2013).
Abbott, R. D., Brand, F. N., Kannel, W. B. & Castelli, W. P. Gout and coronary heart disease: the Framingham Study. J. Clin. Epidemiol. 41, 237–242 (1988).
Krishnan, E., Baker, J. F., Furst, D. E. & Schumacher, H. R. Gout and the risk of acute myocardial infarction. Arthritis Rheum. 54, 2688–2696 (2006).
Choi, H. K. & Curhan, G. Independent impact of gout on mortality and risk for coronary heart disease. Circulation 116, 894–900 (2007).
De Vera, M. A., Rahman, M. M., Bhole, V., Kopec, J. A. & Choi, H. K. Independent impact of gout on the risk of acute myocardial infarction among elderly women: a population-based study. Ann. Rheum. Dis. 69, 1162–1164 (2010).
Baker, J. F., Schumacher, H. R. & Krishnan, E. Serum uric acid level and risk for peripheral arterial disease: analysis of data from the multiple risk factor intervention trial. Angiology 58, 450–457 (2007).
Krishnan, E. Gout and the risk for incident heart failure and systolic dysfunction. BMJ Open 15, e000282 (2012).
Seminog, O. O. & Goldacre, M. J. Gout as a risk factor for myocardial infarction and stroke in England: evidence from record linkage studies. Rheumatology (Oxford) 52, 2251–2259 (2013).
Lottmann, K., Chen, X. & Schadlich, P. K. Association between gout and all-cause as well as cardiovascular mortality: a systematic review. Curr. Rheumatol. Rep. 14, 195–203 (2012).
Stack, A. G. et al. Independent and conjoint associations of gout and hyperuricaemia with total and cardiovascular mortality. QJM 106, 647–658 (2013).
Teng, G. G. et al. Mortality due to coronary heart disease and kidney disease among middle-aged and elderly men and women with gout in the Singapore Chinese Health Study. Ann. Rheum. Dis. 71, 924–928 (2012).
Perez-Ruiz, F. et al. Tophaceous gout and high level of hyperuricaemia are both associated with increased risk of mortality in patients with gout. Ann. Rheum. Dis. 73, 177–182 (2014).
Kim, S. Y. et al. Hyperuricemia and coronary heart disease: a systematic review and meta-analysis. Arthritis Care Res. (Hoboken) 62, 170–180 (2010).
Chen, S. Y., Chen, C. L. & Shen, M. L. Severity of gouty arthritis is associated with Q-wave myocardial infarction: a large-scale, cross-sectional study. Clin. Rheumatol. 26, 308–313 (2007).
Culleton, B. F., Larson, M. G., Kannel, W. B. & Levy, D. Serum uric acid and risk for cardiovascular disease and death: the Framingham Heart Study. Ann. Intern. Med. 131, 7–13 (1999).
Kim, S. Y. et al. Hyperuricemia and risk of stroke: a systematic review and meta-analysis. Arthritis Rheum. 61, 885–892 (2009).
Grayson, P. C., Kim, S. Y., LaValley, M. & Choi, H. K. Hyperuricemia and incident hypertension: a systematic review and meta-analysis. Arthritis Care Res. (Hoboken) 63, 102–110 (2010).
Zhang, W. et al. Plasma uric acid and hypertension in a Chinese community: prospective study and metaanalysis. Clin. Chem. 55, 2026–2034 (2009).
Gaffo, A. L. et al. Serum urate association with hypertension in young adults: analysis from the Coronary Artery Risk Development in Young Adults cohort. Ann. Rheum. Dis. 72, 1321–1327 (2013).
Loeffler, L. F., Navas-Acien, A., Brady, T. M., Miller, E. R. 3rd & Fadrowski, J. J. Uric acid level and elevated blood pressure in US adolescents: National Health and Nutrition Examination Survey, 1999–2006. Hypertension 59, 811–817 (2012).
Mazzali, M. et al. Hyperuricemia induces a primary renal arteriolopathy in rats by a blood pressure-independent mechanism. Am. J. Physiol. Renal Physiol. 282, F991–F997 (2002).
Sanchez-Lozada, L. G. et al. Mild hyperuricemia induces glomerular hypertension in normal rats. Am. J. Physiol. Renal Physiol. 283, F1105–F1110 (2002).
Choi, H. K., Ford, E. S., Li, C. & Curhan, G. Prevalence of the metabolic syndrome in patients with gout: the Third National Health and Nutrition Examination Survey. Arthritis Rheum. 57, 109–115 (2007).
Lv, Q. et al. High serum uric acid and increased risk of type 2 diabetes: a systemic review and meta-analysis of prospective cohort studies. PLoS ONE 8, e56864 (2013).
Quinones Galvan, A. et al. Effect of insulin on uric acid excretion in humans. Am. J. Physiol. 268, E1–E5 (1995).
Kodama, S. et al. Association between serum uric acid and development of type 2 diabetes. Diabetes Care 32, 1737–1742 (2009).
Viazzi, F., Leoncini, G., Vercelli, M., Deferrari, G. & Pontremoli, R. Serum uric acid levels predict new-onset type 2 diabetes in hospitalized patients with primary hypertension: the MAGIC study. Diabetes Care 34, 126–128 (2011).
Bhole, V., Choi, J. W., Kim, S. W, de Vera, M. & Choi, H. Serum uric acid levels and the risk of type 2 diabetes: a prospective study. Am. J. Med. 123, 957–961 (2010).
Onat, A. et al. Serum uric acid is a determinant of metabolic syndrome in a population-based study. Am. J. Hypertens. 19, 1055–1062 (2006).
Wang, J. Y. et al. Predictive value of serum uric acid levels for the diagnosis of metabolic syndrome in adolescents. J. Pediatr. 161, 753–756.e2 (2012).
Reungjui, S., Pratipanawatr, T., Johnson, R. & Nakagawa, T. Do thiazides worsen metabolic syndrome and renal disease? The pivotal roles for hyperuricemia and hypokalemia. Curr. Opin. Nephrol. Hypertens. 17, 470–476 (2008).
Cox, C. L. et al. Consumption of fructose- but not glucose-sweetened beverages for 10 weeks increases circulating concentrations of uric acid, retinol binding protein-4, and gamma-glutamyl transferase activity in overweight/obese humans. Nutr. Metab. (Lond.) 9, 68 (2012).
Sanchez-Lozada, L. G. et al. Fructose-induced metabolic syndrome is associated with glomerular hypertension and renal microvascular damage in rats. Am. J. Physiol. Renal Physiol. 292, F423–F429 (2007).
Perez-Pozo, S. E. et al. Excessive fructose intake induces the features of metabolic syndrome in healthy adult men: role of uric acid in the hypertensive response. Int. J. Obes. (Lond.) 34, 454–461 (2010).
Choi, H. K. & Curhan, G. Soft drinks, fructose consumption, and the risk of gout in men: prospective cohort study. BMJ 336, 309–312 (2008).
Choi, H. K., Willett, W. & Curhan, G. Fructose-rich beverages and risk of gout in women. JAMA 304, 2270–2278 (2010).
So, A. & Thorens, B. Uric acid transport and disease. J. Clin. Invest. 120, 1791–1799 (2010).
Zhu, Y., Pandya, B. J. & Choi, H. K. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007–2008. Am. J. Med. 125, 679–687.e1 (2011).
Jalal, D. I., Chonchol, M., Chen, W. & Targher, G. Uric acid as a target of therapy in CKD. Am. J. Kidney Dis. 61, 134–146 (2013).
Johnson, R. J. et al. Uric acid and chronic kidney disease: which is chasing which? Nephrol. Dial. Transplant. 28, 2221–2228 (2013).
Umekawa, T., Chegini, N. & Khan, S. R. Increased expression of monocyte chemoattractant protein-1 (MCP-1) by renal epithelial cells in culture on exposure to calcium oxalate, phosphate and uric acid crystals. Nephrol. Dial. Transplant. 18, 664–669 (2003).
Omori, H. et al. Use of xanthine oxidase inhibitor febuxostat inhibits renal interstitial inflammation and fibrosis in unilateral ureteral obstructive nephropathy. Clin. Exp. Nephrol. 16, 549–556 (2012).
Sanchez-Lozada, L. G. et al. Effects of febuxostat on metabolic and renal alterations in rats with fructose-induced metabolic syndrome. Am. J. Physiol. Renal Physiol. 294, F710–F718 (2008).
Kosugi, T. et al. Effect of lowering uric acid on renal disease in the type 2 diabetic db/db mice. Am. J. Physiol. Renal Physiol. 297, F481–F488 (2009).
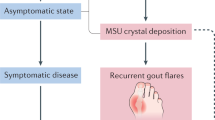
Pascual, E. Persistence of monosodium urate crystals and low-grade inflammation in the synovial fluid of patients with untreated gout. Arthritis Rheum. 34, 141–145 (1991).
Perez-Ruiz, F. Treating to target: a strategy to cure gout. Rheumatology (Oxford) 48 (Suppl. 2), ii9–ii14 (2009).
Dalbeth, N. et al. Cellular characterization of the gouty tophus: a quantitative analysis. Arthritis Rheum. 62, 1549–1556 (2010).
Schlesinger, N. et al. Canakinumab for acute gouty arthritis in patients with limited treatment options: results from two randomised, multicentre, active-controlled, double-blind trials and their initial extensions. Ann. Rheum. Dis. 71, 1839–1848 (2012).
Chowalloor, P. V. & Keen, H. I. A systematic review of ultrasonography in gout and asymptomatic hyperuricaemia. Ann. Rheum. Dis. 72, 638–645 (2013).
Pineda, C. et al. Joint and tendon subclinical involvement suggestive of gouty arthritis in asymptomatic hyperuricemia: an ultrasound controlled study. Arthritis Res. Ther. 13, R4 (2011).
Puig, J. G. et al. Asymptomatic hyperuricemia: impact of ultrasonography. Nucleosides Nucleotides Nucleic Acids 27, 592–595 (2008).
Daskalopoulou, S. S., Tzovaras, V., Mikhailidis, D. P. & Elisaf, M. Effect on serum uric acid levels of drugs prescribed for indications other than treating hyperuricaemia. Curr. Pharm. Des. 11, 4161–4175 (2005).
Kelkar, A., Kuo, A. & Frishman, W. H. Allopurinol as a cardiovascular drug. Cardiol. Rev. 19, 265–271 (2011).
Chen, X., Wu, G. & Schwarzschild, M. A. Urate in Parkinson's disease: more than a biomarker? Curr. Neurol. Neurosci. Rep. 12, 367–375 (2012).
Hershfield, M. S. et al. Treating gout with pegloticase, a PEGylated urate oxidase, provides insight into the importance of uric acid as an antioxidant in vivo. Proc. Natl Acad. Sci. USA 107, 14351–14356 (2010).
Pacher, P., Nivorozhkin, A. & Szabo, C. Therapeutic effects of xanthine oxidase inhibitors: renaissance half a century after the discovery of allopurinol. Pharmacol. Rev. 58, 87–114 (2006).
Love, B. L., Barrons, R., Veverka, A. & Snider, K. M. Urate-lowering therapy for gout: focus on febuxostat. Pharmacotherapy 30, 594–608 (2010).
Malik, U. Z. et al. Febuxostat inhibition of endothelial-bound XO: implications for targeting vascular ROS production. Free Radic. Biol. Med. 51, 179–184 (2011).
Kaptoge, S. et al. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet 375, 132–140 (2010).
Martinon, F., Petrilli, V., Mayor, A., Tardivel, A. & Tschopp, J. Gout-associated uric acid crystals activate the NALP3 inflammasome. Nature 440, 237–241 (2006).
Duewell, P. et al. NLRP3 inflammasomes are required for atherogenesis and activated by cholesterol crystals. Nature 464, 1357–1361 (2010).
Inaba, S., Sautin, Y., Garcia, G. E. & Johnson, R. J. What can asymptomatic hyperuricaemia and systemic inflammation in the absence of gout tell us? Rheumatology (Oxford) 52, 963–965 (2013).
Rothenbacher, D. et al. Relationship between inflammatory cytokines and uric acid levels with adverse cardiovascular outcomes in patients with stable coronary heart disease. PLoS ONE 7, e45907 (2012).
Kanellis, J. et al. Uric acid stimulates monocyte chemoattractant protein-1 production in vascular smooth muscle cells via mitogen-activated protein kinase and cyclooxygenase-2. Hypertension 41, 1287–1293 (2003).
Shi, Y., Evans, J. E. & Rock, K. L. Molecular identification of a danger signal that alerts the immune system to dying cells. Nature 425, 516–521 (2003).
Dinarello, C. A., Simon, A. & van der Meer, J. W. Treating inflammation by blocking interleukin-1 in a broad spectrum of diseases. Nat. Rev. Drug Discov. 11, 633–652 (2012).
Higgins, P. et al. Xanthine oxidase inhibition for the treatment of cardiovascular disease: a systematic review and meta-analysis. Cardiovasc. Ther. 30, 217–226 (2012).
Rajendra, N. S. et al. Mechanistic insights into the therapeutic use of high-dose allopurinol in angina pectoris. J. Am. Coll. Cardiol. 58, 820–828 (2011).
Noman, A., Ang, D. S., Ogston, S., Lang, C. C. & Struthers, A. D. Effect of high-dose allopurinol on exercise in patients with chronic stable angina: a randomised, placebo controlled crossover trial. Lancet 375, 2161–2167 (2010).
Thanassoulis, G., Brophy, J. M., Richard, H. & Pilote, L. Gout, allopurinol use, and heart failure outcomes. Arch. Intern. Med. 170, 1358–1364 (2010).
Grimaldi-Bensouda, L. et al. Impact of allopurinol on risk of myocardial infarction. Ann. Rheum. Dis. http://dx.doi.org/10.1136/annrheumdis-2012-202972 (2014).
Athyros, V. G. et al. Effect of statins versus untreated dyslipidemia on serum uric acid levels in patients with coronary heart disease: a subgroup analysis of the GREek Atorvastatin and Coronary-heart-disease Evaluation (GREACE) study. Am. J. Kidney Dis. 43, 589–599 (2004).
Hoieggen, A. et al. The impact of serum uric acid on cardiovascular outcomes in the LIFE study. Kidney Int. 65, 1041–1049 (2004).
George, J., Carr, E., Davies, J., Belch, J. J. & Struthers, A. High-dose allopurinol improves endothelial function by profoundly reducing vascular oxidative stress and not by lowering uric acid. Circulation 114, 2508–2516 (2006).
Ogino, K. et al. Uric acid-lowering treatment with benzbromarone in patients with heart failure: a double-blind placebo-controlled crossover preliminary study. Circ. Heart Fail. 3, 73–81 (2010).
Harzand, A., Tamariz, L. & Hare, J. M. Uric acid, heart failure survival, and the impact of xanthine oxidase inhibition. Congest. Heart Fail. 18, 179–182 (2012).
Gois, P. H. & Souza, E. R. Pharmacotherapy for hyperuricemia in hypertensive patients. Cochrane Database of Systematic Reviews, Issue 1. Art. No.: CD008652. http://dx.doi.org/10.1002/14651858.CD008652.pub2.
Agarwal, V., Hans, N. & Messerli, F. H. Effect of allopurinol on blood pressure: a systematic review and meta-analysis. J. Clin. Hypertens. (Greenwich) 15, 435–442 (2013).
Feig, D. I., Soletsky, B. & Johnson, R. J. Effect of allopurinol on blood pressure of adolescents with newly diagnosed essential hypertension: a randomized trial. JAMA 300, 924–932 (2008).
Soletsky, B. & Feig, D. I. Uric acid reduction rectifies prehypertension in obese adolescents. Hypertension 60, 1148–1156 (2012).
Sezai, A. et al. Comparison of febuxostat and allopurinol for hyperuricemia in cardiac surgery patients (NU-FLASH Trial). Circ. J. 77, 2043–2049 (2013).
Kostka-Jeziorny, K., Uruski, P. & Tykarski, A. Effect of allopurinol on blood pressure and aortic compliance in hypertensive patients. Blood Press. 20, 104–110 (2011).
Siu, Y. P., Leung, K. T., Tong, M. K. & Kwan, T. H. Use of allopurinol in slowing the progression of renal disease through its ability to lower serum uric acid level. Am. J. Kidney Dis. 47, 51–59 (2006).
Goicoechea, M. et al. Effect of allopurinol in chronic kidney disease progression and cardiovascular risk. Clin. J. Am. Soc. Nephrol. 5, 1388–1393 (2010).
Miao, Y. et al. Effect of a reduction in uric acid on renal outcomes during losartan treatment: a post hoc analysis of the reduction of endpoints in non-insulin-dependent diabetes mellitus with the Angiotensin II Antagonist Losartan Trial. Hypertension 58, 2–7 (2011).
Whelton, A., Macdonald, P. A., Zhao, L., Hunt, B. & Gunawardhana, L. Renal function in gout: long-term treatment effects of febuxostat. J. Clin. Rheumatol. 17, 7–13 (2011).
Gibson, T. J. Hypertension, its treatment, hyperuricaemia and gout. Curr. Opin. Rheumatol. 25, 217–222 (2013).
Gibson, T., Rodgers, V., Potter, C. & Simmonds, H. A. Allopurinol treatment and its effect on renal function in gout: a controlled study. Ann. Rheum. Dis. 41, 59–65 (1982).
Nidorf, S. M., Eikelboom, J. W., Budgeon, C. A. & Thompson, P. L. Low-dose colchicine for secondary prevention of cardiovascular disease. J. Am. Coll. Cardiol. 61, 404–410 (2013).
Pascual, E. & Castellano, J. A. Treatment with colchicine decreases white cell counts in synovial fluid of asymptomatic knees that contain monosodium urate crystals. J. Rheumatol. 19, 600–603 (1992).
Crittenden, D. B. et al. Colchicine use is associated with decreased prevalence of myocardial infarction in patients with gout. J. Rheumatol. 39, 1458–1464 (2012).
Nidorf, M. & Thompson, P. L. Effect of colchicine (0.5 mg twice daily) on high-sensitivity C-reactive protein independent of aspirin and atorvastatin in patients with stable coronary artery disease. Am. J. Cardiol. 99, 805–807 (2007).
Raju, N. C. et al. Effect of colchicine compared with placebo on high sensitivity C-reactive protein in patients with acute coronary syndrome or acute stroke: a pilot randomized controlled trial. J. Thromb. Thrombolysis 33, 88–94 (2012).
Muir, S. W. et al. Allopurinol use yields potentially beneficial effects on inflammatory indices in those with recent ischemic stroke: a randomized, double-blind, placebo-controlled trial. Stroke 39, 3303–3307 (2008).
Kanbay, M. et al. Effect of treatment of hyperuricemia with allopurinol on blood pressure, creatinine clearence, and proteinuria in patients with normal renal functions. Int. Urol. Nephrol. 39, 1227–1233 (2007).
Yiginer, O. et al. Allopurinol improves endothelial function and reduces oxidant-inflammatory enzyme of myeloperoxidase in metabolic syndrome. Clin. Res. Cardiol. 97, 334–340 (2008).
Acknowledgements
The authors wish to thank T. Kielstein and A. K. Tausche for helpful discussion. Editorial assistance for the preparation of this manuscript (copyediting for English language, prior to submission to the journal and before peer-review) was provided by L. Giacomelli (Content Ed Net).
Author information
Authors and Affiliations
Contributions
All authors researched data for the article and made a substantial contribution to discussion of content and writing the article. P.R. and T.B. reviewed/edited the manuscript before submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare they have received consultancy and/or speaker fees from Abbott (T.L.J.), Ardea Biosciences (F.P.-R., M.D., G.N., A.K.S., T.B.), Astra Zeneca (P.R.), Biocryst (G.N., T.B.), Ipsen (P.R., M.D., T.L.J., G.N., A.K.S., T.B.), Menarini (P.R., F.P.-R., M.D., T.L.J., G.N., E.P., A.K.S., T.B.), Metabolex (F.P.-R.), Novartis (P.R., F.P.-R., M.D., G.N., A.K.S., T.B.), Pfizer (F.P.-R.), Roche (T.L.J.), Sanofi (P.R.), Savient (P.R., F.P.-R. G.N., M.D., E.P., T.B.) and UCB (T.L.J.). F.P.-R. declares he has received grants from Ministerio de Sanidad, Gobierno de España and Asociación de Reumatólogos del Hospital de Cruces. P.R. declares he has received an educational grant from Menarini.
Rights and permissions
About this article

Cite this article
Richette, P., Perez-Ruiz, F., Doherty, M. et al. Improving cardiovascular and renal outcomes in gout: what should we target?. Nat Rev Rheumatol 10, 654–661 (2014). https://doi.org/10.1038/nrrheum.2014.124
Published:
Issue Date:
DOI: https://doi.org/10.1038/nrrheum.2014.124
This article is cited by
-
Exploring the impact of taurine on the biochemical properties of urate oxidase: response surface methodology and molecular dynamics simulation
Journal of Biological Engineering (2024)
-
Clinical effects of a selective urate reabsorption inhibitor dotinurad in patients with hyperuricemia and treated hypertension: a multicenter, prospective, exploratory study (DIANA)
European Journal of Medical Research (2023)
-
Professionals’ perspectives on existing practice and conditions for nurse-led gout care based on treatment recommendations: a qualitative study in primary healthcare
BMC Primary Care (2022)
-
Assessing the causal relationships between gout and hypertension: a bidirectional Mendelian randomisation study with coarsened exposures
Arthritis Research & Therapy (2022)
-
Excess comorbidities in gout: the causal paradigm and pleiotropic approaches to care
Nature Reviews Rheumatology (2022)
