
Abstract
Objective
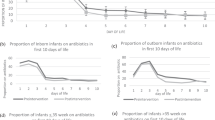
On 2/2019, the Neonatal Antimicrobial Stewardship Program at Nationwide Children’s Hospital recommended reducing empirical antibiotic therapy for early-onset sepsis (EOS) from 48 to 24 hours with a TIME-OUT. We describe our experience with this guideline and assess its safety.
Methods
Retrospective review of newborns evaluated for possible EOS at 6 NICUs from 12/2018-7/2019. Safety endpoints were re-initiation of antibiotics within 7 days after discontinuation of the initial course, positive bacterial blood or cerebrospinal fluid culture in the 7 days after antibiotic discontinuation, and overall and sepsis-related mortality.
Result
Among 414 newborns evaluated for EOS, 196 (47%) received a 24 hour rule-out sepsis antibiotic course while 218 (53%) were managed with a 48 hour course. The 24-hour rule-out group were less likely to have antibiotics re-initiated and did not differ in the other predefined safety endpoints.
Conclusion
Antibiotic therapy for suspected EOS may be discontinued safely within 24 hours.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others


Data availability
The de-identified dataset generated from the study is available from the corresponding author on reasonable request and following approval by the Institutional Review Board of Nationwide Children’s Hospital.
References
Hsieh EM, Hornik CP, Clark RH, Laughon MM, Benjamin DK Jr, Smith PB, et al. Medication use in the neonatal intensive care unit. Am J Perinatol. 2014;31:811–21.
Cotten CM, Taylor S, Stoll B, Goldberg RN, Hansen NI, Sanchez PJ, et al. Prolonged duration of initial empirical antibiotic treatment is associated with increased rates of necrotizing enterocolitis and death for extremely low birth weight infants. Pediatrics. 2009;123:58–66.
Cantey JB, Pyle AK, Wozniak PS, Hynan LS, Sanchez PJ. Early Antibiotic Exposure and Adverse Outcomes in Preterm, Very Low Birth Weight Infants. J Pediatr. 2018;203:62–7.
Alexander VN, Northrup V, Bizzarro MJ. Antibiotic exposure in the newborn intensive care unit and the risk of necrotizing enterocolitis. J Pediatr. 2011;159:392–7.
Kuppala VS, Meinzen-Derr J, Morrow AL, Schibler KR. Prolonged initial empirical antibiotic treatment is associated with adverse outcomes in premature infants. J Pediatr. 2011;159:720–5.
Novitsky A, Tuttle D, Locke RG, Saiman L, Mackley A, Paul DA. Prolonged early antibiotic use and bronchopulmonary dysplasia in very low birth weight infants. Am J Perinatol. 2015;32:43–8.
Ting JY, Synnes A, Roberts A, Deshpandey A, Dow K, Yoon EW, et al. Association Between Antibiotic Use and Neonatal Mortality and Morbidities in Very Low-Birth-Weight Infants Without Culture-Proven Sepsis or Necrotizing Enterocolitis. JAMA Pediatr. 2016;170:1181–7.
Ting JY, Synnes A, Roberts A, Deshpandey AC, Dow K, Yang J, et al. Association of Antibiotic Utilization and Neurodevelopmental Outcomes among Extremely Low Gestational Age Neonates without Proven Sepsis or Necrotizing Enterocolitis. Am J Perinatol. 2018;35:972–8.
Cantey JB, Huffman LW, Subramanian A, Marshall AS, Ballard AR, Lefevre C, et al. Antibiotic Exposure and Risk for Death or Bronchopulmonary Dysplasia in Very Low Birth Weight Infants. J Pediatr. 2017;181:289–93.e1.
de Man P, Verhoeven BA, Verbrugh HA, Vos MC, van den Anker JN. An antibiotic policy to prevent emergence of resistant bacilli. Lancet. 2000;355:973–8.
Cantey JB, Wozniak PS, Pruszynski JE, Sanchez PJ. Reducing unnecessary antibiotic use in the neonatal intensive care unit (SCOUT): a prospective interrupted time-series study. Lancet Infect Dis. 2016;16:1178–84.
Ting JY, Roberts A, Sherlock R, Ojah C, Cieslak Z, Dunn M, et al. Duration of Initial Empirical Antibiotic Therapy and Outcomes in Very Low Birth Weight Infants. Pediatrics. 2019;143:e20182286.
Mukhopadhyay S, Lieberman ES, Puopolo KM, Riley LE, Johnson LC. Effect of early-onset sepsis evaluations on in-hospital breastfeeding practices among asymptomatic term neonates. Hosp Pediatr. 2015;5:203–10.
Ong MS, Umetsu DT, Mandl KD. Consequences of antibiotics and infections in infancy: bugs, drugs, and wheezing. Ann Allergy Asthma Immunol. 2014;112:441–5 e1.
Bailey LC, Forrest CB, Zhang P, Richards TM, Livshits A, DeRusso PA. Association of antibiotics in infancy with early childhood obesity. JAMA Pediatr. 2014;168:1063–9.
Nguyen LH, Ortqvist AK, Cao Y, Simon TG, Roelstraete B, Song M, et al. Antibiotic use and the development of inflammatory bowel disease: a national case-control study in Sweden. Lancet Gastroenterol Hepatol. 2020;5:986–95.
Dash S, Syed YA, Khan MR. Understanding the Role of the Gut Microbiome in Brain Development and Its Association With Neurodevelopmental Psychiatric Disorders. Front Cell Dev Biol. 2022;10:880544.
Mohamed TH, Abdi HH, Magers J, Prusakov P, Slaughter JL. Nephrotoxic medications and associated acute kidney injury in hospitalized neonates. J Nephrol. 2022;35:1679–87.
American Academy of Pediatrics Committee on F, Newborn. Levels of neonatal care. Pediatrics. 2012;130:587–97.
Puopolo KM, Benitz WE, Zaoutis TE, Committee On F, Newborn, Committee On Infectious D. Management of Neonates Born at </=34 6/7 Weeks’ Gestation With Suspected or Proven Early-Onset Bacterial Sepsis. Pediatrics. 2018;142:e20182896.
Puopolo KM, Benitz WE, Zaoutis TE, Committee On F, Newborn, Committee On Infectious D. Management of Neonates Born at >/=35 0/7 Weeks’ Gestation With Suspected or Proven Early-Onset Bacterial Sepsis. Pediatrics. 2018;142:e20182894.
Kirn TJ, Weinstein MP. Update on blood cultures: how to obtain, process, report, and interpret. Clin Microbiol Infect. 2013;19:513–20.
Parry G, Tucker J, Tarnow-Mordi W, Group UKNSSC. CRIB II: an update of the clinical risk index for babies score. Lancet. 2003;361:1789–91.
Reyman M, van Houten MA, Watson RL, Chu M, Arp K, de Waal WJ, et al. Effects of early-life antibiotics on the developing infant gut microbiome and resistome: a randomized trial. Nat Commun. 2022;13:893.
Kuzniewicz MW, Puopolo KM. Antibiotic stewardship for early-onset sepsis. Semin Perinatol. 2020;44:151325.
Le J, Greenberg RG, Benjamin DK, Yoo Y, Zimmerman KO, Cohen-Wolkowiez M, et al. Prolonged Post-Discontinuation Antibiotic Exposure in Very Low Birth Weight Neonates at Risk for Early-Onset Sepsis. J Pediatr Infect Dis Soc. 2021;10:615–21.
Magers J, Prusakov P, Speaks S, Conroy S, Sanchez PJ. Safety and Efficacy of Nafcillin for Empiric Therapy of Late-Onset Sepsis in the NICU. Pediatrics. 2022;149:e2021052360.
Arias-Felipe A, Ramirez-Berrios J, Recio-Martinez R, Orellana-Miguel MA, Fontiveros-Escalona D, Bergon-Sendin E, et al. Determining Time to Positivity of Blood Cultures in a Neonatal Unit. J Pediatr Infect Dis Soc. 2022;11:510–3.
Acknowledgements
The authors wish to thank Alexandra K. Medoro, MD, Joshua R. Watson, MD, Gregory Ryshen, BS, MS, MBA, Melinda Albertson, NNP, Caitlyn Schwirian, PharmD, Wai-Yin Mandy Tam, PharmD, Tommy Nathaniel Johnson-Roddenberry, DNP, NNP-BC, and Maria Jebbia, MD at Nationwide Children’s Hospital for their support of the short course empirical antibiotic therapy for early-onset sepsis guidance. The study was presented virtually and in part at the Pediatric Academic Societies Meeting on 8/4/2020.
Author information
Authors and Affiliations
Consortia
Contributions
PJS conceptualized and designed the study, coordinated and supervised data collection, and drafted and revised the manuscript. PP conceptualized and designed the study, designed the data collection instruments, collected data, carried out the initial analyses, and reviewed and revised the manuscript. CdeAR collected and helped to analyze the data, reviewed and revised the manuscript, and approved the final manuscript as submitted. EZ-F collected and helped to analyze the data, reviewed and revised the manuscript, and approved the final manuscript as submitted. MCRE collected and helped to analyze the data, reviewed and revised the manuscript, and approved the final manuscript as submitted. NOW conceptualized and designed the study, reviewed and revised the manuscript. RRM conceptualized and designed the study, reviewed and revised the manuscript. RM conceptualized and designed the study, reviewed and revised the manuscript. ART conceptualized and designed the study, reviewed, and revised the manuscript. JKM conceptualized and designed the study, collected data, reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
PP received grant funding from Merck & Co. unrelated to this study. Other authors have no conflicts of interest relevant to this article to disclose.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sánchez, P.J., Prusakov, P., de Alba Romero, C. et al. Short-course empiric antibiotic therapy for possible early-onset sepsis in the NICU. J Perinatol 43, 741–745 (2023). https://doi.org/10.1038/s41372-023-01634-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-023-01634-3
This article is cited by
-
Short course antibiotic therapy: When is no difference the same?
Journal of Perinatology (2023)
