
Abstract
Early intervention is essential for favorable long-term outcomes in schizophrenia. However, there is limited guidance in the scientific literature on how best to choose between dopamine D2 receptor (D2R) partial agonists and D2R antagonists in early stages of schizophrenia. The aim of this meta-analysis was to directly compare D2R partial agonists with D2R antagonists for efficacy and tolerability, using randomized controlled trials (RCTs) that involved participants diagnosed with first-episode psychosis, schizophrenia, or related psychotic disorders with a duration of illness ≤5 years. Fourteen RCTs, involving 2494 patients, were included in the meta-analysis. Aripiprazole was the only identified D2R partial agonist, and was not significantly different from pooled D2R antagonists for overall symptom reduction or all-cause discontinuation. However, aripiprazole was more favorable than pooled D2R antagonists for depressive symptoms, prolactin levels, and triglyceride levels. Specifically, aripiprazole was more favorable than paliperidone for triglyceride levels and more favorable than risperidone and olanzapine, but less favorable than ziprasidone, for weight gain. In addition, aripiprazole was less favorable for akathisia compared with second-generation D2R antagonists, in particular olanzapine and quetiapine, and less favorable for discontinuation due to inefficacy than risperidone. Lastly, aripiprazole was more favorable than haloperidol for various efficacy and tolerability outcomes. In conclusion, aripiprazole’s efficacy did not differ substantially from D2R antagonists in the early course of schizophrenia, whereas differential tolerability profiles were noted. More double-blind RCTs are required comparing the efficacy and tolerability of aripiprazole as well as other D2R partial agonists with D2R antagonists in early stages of schizophrenia.
Similar content being viewed by others


Introduction
Schizophrenia is a debilitating psychiatric disorder that affects 0.87% of the general population over a lifetime1. The onset of schizophrenia is typically between the ages of 14 and 352, and the disease is associated with a reduction in lifespan by approximately 16.3–18.7 years compared with the general population3. Recent research shows that antipsychotic treatment is associated with a lower mortality risk compared with no treatment during follow-up periods4. This illustrates the importance of utilizing antipsychotics in patients with schizophrenia, but how these medications should be used for optimal outcomes requires further research.
First-episode psychosis (FEP) refers to the first time an individual experiences psychotic symptoms, which gives significant distress, confusion, and fear to many individuals5. There is well-established evidence that the duration of untreated psychosis is negatively associated with long-term outcomes, indicating that intervening early and effectively is important in FEP5. The literature suggests that an illness duration of less than 5 years is considered an acceptable period of time to define the early stage of schizophrenia6. Thus, a person who has FEP, or is in an early stage of schizophrenia, should be provided with evidence-based pharmacotherapy in a timely manner.
Current treatment guidelines recommend second-generation antipsychotics, including risperidone, quetiapine, olanzapine, and aripiprazole, as first-line treatment for schizophrenia7. Aripiprazole’s pharmacology is distinct from most antipsychotics in that it is a dopamine D2 receptor (D2R) partial agonist, rather than a full D2 receptor antagonist8. Owing to this difference in pharmacology, D2R partial agonists (including brexpiprazole and cariprazine) have also been referred to as third-generation antipsychotics8. To date, there is limited evidence as to how D2R partial agonists differ from D2R antagonists in the early course of schizophrenia. The most recent network meta-analysis of the efficacy and tolerability of antipsychotics in FEP included 19 randomized controlled studies (RCTs), of which only one RCT involved a D2 partial agonist, aripiprazole9.
The small number of RCTs in the literature that compared D2 partial agonists with D2 antagonists in FEP led us to conduct a systematic review that does not restrict the target population to FEP but also includes all individuals in the early course of their disease, using the evidence-based definition (i.e., a duration of illness less than 5 years)6. The objective of our study was to conduct a meta-analysis comparing the efficacy and tolerability of D2R partial agonists with D2R antagonists in the early course of schizophrenia.
Results
Study characteristics
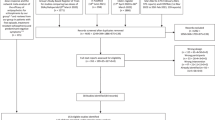
Of the 1072 records identified, 14 studies, involving a total of 2494 patients were included in our meta-analysis (Supplementary Fig. 1)10,11,12,13,14,15,16,17,18,19,20,21,22,23. Included studies are summarized in Table 1. Seven of our included studies were open-label (50%), 4 were double-blind (28.6%), and 2 were single-blind RCTs (14.3%). Blinding was unknown for one study (7.1%). In this meta-analysis, aripiprazole was the only D2R partial agonist that was identified and all studies utilized an oral form of aripiprazole. Aripiprazole (n = 1013) was compared directly with D2R antagonists (n = 1481), including risperidone (n = 421; 7 studies), olanzapine (n = 298; 4 studies), quetiapine (n = 206; 4 studies), haloperidol (n = 209; 3 studies), ziprasidone (n = 150; 3 studies), paliperidone (n = 175; 2 studies), and perospirone (n = 22; 1 study). The pooled mean age of the entire sample (one study missing; n = 2434) was 25.85 (SD = 9.19) years and male patients consisted of 60.6% of the population. The mean duration of illness was 1.78 years (n = 2302; 10 studies). Regarding the risk of bias assessment, few details were reported about allocation of concealment (14.3%), and less than half of the included studies demonstrated low risk for blinding of participants and personnel (28.6%) and blinding of outcome assessment (42.9%). Other aspects of risk of bias assessment are summarized in Supplementary Fig. 2. Four studies reported results for multiple follow-up durations11,16,18,23. For some of the included studies19,22,23, outcomes of interest were additionally found in separate publications24,25,26,27,28,29,30,31,32,33.
Aripiprazole versus pooled D2R antagonists
Results of comparing aripiprazole with D2R antagonists (as a group) are shown in Table 2. Aripiprazole was not significantly different from D2R antagonists in terms of overall symptom reduction (SMD = −0.05, 95% CI = −0.27 to 0.18; Table 2). In terms of other secondary outcomes, aripiprazole was more favorable than D2R antagonists for depressive symptoms (SMD = −0.17, 95% CI = −0.31 to −0.04), prolactin levels (SMD = −0.55, 95% CI = −0.94 to −0.16), and triglyceride levels (SMD = −0.23, 95% CI = −0.45 to −0.02) (Table 2). Removal of haloperidol trials led to aripiprazole being less favorable than D2R antagonists for akathisia (RR = 1.42, 95% CI = 1.11 to 1.81) and use of anticholinergics (RR = 1.32, 95% CI = 1.01 to 1.72).
When only blinded RCTs were considered (4 double-blind, 2 single-blind), aripiprazole remained more favorable than D2R antagonists for depressive symptoms (p = 0.03), prolactin levels (p = 0.008), and triglyceride levels (p = 0.002). In addition, aripiprazole was more favorable than D2R antagonists for total cholesterol (p < 0.001) and glucose levels (p = 0.001), and less favorable than D2R antagonists for discontinuation due to inefficacy (p = 0.02). Including only the double-blind RCTs led to aripiprazole being more favorable than D2R antagonists for prolactin (p = 0.008), triglyceride (p = 0.03), total cholesterol (p < 0.001), and glucose levels (p = 0.001), and less favorable for discontinuation due to inefficacy (p = 0.02). Restricting the analysis to open-label RCTs (N = 7 trials) led to aripiprazole being less favorable than second-generation D2R antagonists for akathisia (p = 0.02) and anticholinergic use (p < 0.001), whereas no significant difference emerged for blinded RCTs.
When studies were stratified according to trial duration, for short-term trials (<6 months), aripiprazole was significantly more favorable than D2R antagonists for depressive symptoms (SMD = −0.20, 95% CI = −0.35 to −0.04), total cholesterol levels (SMD = −0.28, 95% CI = −0.49 to −0.06), triglyceride levels (SMD = −0.27, 95% CI = −0.42 to −0.11), glucose levels (SMD = −0.22, 95% CI = −0.35 to −0.08), and prolactin levels (SMD = −0.67, 95% CI = −1.07 to −0.26), and less favorable for akathisia (RR = 1.42, 95% CI = 1.05 to 1.90). Removal of the short-term trial that used perospirone (which is only used in Japan) did not change the significance of the results. For long-term trials (≥6 months), aripiprazole was significantly more favorable than D2R antagonists for discontinuation due to adverse events (RR = 0.40, 95% CI = 0.19 to 0.83) and sedation (RR = 0.75, 95% CI = 0.57 to 0.99). When the long-term trials that used first-generation antipsychotics (i.e., haloperidol) were removed from the analysis, aripiprazole was no longer significantly more favorable than D2R antagonists for discontinuation due to adverse events.
Aripiprazole versus individual D2R antagonists
Comparisons of aripiprazole with each of the D2R antagonists that led to significant results and were based on at least two comparisons are summarized in Table 3. Aripiprazole was associated with larger reductions in overall and negative symptoms than haloperidol and in depressive symptoms than haloperidol and risperidone. Aripiprazole was more favorable for discontinuation due to any cause and adverse events than haloperidol, but less favorable for discontinuation due to inefficacy than risperidone. Aripiprazole was more favorable for metabolic adverse effects than risperidone (weight gain), paliperidone (triglyceride levels), and olanzapine (weight gain), but less favorable than ziprasidone (weight gain). Aripiprazole was less favorable for extrapyramidal side effects than quetiapine (akathisia) and olanzapine (akathisia and use of anticholinergics).
Studies comparing aripiprazole with risperidone were sufficient in number to be analyzed in short-term and long-term trials. For overall symptom reduction, aripiprazole did not significantly differ from risperidone in short-term trials (N = 7 trials, n = 732, SMD = 0.13, 95% CI = −0.13 to 0.39, p = 0.34), but demonstrated significantly greater efficacy than risperidone in long-term trials (N = 3 trials, n = 198; SMD = −0.74, 95% CI = −1.25 to −0.24, p = 0.004), and a significant difference was found between the two durations (χ2 = 6.44, p = 0.01). For positive symptom reduction, aripiprazole was significantly less efficacious than risperidone in short-term trials (N = 4 trials, n = 444; SMD = 0.25, 95% CI = 0.06 to 0.44, p = 0.009), but was not significantly different in long-term trials (N = 2 trials, n = 158; SMD = −0.40, 95% CI = −0.82 to 0.02, p = 0.06), and no significant subgroup difference was found between short-term and long-term trials. For negative symptom reduction, no significant difference between aripiprazole and risperidone was found in neither short-term nor long-term trials, and no subgroup difference between the two durations was noted. For all-cause discontinuation and discontinuation due to adverse events, no significant difference between aripiprazole and risperidone was found in neither short-term nor long-term trials, and no subgroup difference between the two durations was noted. For discontinuation due to inefficacy, aripiprazole was significantly less favorable than risperidone in short-term trials (N = 2 trials, n = 410; RR = 1.77, 95% CI = 1.13 to 2.76, p = 0.01), but was not significantly different in long-term trials (N = 2, n = 482; RR = 1.66, 95% CI = 0.85 to 3.24, p = 0.14), and no subgroup difference between the two durations was noted.
Heterogeneity
Heterogeneity (I2 > 50%) was present for overall symptom reduction, positive symptom reduction, discontinuation due to adverse events and inefficacy, use of anticholinergics, incidence of akathisia, weight gain, total cholesterol levels, triglyceride levels, fasting glucose levels, prolactin levels, and incidence of sedation (Table 2). The short-term study (i.e., 8 weeks) that compared aripiprazole with risperidone and olanzapine22 and the long-term study (i.e., 3 years) that compared aripiprazole with risperidone, quetiapine, olanzapine, ziprasidone, and haloperidol23 were each source of heterogeneity for positive symptom reduction, and removal of each study did not change the significance of the result. The long-term study (i.e., 3 years) that compared aripiprazole with quetiapine and ziprasidone29 was the source of heterogeneity for triglyceride levels, and removal of the study did not change the significance of the result. The long-term study (i.e., 1 year) that compared aripiprazole with paliperidone and ziprasidone11 was the source of heterogeneity for glucose levels, and removal of the study led to aripiprazole being significantly more favorable than D2R antagonists (SMD = −0.21, 95% CI = −0.34 to −0.07). The long-term study (i.e., 1 year) that compared aripiprazole with haloperidol10 was the source of heterogeneity for incidence of akathisia, and removal of the study led to aripiprazole being significantly less favorable than D2R antagonists (RR = 1.39, 95% CI = 1.08 to 1.80). The long-term study (i.e., 3 years) that compared aripiprazole with risperidone, quetiapine, olanzapine, ziprasidone, and haloperidol23 and the long-term study (i.e., 1 year) that compared aripiprazole with risperidone and olanzapine33 were each source of heterogeneity for discontinuation due to inefficacy, and removal of the former study led to aripiprazole being less favorable than D2R antagonists (RR = 2.25, 95% CI = 1.24 to 4.09). The short-term study (i.e., 12 weeks) that compared aripiprazole with quetiapine19 and the long-term study (i.e., 3 years) that compared aripiprazole with risperidone, quetiapine, olanzapine, ziprasidone, and haloperidol23 were each source of heterogeneity for incidence of sedation, and removal of each study did not change the significance of the result. No single study was the source of heterogeneity for overall symptom reduction, discontinuation due to adverse events, use of anticholinergics, weight gain, total cholesterol levels, and prolactin levels.
Meta-regression
In our meta-regression analysis, associations of covariates with overall symptom reduction (n = 14 studies) and all-cause discontinuation (n = 11 studies) were examined (Supplementary Table 1). Aripiprazole’s effect on overall symptom reduction relative to D2R antagonists was positively associated with trial duration (estimate = −0.01, p = 0.020) and baseline symptom severity (estimate = −0.02, p = 0.041). None of the covariates demonstrated significant associations with all-cause discontinuation.
Publication bias
We assessed publication bias for overall symptom reduction (n = 14 studies) and all-cause discontinuation (n = 11 studies) (Supplementary Fig. 3). Egger’s test did not indicate substantial asymmetry in the funnel plots for both outcomes (p = 0.546 for overall symptom reduction and p = 0.917 for all-cause discontinuation).
Discussion
Our meta-analysis directly compared aripiprazole with D2R antagonists for efficacy and tolerability in the early course of schizophrenia. Aripiprazole was the only identified D2R partial agonist and was compared with various D2R antagonists, including risperidone, paliperidone, quetiapine, olanzapine, ziprasidone, perospirone, and haloperidol. Our results indicate that aripiprazole’s efficacy was comparable to D2R antagonists (as a group), however; it was more favorable in terms of depressive symptoms, triglyceride levels, and prolactin levels. When stratified according to trial duration, aripiprazole was additionally more favorable for total cholesterol levels (short-term), glucose levels (short-term), and sedation (long-term), but was less favorable for akathisia (short-term). These results are largely consistent with existing evidence that aripiprazole has antidepressant effects and a lower tendency to cause hyperprolactinemia, metabolic dysregulation, and sedation34,35,36,37,38.
Several mechanisms of action that are unique to aripiprazole may explain such results. Aripiprazole’s D2 partial agonistic properties have prolactin-sparing effects34,35. Its partial agonistic activity at postsynaptic 5-HT1A and 5-HT2C receptors, coupled with desensitization of presynaptic 5-HT1A receptors, would lead to an increased serotonergic tone, which may play a role in improving depressive and anxiety disorders38,39. Aripiprazole’s relatively lower affinity for H1 receptors compared with other second-generation antipsychotics may explain its lower propensity to induce sedation35,36. Aripiprazole’s lack of anticholinergic effects, relatively modest antagonism of H1 receptors, and partial agonistic activity at D2 and 5-HT1A receptors would explain its favorable metabolic profiles compared with other second-generation antipsychotics, apart from ziprasidone37. These results are consistent with existing evidence that both aripiprazole and ziprasidone, have favorable metabolic profiles relative to many other antipsychotics37.
It should be noted that aripiprazole (in short-term trials) was more frequently associated with akathisia compared with D2 antagonists, especially quetiapine and olanzapine. This is consistent with a recent network meta-analysis involving patients with FEP, where aripiprazole was less favorable than quetiapine and olanzapine for akathisia9. Nevertheless, aripiprazole was not associated with higher discontinuation due to adverse events than D2R antagonists, including quetiapine and olanzapine, indicating that the severity of akathisia may have been tolerable. Aripiprazole-induced akathisia may be attributed to its pro-serotonergic effects as well as its functional selectivity for D2 receptors. In the case of the latter, aripiprazole may be acting as a full antagonist in certain brain regions (e.g., striatum) where there are higher levels of D2 receptor expression35,40.
Differential results were found compared with a recent network meta-analysis involving patients with multi-episode, chronic schizophrenia41. We found that compared with haloperidol, aripiprazole was more favorable in terms of overall, negative, and depressive symptoms and discontinuation due to any cause and adverse events. This is consistent with a recent network meta-analysis involving patients with FEP that found haloperidol to be less efficacious than second-generation antipsychotics9. However, aripiprazole’s efficacy was not significantly different from haloperidol’s in patients with multi-episode, chronic schizophrenia41. Also, we found that aripiprazole was less favorable than risperidone in terms of discontinuation due to inefficacy, which is consistent with the finding in patients with multi-episode, chronic schizophrenia where risperidone was more efficacious than aripiprazole41.
Such differential results between FEP and multi-episode, chronic schizophrenia may be explained by dopamine supersensitivity, which is a key predictor of poor long-term outcomes in schizophrenia42. Individuals with multi-episode, chronic schizophrenia are likely to be exposed to chronic D2 receptor blockade, increasing the propensity to develop dopamine supersensitivity42. Since dopamine supersensitivity is associated with upregulation of D2 receptors, D2R antagonists with high affinities for the D2 receptor may be more effective than antipsychotics with lower affinities to treat the related psychosis, with the exception of clozapine that has a lower affinity but has the potential to reverse dopamine supersensitivity43. Although aripiprazole has a very high affinity for the D2 receptor (0.34 nM), its action as a partial agonist would predict worsening of psychosis in an environment of dopamine supersensitivity. This is consistent with reports showing that switching patients with chronic schizophrenia to aripiprazole can be less effective or even lead to psychotic worsening44.
However, it should be noted that aripiprazole has been shown to prevent and reverse dopamine supersensitivity and thus may be more effective over the long term45. In support of this, our sensitivity analysis found that aripiprazole, although less favorable than risperidone for discontinuation due to inefficacy over a short term, was more efficacious than risperidone over a longer term. Although more studies are required to replicate this finding, the data from animal studies and our preliminary analysis may provide a rationale for using aripiprazole prior to D2R antagonists in the treatment of FEP.
Our meta-analysis has several limitations to be considered. First, the number of studies included in our meta-analysis was relatively small. Second, many of the included studies were open-label RCTs, which could have increased the risk of performance and detection bias. Third, aripiprazole was the only identified dopamine D2R partial agonist. Due to differences in pharmacological activity even among dopamine D2R partial agonists (aripiprazole, brexpiprazole, and cariprazine), there needs to be caution when extrapolating the results of our meta-analysis to D2R partial agonists other than aripiprazole. Fourth, heterogeneity was present in various outcomes in our meta-analysis. This was expected as D2R antagonists have unique receptor profiles and thus may have varying efficacy and tolerability profiles. However, we identified sources of heterogeneity for the majority of the outcomes and addressed this limitation via subgroup, sensitivity, and meta-regression analyses. Lastly, although multiple outcomes were examined in our review, multiple comparisons were not adjusted for. This may have increased the risk of type 1 error. However, given the relatively small number of studies for each outcome, such a statistical adjustment may be more appropriate when more studies become available in the future.
In conclusion, aripiprazole’s efficacy did not differ substantially from D2R antagonists in the early course of schizophrenia, whereas it demonstrated greater antidepressant effects than D2R antagonists. Differential tolerability profiles were noted between aripiprazole and D2R antagonists, where aripiprazole appeared to have general advantages regarding prolactin and triglyceride levels over D2R antagonists, but may induce more akathisia. Evidence is still limited to draw strong conclusions. More double-blind RCTs are required to better understand the relative effects of aripiprazole and other D2R partial agonists in the early course of schizophrenia.
Methods
Search strategy
The systematic review and meta-analysis were conducted according to the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 200946. Pre-registration with the International Prospective Register of Systematic Reviews was not undertaken for our review, but we ensured that no duplicate review is ongoing to date. We searched for RCTs comparing D2R partial agonists with D2R antagonists in the early course of schizophrenia that were published up to, and including 15 July 2020, using the MEDLINE, EMBASE, and PsycINFO, and ClinicalTrials.gov databases. The following search terms and associated MeSH terms were used: (1) [‘aripiprazole’ OR ‘brexpiprazole’ OR ‘cariprazine’] AND (2) [(‘first episode’ OR ‘first-episode’ OR ‘$naive’ OR ‘early*’ OR ‘recent*’ OR ‘prodrom*’ OR ‘youth*’ OR ‘adolescen*’ OR ‘child*’) AND (‘schizophreni*’ OR ‘schizophrenia spectrum’ OR ‘psychosis’)] AND (3) [(‘random*’) OR ((‘random*’) AND (‘comparative’ OR ‘comparison*’ OR ‘compare*’ OR ‘versus’ OR ‘vs*’ OR ‘open*’)) OR (‘$blind*’)]. We also manually searched the reference lists of all relevant retrieved articles for potential studies eligible for inclusion in our analysis. Two authors (D.D.K. and L.L.) independently screened for relevant articles and any discrepancy was resolved following a discussion between the two authors or with R.M.P. Corresponding authors of the included studies were contacted for any missing data.
Selection criteria
Studies were included in the quantitative analysis if they enrolled patients who met the diagnostic criteria for schizophrenia or schizophrenia-spectrum disorders and were in their first episode (as identified by authors) or were in the early course of their illness. We defined early stages of illness as follows: (1) FEP, 2) antipsychotic-naïve, and (3) ≤5 years of mean duration of illness6. We placed no restriction on language, blinding, publication year, age, sex, ethnicity, settings, or trial duration.
Data extraction
The following data were extracted: publication year, sample size, age, sex, duration of illness, trial duration, doses of antipsychotics used, baseline symptom severity, change/endpoint scores for overall, positive, negative, and depressive symptoms, incidence of akathisia, sedation, discontinuation due to any cause, adverse events, and inefficacy, use of medications to treat extrapyramidal symptoms (EPS) (i.e., anticholinergics), and changes in body mass index and levels of prolactin, total cholesterol, triglycerides, and fasting glucose.
Mean antipsychotic doses were converted to chlorpromazine equivalents according to methods provided elsewhere47,48. Change scores measured using the Positive and Negative Syndrome Scale (PANSS) were the primary efficacy outcome49. Other validated scales were considered if the PANSS was not available. If change scores were not available, authors were contacted for the data. Endpoint scores were used if authors did not respond to our request. D.D.K. and L.L. reviewed included studies and supplementary materials, extracted relevant data, and assessed risk of bias using the Cochrane Risk of Bias tool50.
Data analysis
The meta-analysis was performed using Cochrane Review Manager (version 5.4). Using random-effects models, aripiprazole was compared with D2R antagonists (as a group) and also with individual D2R antagonists. Standardized mean differences (SMDs) and risk ratios (RRs) were calculated for continuous and dichotomous variables, respectively, with 95% confidence intervals (CIs). SMDs less than 0 and RRs less than 1 indicated that aripiprazole was favored compared with D2R antagonists. An inverse variance method was used according to the Cochrane guideline when dichotomous and continuous variables needed to be combined. When necessary, online tools were used to calculate an effect size from F or t statistics or to combine multiple means and standard deviations51. Study heterogeneity was quantified using the I2 statistic, where I2 > 50% was considered substantial heterogeneity. If a study provided data for multiple timepoints, our main analysis included the study’s planned duration. A secondary analysis was performed using the short-term (i.e., <6 months) and long-term (i.e., ≥6 months) data separately.
For outcomes that involved at least 10 studies, meta-regression analysis was performed and publication bias was assessed using R52. For the meta-regression analysis, we examined the effects of the following covariates: sample size, study year, age, trial duration, aripiprazole dose, baseline symptom severity, proportion of open-label studies, male participants, studies that included FEP patients, and studies that utilized risperidone or olanzapine. The rationale for including the proportion of risperidone or olanzapine as a covariate was based on a recent meta-analysis that has shown that risperidone and olanzapine tend to be more efficacious than other antipsychotics in multi-episode, chronic schizophrenia41. Baseline symptom scores measured on scales other than the PANSS were standardized using methods provided elsewhere53. Publication bias was assessed using funnel plots, Egger’s regression test, and trim-and-fill procedure54.
Data availability
The manuscript reports meta-analytic data based on original studies. Extracted data are available upon request.
References
Perälä, J. et al. Lifetime prevalence of psychotic and bipolar I disorders in a general population. Arch. Gen. Psychiatry 64, 19–28 (2007).
Kessler, R. C. et al. Age of onset of mental disorders: a review of recent literature. Curr. Opin. Psychiatry 20, 359–364 (2007).
Laursen, T. M. Life expectancy among persons with schizophrenia or bipolar affective disorder. Schizophr. Res. 131, 101–104 (2011).
Vermeulen, J. et al. Antipsychotic medication and long-term mortality risk in patients with schizophrenia; a systematic review and meta-analysis. Psychol. Med. 47, 2217–2228 (2017).
McGlashan, T. H. Duration of untreated psychosis in first-episode schizophrenia: marker or determinant of course? Biol. Psychiatry 46, 899–907 (1999).
Newton, R. et al. Diverse definitions of the early course of schizophrenia-a targeted literature review. NPJ Schizophr. 4, 21 (2018).
Remington, G. et al. Guidelines for the pharmacotherapy of schizophrenia in adults. Can. J. Psychiatry 62, 604–616 (2017).
Procyshyn, R.M., Bezchlibnyk-Butler, K.Z. & Jeffries, J.J. (eds). Clinical Handbook of Psychotropic Drugs 23rd edn (Hogrefe Publishing, 2019).
Zhu, Y. et al. Antipsychotic drugs for the acute treatment of patients with a first episode of schizophrenia: a systematic review with pairwise and network meta-analyses. Lancet Psychiatry 4, 694–705 (2017).
Girgis, R. R. et al. Aripiprazole versus haloperidol treatment in early-stage schizophrenia. J. Psychiatr. Res. 45, 756–762 (2011).
Zhang, Y. & Dai, G. Efficacy and metabolic influence of paliperidone ER, aripiprazole and ziprasidone to patients with first-episode schizophrenia through 52 weeks follow-up in China. Hum. Psychopharmacol. 27, 605–614 (2012).
Maat, A. et al. Open, randomized trial of the effects of aripiprazole versus risperidone on social cognition in schizophrenia. Eur. Neuropsychopharmacol. 24, 575–584 (2014).
Zhang, S. & Lan, G. Prospective 8-week trial on the effect of olanzapine, quetiapine, and aripiprazole on blood glucose and lipids among individuals with first-onset schizophrenia. Shanghai Arch. Psychiatry 26, 339–346 (2014).
Kuzmanovic, A. et al. Aripiprazole in treatment of first episode schizophrenia. Eur. Neuropsychopharmacol. 25, S498–S499 (2015).
Robinson, D. G. et al. A randomized comparison of aripiprazole and risperidone for the acute treatment of first-episode schizophrenia and related disorders: 3-month outcomes. Schizophr. Bull. 41, 1227–1236 (2015).
Savitz, A. J., Lane, R., Nuamah, I., Gopal, S. & Hough, D. Efficacy and safety of paliperidone extended release in adolescents with schizophrenia: a randomized, double-blind study. J. Am. Acad. Child Adolesc. Psychiatry 54, 126–137 (2015). e1.
Takekita, Y. et al. Antagonist and partial agonist at the dopamine D2 receptors in drug-naïve and non-drug-naïve schizophrenia: a randomized, controlled trial. Eur. Arch. Psychiatry Clin. Neurosci. 265, 579–588 (2015).
Nussbaum, L. et al. Pharmacological and clinical aspects of efficacy, safety and tolerability of atypical antipsychotic medication in child and adolescent patients with schizophrenia and bipolar disorders. Farmacia 64, 868–875 (2016).
Pagsberg, A. K. et al. Quetiapine extended release versus aripiprazole in children and adolescents with first-episode psychosis: the multicentre, double-blind, randomised tolerability and efficacy of antipsychotics (TEA) trial. Lancet Psychiatry 4, 605–618 (2017).
Wang, C. et al. The efficacy, acceptability, and safety of five atypical antipsychotics in patients with first-episode drug-naïve schizophrenia: a randomized comparative trial. Ann. Gen. Psychiatry 16, 47 (2017).
Liemburg, E. J., Sibeijn-Kuiper, A., Knegtering, H. & Aleman, A. The effect of aripiprazole versus risperidone on prefrontal brain metabolite levels and brain volume in psychotic disorders: an exploratory study. Neuropsychiatry (Lond.) 8, 176–185 (2018).
Cheng, Z. et al. An open-label randomised comparison of aripiprazole, olanzapine and risperidone for the acute treatment of first-episode schizophrenia: eight-week outcomes. J. Psychopharmacol. 33, 1227–1236 (2019).
Gómez-Revuelta, M. et al. Antipsychotic treatment effectiveness in first episode of psychosis: PAFIP 3-year follow-up randomized clinical trials comparing haloperidol, olanzapine, risperidone, aripiprazole, quetiapine, and ziprasidone. Int. J. Neuropsychopharmacol. 23, 217–229 (2020).
Juncal-Ruiz, M. et al. Comparison of the anti-inflammatory effect of aripiprazole and risperidone in 75 drug-naïve first episode psychosis individuals: a 3 months randomized study. Schizophr. Res. 202, 226–233 (2018).
Juncal-Ruiz, M. et al. Incidence and risk factors of acute akathisia in 493 individuals with first episode non-affective psychosis: a 6-week randomised study of antipsychotic treatment. Psychopharmacology (Berl.) 234, 2563–2570 (2017).
Pérez-Iglesias, R. et al. Comparison of metabolic effects of aripiprazole, quetiapine and ziprasidone after 12 weeks of treatment in first treated episode of psychosis. Schizophr. Res. 159, 90–94 (2014).
Crespo-Facorro, B. et al. Effects of aripiprazole, quetiapine and ziprasidone on plasma prolactin levels in individuals with first episode nonaffective psychosis: analysis of a randomized open-label 1year study. Schizophr. Res. 189, 134–141 (2017).
Crespo-Facorro, B. et al. Treatment of first-episode non-affective psychosis: a randomized comparison of aripiprazole, quetiapine and ziprasidone over 1 year. Psychopharmacology (Berl.) 231, 357–366 (2014).
Crespo-Facorro, B. et al. Aripiprazole, Ziprasidone and Quetiapine in the treatment of first-episode nonaffective psychosis: a 12-week randomized, flexible-dose, open-label trial. Schizophr. Res. 147, 375–382 (2013).
Vázquez-Bourgon, J. et al. A 3-year prospective study on the metabolic effect of aripiprazole, quetiapine and ziprasidone: a pragmatic clinical trial in first episode psychosis patients. Eur. Neuropsychopharmacol. 39, 46–55 (2020).
Jensen, K. G. et al. Cardiometabolic adverse effects and its predictors in children and adolescents with first-episode psychosis during treatment with quetiapine-extended release versus aripiprazole: 12-week results from the tolerance and effect of antipsychotics in children and adolescents with psychosis (TEA) Trial. J. Am. Acad. Child Adolesc. Psychiatry 58, 1062–1078 (2019).
Wang, J. et al. Cognitive effects of atypical antipsychotic drugs in first-episode drug-naïve schizophrenic patients. Neural Regen. Res. 8, 277–286 (2013).
Hou, Y. et al. Neurocognitive effects of atypical antipsychotics in patients with first-episode schizophrenia. Nord. J. Psychiatry 1–8 (2020).
Keks, N. et al. Comparative tolerability of dopamine D2/3 receptor partial agonists for schizophrenia. CNS Drugs 34, 473–507 (2020).
Shapiro, D. A. et al. Aripiprazole, a novel atypical antipsychotic drug with a unique and robust pharmacology. Neuropsychopharmacology 28, 1400–1411 (2003).
Correll, C. U. & Gallego, J. A. Antipsychotic polypharmacy: a comprehensive evaluation of relevant correlates of a long-standing clinical practice. Psychiatr. Clin. North Am. 35, 661–681 (2012).
Nasrallah, H. A. Atypical antipsychotic-induced metabolic side effects: insights from receptor-binding profiles. Mol. Psychiatry 13, 27–35 (2008).
Pae, C. U., Serretti, A., Patkar, A. A. & Masand, P. S. Aripiprazole in the treatment of depressive and anxiety disorders: a review of current evidence. CNS Drugs 22, 367–388 (2008).
Kim, D. D. et al. Clozapine-associated obsessive-compulsive symptoms and their management: a systematic review and analysis of 107 reported cases. Psychother. Psychosom. 89, 151–160 (2020).
Guo, M. Y. et al. Association of antidepressant use with drug-related extrapyramidal symptoms: a pharmacoepidemiological study. J. Clin. Psychopharmacol. 38, 349–356 (2018).
Huhn, M. et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. Lancet 394, 939–951 (2019).
Yin, J., Barr, A. M., Ramos-Miguel, A. & Procyshyn, R. M. Antipsychotic induced dopamine supersensitivity psychosis: a comprehensive review. Curr. Neuropharmacol. 15, 174–183 (2017).
Kim, D. D., Barr, A. M., Honer, W. G. & Procyshyn, R. M. Reversal of dopamine supersensitivity as a mechanism of action of clozapine. Psychother. Psychosom. 87, 306–307 (2018).
Takeuchi, H. & Remington, G. A systematic review of reported cases involving psychotic symptoms worsened by aripiprazole in schizophrenia or schizoaffective disorder. Psychopharmacology (Berl.) 228, 175–185 (2013).
Tadokoro, S. et al. Chronic treatment with aripiprazole prevents development of dopamine supersensitivity and potentially supersensitivity psychosis. Schizophr. Bull. 38, 1012–1020 (2012).
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G., PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6, e1000097 (2009).
Inada, T. & Inagaki, A. Psychotropic dose equivalence in Japan. Psychiatry Clin. Neurosci. 69, 440–447 (2015).
Leucht, S. et al. Dose equivalents for second-generation antipsychotics: the minimum effective dose method. Schizophr. Bull. 40, 314–326 (2014).
Kay, S. R., Fiszbein, A. & Opler, L. A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 13, 261–276 (1987).
Higgins, J. P. T. et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.1 (updated September 2020). Cochrane, 2020. Available from www.training.cochrane.org/handbook.
Wilson, D. B. Practical Meta-Analysis Effect Size Calculator. George Mason University. http://www.campbellcollaboration.org/escalc/html/EffectSizeCalculator-Home.php. Accessed 14 July 2019.
Balduzzi, S., Rücker, G. & Schwarzer, G. How to perform a meta-analysis with R: a practical tutorial. Evid. Based Ment. Health 22, 153–160 (2019).
Leucht, S., Rothe, P., Davis, J. M. & Engel, R. R. Equipercentile linking of the BPRS and the PANSS. Eur. Neuropsychopharmacol. 23, 956–959 (2013).
Sterne, J. A., Egger, M. & Smith, G. D. Systematic reviews in health care: Investigating and dealing with publication and other biases in meta-analysis. BMJ 323, 101–105 (2001).
Author information
Authors and Affiliations
Contributions
D.D.K. and R.M.P. conceived the idea and designed the study. D.D.K. conducted the systematic review and meta-analysis, and drafted the manuscript. R.M.P. and A.M.B. supervised the study. L.L. assisted with study selection and data extraction. A.M.B., J.W.Y.Y., D.F., W.G.H., and A.E.T. contributed to the interpretation of data and critically reviewed the content of the manuscript for important intellectual content. All authors revised and edited the paper and approved the completed version.
Corresponding author
Ethics declarations
Competing interests
A.M.B. has no potential conflicts. W.G.H. has received consulting fees or sat on paid advisory boards for the AlphaSights, Guidepoint, In Silico (unpaid), Newron, Translational Life Sciences and Otsuka/Lundbeck, and is a shareholder in Eli Lilly and Translational Life Sciences. R.M.P. has received consulting fees or sat on paid advisory boards for Janssen, Lundbeck and Otsuka; is on the speaker’s bureau for Janssen, Lundbeck and Otsuka. D.D.K., L.L., J.W.Y.Y., D.F. have no conflict of interest to declare.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kim, D.D., Barr, A.M., Lian, L. et al. Efficacy and tolerability of aripiprazole versus D2 antagonists in the early course of schizophrenia: a systematic review and meta-analysis. npj Schizophr 7, 29 (2021). https://doi.org/10.1038/s41537-021-00158-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41537-021-00158-z
This article is cited by
-
Antipsychotic drug—aripiprazole against schizophrenia, its therapeutic and metabolic effects associated with gene polymorphisms
Pharmacological Reports (2023)
-
Consumption of psychotropic drugs in Croatia before and during the COVID-19 pandemic: a 10-year longitudinal study (2012–2021)
Social Psychiatry and Psychiatric Epidemiology (2023)
-
Place of the partial dopamine receptor agonist aripiprazole in the management of schizophrenia in adults: a Delphi consensus study
BMC Psychiatry (2022)
-
Network Analysis of the Structure of the Core Symptoms and Clinical Correlates in Comorbid Schizophrenia and Gambling Disorder
International Journal of Mental Health and Addiction (2022)
