
Abstract
The main objective of the present study was to investigate the association between several epigenetic clocks, covering different aspects of aging, with schizophrenia relapse evaluated over a 3-year follow-up period in a cohort of ninety-one first-episode schizophrenia patients. Genome-wide DNA methylation was profiled and four epigenetic clocks, including epigenetic clocks of chronological age, mortality and telomere length were calculated. Patients that relapsed during the follow-up showed epigenetic acceleration of the telomere length clock (p = 0.030). Shorter telomere length was associated with cognitive performance (working memory, r = 0.31 p = 0.015; verbal fluency, r = 0.28 p = 0.028), but no direct effect of cognitive function or symptom severity on relapse was detected. The results of the present study suggest that epigenetic age acceleration could be involved in the clinical course of schizophrenia and could be a useful marker of relapse when measured in remission stages.
Similar content being viewed by others


Introduction
Schizophrenia has been associated with reduced life expectancy due to an increased suicide rate, poor health habits, and limited access to medical care, but especially due to chronic related pathologies1,2,3,4. Schizophrenia patients exhibit higher expression of age-related peripheral biomarkers of inflammation, oxidative stress and metabolic health5. The accelerated aging hypothesis of schizophrenia has been proposed to explain these observations, arguing that schizophrenia risk factors, either endogenous (i.e., genetic factors) or environmental (i.e., early life stressors), could accelerate the progressive biological changes of normal aging5,6.
According to recent research, aging can be defined in different ways and has several hallmarks that may play an integral role in the biological process of accelerated aging7. Several biomarkers of aging have been proposed in schizophrenia with contradictory outcomes, leading to the idea that schizophrenia may be associated with segmental aging, that is, some but not all features of aging may be accelerated6.
DNA methylation-based epigenetic clocks8,9 are validated predictors of chronological age across all tissues and across the entire lifespan. Increased or decreased epigenetic age relative to chronological age is termed as acceleration or deceleration. Age acceleration predicts an increased risk of age-related diseases10 and all-cause mortality11. Although aberrant DNA methylation has been consistently reported in schizophrenia12, no significant accelerated aging has been observed13,14,15,16,17,18. In fact, the largest study performed to date in whole blood and brain tissues identified a reduced age acceleration in patients who have schizophrenia, which contradicts the accelerated aging hypothesis of schizophrenia19. However, in recent years, numerous epigenetic clocks have been developed that appear to capture distinct aspects of aging, other than the classical prediction of chronological age, such as age-related morbidity and mortality20 or telomere length21. A recent large-scale DNA methylation study that simultaneously tested 14 epigenetic clocks covering different aspects of aging found that non-classical predictors of epigenetic aging (i.e., mortality telomere length clocks) were altered in schizophrenia cases22. Overall these results are consistent with the notion of segmental aging in schizophrenia. However, little is known about the effect that accelerated epigenetic age has on the clinical course of the disease.
The main objective of the present study was to investigate the association between several epigenetic clocks, covering different aspects of aging, with schizophrenia relapse evaluated over a 3-year follow-up period in a cohort of first-episode schizophrenia patients with less than 5 years of evolution. We hypothesized that relapse would be associated with accelerated aging, observable in clinical remission stages after a first episode of schizophrenia.
Results
Sample description
Table 1 shows the sociodemographic and clinical characteristics of the 91 participants at study entry, classified as non-relapse (those patients that had not experienced relapse after 3 years of enrollment) (N = 49) or relapse (those patients that relapsed during the 3-year follow-up) (N = 42). At study entry, relapsed patients were, on average, in the first year after the diagnosis of their first episode (0.90 ± 1.06), whereas non-relapsed patients had experienced their first episode one year and a half before (1.67 ± 1.44) (t89 = 2.82, p = 0.006).
Epigenetic clocks in relapse
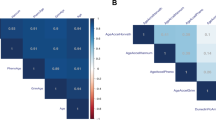
In our cohort, the measured epigenetic clocks of chronological age (Horvath and Hannun clocks), mortality (PhenoAge) and telomere length (DNAmTL) were highly correlated with each other and with the chronological age (Fig. 1A). As might be expected, because telomere length decreases with age, a negative correlation between the DNAmTL clock and the other computed clocks and chronological age was observed.

A Correlation coefficient between the measured epigenetic clocks of chronological age (Horvath and Hannun clocks), mortality (PhenoAge) and telomere length (DNAmTL) and chronological age. (***p < 0.001). B Average IEAA of the measured epigenetic clocks of chronological age (Horvath and Hannun clocks), mortality (PhenoAge) and telomere length (DNAmTL) between patients that relapse (R) and those that do not relapse (NR).
Several factors may have an impact on DNA methylation, such as gender, socio-economic status, toxic habits (including tobacco, cannabis and alcohol), antipsychotic dose and time since first episode. In our cohort, none of these showed a significant association with the two measures of age acceleration in any epigenetic clock, except for the PhenoAge IEAA, which showed significant differences among genders (males −0.29 ± 4.62 vs. females 0.97 ± 5.13, t89 = 2.22 p = 0.029) (Supplementary Table 1).
We failed to find any acceleration or deceleration of the epigenetic clocks between relapsed and non-relapsed patients when we used the IEAA (Fig. 1B). However, when we adjusted for cell composition using the EEAA (Fig. 2), significant differences in acceleration of telomere length between non-relapsed patients (0.02 ± 0.11 base pairs) and relapsed patients (−0.03 ± 0.09 base pairs) were observed (t89 = 2.21, p = 0.030) (Fig. 2A). As mentioned previously, telomere length decreases with age, and for this reason we considered telomere length and DNAmTL to be accelerated in relapse (Fig. 2B). In order to explore the discrepancy between IEAA and EAA results we assessed the correlation between cell composition and epigenetic acceleration of the DNAmTL clock. IEAA showed significant positive correlation with CD4T (r = 0.40, p < 0.001), whereas as expected, EEAA showed no significant correlation with cell composition as it accounted for these differences.

Average EEAA of the epigenetic clocks (mean ± SD) (A) and chronological age compared to DNAm Age or telomere length (B) between patients that relapse (R) and those that do not relapse (NR).
Epigenetic clocks and clinical data
As a secondary analysis we analyzed the partial correlations adjusting for gender, socio-economic status, toxic habits (tobacco, cannabis and alcohol), antipsychotic dose and time since first episode, has been performed to assess the correlations between the epigenetic age acceleration measures and symptom severity according to the standard Marder PANSS factors, the seven cognitive domains identified in the PCA analysis and the cognitive reserve. Only the EEAA of the DNAmTL clock showed significant correlations with working memory (r = 0.31 p = 0.015) and verbal fluency (r = 0.28 p = 0.028) (Supplementary Table 2).
Working memory and verbal fluency were considered for the mediation analysis, as they were significantly associated with the EEAA of the DNAmTL clock. However, mediation analyses did not provide evidence of a significant indirect effect of these mediator variables on relapse (Table 2).
Discussion
To establish a relationship between epigenetic clocks and relapse after the remission of a first episode of psychosis we measured several epigenetic clocks to capture the complex and multifaceted process of aging8,9,20,21 in a cohort of patients with less than 5 years of evolution that were evaluated over a 3-year follow-up period. Patients that relapsed during the follow-up showed epigenetic acceleration of the telomere length clock, this is shorter telomeres than patients who had not relapsed. The significant results for the epigenetic estimator of telomere length, but not the other epigenetic clocks that predict chronological age or mortality, were consistent with the segmental aging hypothesis for schizophrenia, since not all features of accelerated aging are evident in these patients6,22.
The results of the present study suggest that epigenetic age acceleration could be involved in the clinical course of schizophrenia and could be a useful marker of relapse when measured in remission stages. This is consistent with a recent study that examined epigenetic clocks of chronological age and symptom severity in a schizophrenia sample23. The authors found a significant positive correlation between the EEAA measure and the SCL-90 psychotic score, with those patients with the worst scores having higher acceleration23. It is also consistent with previous studies that also showed associations between the EEAA and clinical symptoms and the course of the disease in other neuropsychiatric diseases such as posttraumatic stress disorder24,25.
Extrinsic epigenetic age acceleration measures capture both cell intrinsic methylation changes and extracelular changes in blood cell composition26. Therefore, by construction, reflects aspects of immunosenescence, as it captures age-related changes in blood cell composition, such as T lymphocyte populations, which underlie much of the age-related decline in the protective immune response27. Thus, the predictive significance of EEAA of the DNAmTL clock for relapse instead of IEAA probably reflects the fact that it assesses multiple aspects of the biological age of the immune system. Our results agreed with multiple evidences of dysregulation of the adaptive immunity cells in schizophrenia28. Moreover, a recent study identified a subtype of schizophrenia, using multi-omic measures, which exhibited widespread methylation level alterations among genes enriched in immune cell activity, as well as a higher proportion of neutrophils and lower proportion of lymphocytes29. This subtype had higher symptom severity and performed worse on cognitive measures, both factors that could be related to higher relapse rates.
Telomere length in leukocytes is one of the most studied hallmarks of aging in schizophrenia, having been used to demonstrate the accelerated aging hypothesis of this disease. Different studies have shown an association between telomere shortening and schizophrenia30,31,32,33,34,35,36,37,38,39, including a meta-analysis of case-control studies40,41,42. However, the evidence is inconclusive, with studies reporting no differences43,44,45,46,47,48,49,50 or even a longer telomere length in schizophrenia51,52.
Several studies have explored the role of telomere length in the course of the disease. Although different outcomes have been evaluated, our results are consistent with those that showed an association between shorter telomere length and poorer outcomes: no/poor response to antipsychotic medication33,50,53, no remission35, treatment-resistant schizophrenia54 and high symptom severity43,48.
Recently, telomere shortening has been associated with reduced hippocampal progenitor cell proliferation and the expression of genes regulating general cognitive functions55, reduced hippocampal volume56 and poor cognitive function in schizophrenia39,43. Cognitive reserve has been proposed as a mediator of symptomatology, functionality and cognition57,58,59,60, and having a high cognitive reserve predicts a better prognosis61. Based on the above, we hypothesized that, in schizophrenia, shorter telomeres reflect accelerated aging with reduced hippocampus proliferation that leads to worse cognitive function and poor response, which could translate into a higher risk of relapse after remission. Our results partially confirm this hypothesis, as shorter telomere length has been associated with poor cognition and relapse, but causality could not be demonstrated through mediation analysis. In our sample, no direct effect of cognitive function or symptom severity on relapse was detected. This could be related to the complexity of relapse as an outcome, being a complex phenotype that may not only be associated with the pathophysiological characteristics of patients but also with external factors (i.e., cannabis, lack of adherence). Moreover, the direct effect of shorter telomere on risk of relapse might not only be attributed to its effect on cognition but could also reflect the cumulative effect of environmental risk factors, such as psychosocial stress, obstetric complications or cannabis62,63,64,65,66, which in turn could also be related to relapse67,68.
These results should be interpreted in light of some limitations. Firstly, the sample size might limit the statistical power to detect a difference between groups or to stratify patients by antipsychotic medication. Secondly, although the Morinsky-Green scale was used to assess the adherence of the patients, our sample size was not large enough to stratify patients accordingly. Therefore, we were unable to separately analyze secondary relapse, which is commonly associated with non-adherence, and natural or primary relapse, which represents relapse in the absence of this influencer. Thirdly, our results regarding telomere length were obtained using an epigenetic predictor of length, not a direct measurement, so direct comparison with previous studies could be affected. Fourthly, due to the naturalistic design, drug treatment was not controlled, and the study participants maintained their usual treatment. Lastly, no specific scale was used to assess negative symptomatology, due to constraints associated with the PANSS scale. Although it is one of the most widely used measures of negative symptom severity, we acknowledge that it has several limitations. The use of Marder’s factors could solve some of these limitations. Finally, a limitation present in all CR studies undertaken on a psychiatric population is that as there is not yet a valid instrument to measure CR, criteria established and replicated in previous studies were followed. Besides these limitations, the strength of this study lies in the inclusion of a consistent well-characterized first-episode schizophrenia patient sample in remission due to its naturalistic and longitudinal design.
Our results provide preliminary evidence of the role of epigenetic aging in cognition and medium-term outcomes after remission. Further research is needed to validate our results in larger cohorts and to provide further explanation of the mechanistic relationship between epigenetic aging and relapse and the possible role of cognitive function and environmental variables.
Material and methods
Study design
This study is part of the project “Clinical and neurobiological determinants of second episodes of schizophrenia. Longitudinal study of first episode of psychosis” (PI11/00325) (2EPs Project), the aim of which is to identify and characterize the clinical, environmental and biological factors that predict a relapse. The 2EPs is a naturalistic, multicenter, coordinated and multimodal study of patients with a first psychotic episode of schizophrenia with less than 5 years of evolution and has a 3-year longitudinal-prospective follow-up design. The project includes six modules: general, neuroimaging, adherence, neurocognition, physical health and biological. Due to its main goals, the present study was framed within the general and biological modules. The first one aims to assess the presence or absence of relapses and includes clinical assessments. The aim of the biological module is to identify biomarkers potentially involved in second episodes (Bernardo et al., 2021; Gassó et al., 2021; Martínez-Pinteño et al., 2022; Rodríguez et al., 2022).
Subjects
The inclusion criteria for the 2EPs Project were a) age 16–40 years at the time of first assessment (baseline visit); b) meeting diagnostic criteria according to DSM-IV-TR for schizophrenia or schizophreniform disorder (American Psychiatric Association, 1994); c) being in remission from the first psychotic episode (which should have occurred within the last 5 years), according to Andreasen’s criteria (Andreasen et al., 2005); d) not having relapsed after the first psychotic episode; e) speaking Spanish fluently, and f) signing the informed consent form. The exclusion criteria were a) having experienced a traumatic brain injury with loss of consciousness; b) presenting intellectual disability, with an intelligence quotient (IQ) < 70 and presenting malfunctioning and problems with adaptive processes, and/or c) presenting somatic pathology with mental repercussion.
Of the 223 patients recruited in the 2EPs Project, 119 participants (53.4%) completed the study. Ninety-one (76.5%) of these participated in the biological module and provided a biological sample for DNA methylation analysis at baseline.
The study was approved by the investigation ethics committees of all participating clinical centers. Informed consent was obtained from all participants. For children under the age of 18 years old, parents or legal guardians gave written informed consent before the study started, and patients assented to participate. When requested, participants in the study were given a report on the results of the tests. This study was conducted in accordance with the Declaration of Helsinki.
Clinical assessment
At baseline demographic data and a complete personal and family history were collected in a systematic, self-devised interview. Diagnoses were determined according to the DSM-IV-TR criteria (American Psychiatric Association, 1994), using the SCID-I (Williams et al., 1992) or the Kiddie-SADS (Kaufman et al., 1997) depending on age.
Clinical symptomatology was assessed using the Spanish validated version of the Positive and Negative Syndrome Scale (PANSS) (Peralta & Cuesta, 1994). It has been argued that some PANSS items described as negative symptoms may be better described as cognitive deficits. Given this controversy, prior to our analyses we decided to use the Marder PANSS Factor Scores (Marder et al., 1997), which have different, more restrictive criteria for assessing both positive and negative symptomatology.
Pharmacological treatment was also recorded during all visits. The prescribed daily doses of antipsychotics were converted to chlorpromazine equivalent daily dose (CEED) following the method proposed by Leucht and colleagues (Leucht et al., 2016).
At baseline, a systematic survey of drug misuse habits was performed using part of the European adaptation of a multidimensional assessment instrument for drug and alcohol dependence: the multidimensional assessment tool European Addiction Severity Index (EuropAsi) (Kokkevi & Hartgers, 1995).
Cognitive assessment
The neuropsychological battery, assessed at baseline, measured the following cognitive domains: (1) Estimated IQ from Block Design and Vocabulary of the Wechsler Adult Intelligence Scale (WAIS-III) (Wechsler, 1997); (2) Verbal learning and memory, evaluated using the California Verbal Learning Test (CVLT) (Delis et al., 1987); (3) Sustained attention, assessed using the Continuous Performance Test–II (CPT-II) (Conners et al., 2003), version 5, corrected by age and educational level; (4) Processing speed, assessed using the Trail Making Test (Form A) (TMT-A) (Reitan & Wolfson, 1995) and Digit Symbol (WAIS-III); (5) Executive functioning, evaluated using the Tower of London (TOL) (Shallice, 1982); (6) Working memory, based on the Digit Span Subtest and the Letter-Number Sequencing Subtest of the WAIS-III; (7) Verbal memory, assessed using the Brief Visuospatial Memory Test-Revised (Benedict & Groninger, 1995); (8) Verbal fluency, evaluated using semantic fluency (animals) (Peña-Casanova, 1991) and F-A-S tests (Loonstra et al., 2001); and (9) Emotional intelligence, evaluated using the Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT) (Mayer et al., 2002).
A Principal Component Analysis (PCA) was performed between neuropsychological battery tests identifying the seven cognitive domains: verbal memory, visual memory, executive function, sustained attention, working memory, verbal fluency and processing speed (see Supplementary Table 3). Higher scores corresponded to better performance in all cognitive domains except for attention.
To assess cognitive reserve (CR) the three most commonly proposed proxy indicators of CR were used (Amoretti et al., 2016, 2018, 2022; de la Serna et al., 2013; González-Ortega et al., 2020): (1) The estimated premorbid IQ was calculated using the vocabulary subtest of the WAIS-III (Wechsler, 1997); (2) Education was assessed taking into account the degree of schooling attained and passed by the subject; and (3) Lifetime participation in leisure, social and physical activities was assessed using the Premorbid Adjustment Scale (PAS) (scholastic performance) and the Functioning Assessment Short Test (FAST) scale, which allowed us to assess specific life-domains such as interpersonal relationships and leisure time.
Relapse definition
The main outcome variables were relapse rates. As inclusion criteria, patients fulfilled Andreasen’s criteria of symptomatic remission to enter the study, being considered at risk of relapse over the 3-year period (Andreasen et al., 2005).
Relapse was defined as when participants stop fulfilling these remission criteria for at least one week of the follow-up, scoring 4 or more in any of the 8 items of the PANSS Scale used to define these criteria: delusions, unusual thought content, hallucinatory behavior, mannerisms/posturing, blunted affect, social withdrawal, and lack of spontaneity. Hospitalization was also reported in every follow-up visit and considered a relapse when it was related to schizophrenia symptoms (and not to other causes). Follow-up visits to detect relapses were scheduled every 3 months, at which information was collected from the entire period between visits, and the patients, family members or caregivers and clinical teams in charge of the clinical follow-up could notify the research team of the possible relapse of a participant.
Biological samples
Blood samples from each participant were collected at baseline in EDTA (BD Vacutainer K2EDTA tubes; Becton Dickinson, Franklin Lakes, New Jersey, USA). Genomic DNA was extracted using the MagNA Pure LC DNA Isolation Kit and a MagNA Pure LC 2.0 instrument (Roche Diagnostics GmbH, Mannheim, Germany) and DNA concentration and quality were measured using a NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific, Surrey, CA). Genome-wide DNA methylation was profiled at the Centro Nacional de Genotipado (CEGEN-PRB3-ISCIII) using the Illumina Infinium MethylationEPIC BeadChip Kit.
Methylation data collection
Raw intensity data (.IDAT) files were received and bioinformatics processes were conducted in house using the Chip Analysis Methylation Pipeline (ChAMP) Bioconductor package (Tian et al., 2017). Raw IDAT files were used to load the data into the R environment using the champ.load function, which also allows the probe quality control and removal steps to occur simultaneously. Probes with weak signals (p < 0.01) (n = 8441), cross-reactive probes (n = 11), non-CpG probes (n = 2914), probes with < 3 beads in at least 5% of the samples per probe (n = 7725), probes that bound to SNP (Single Nucleotide Polymorphisms) sites (n = 95,134), and sex chromosome probes (n = 16,445) were all considered problematic for the accurate detection of downstream methylation. After removing these probes, 735,248 probes remained for downstream analysis. β values were then normalized using the champ.norm function, specifically using the beta-mixture quartile method (BMIQ function). Next, the singular value decomposition (SVD) method was performed by champ.SVD to assess the amount and significance of the technical batch components in our dataset. Using the champ.runCombat function, combat algorithms were applied to correct for slide and array (significant components detected using the SVD method).
Calculation of the epigenetic age with different clocks
Four epigenetic clocks, including epigenetic clocks of chronological age (Horvath and Hannun clocks), mortality (PhenoAge) and telomere length (DNAmTL) (details in Table 3), were calculated using the methylclock R package (Pelegi-Siso et al., 2021). Several authors demonstrated that the epigenetic clocks are resistant to the lack of CpG sites missing from the EPIC (McEwen et al., 2018). Briefly, the package extracts methylation levels of CpGs included in each clock from normalized and batched corrected methylation data. Subsequently, the coefficients obtained through elastic net in the prediction models of each of the clocks in the original papers were used to calculate DNA methylation age and epigenetic age acceleration in years, except for the DNAmTL clock, which measures telomere length in base pairs. For each clock we obtained the DNA methylation predicted age (DNAm age) in years, and two values of age acceleration: (1) the intrinsic epigenetic age acceleration (IEAA) (Chen et al., 2016), an age residual obtained after regressing chronological age on DNAm age, which captures cellular age acceleration independently of blood cell proportions that are known to change with age; and (2) the extrinsic epigenetic age acceleration (EEAA) (Chen et al., 2016), a set of residuals obtained after regressing chronological age and seven blood cell type proportions on DNAm age, which incorporates intrinsic measures as well as blood cell proportions. We estimated blood cell type proportion (CD4 T-lymphocytes, CD8 T-lymphocytes, monocytes, beta-cell, NK, neutrophils and eosinophils) using the reference panel from Reinius et al. (Reinius et al., 2012), as implemented in the meffil package (Min et al., 2018).
Statistical analysis
Data were analyzed using SPSS 20.0 (statistical analysis software, IBM, Chicago, IL, USA). Two-tailed p-values < 0.05 were considered to be of statistical significance. Means and standard deviations were computed for continuous variables. The normality of continuous variables was tested using the Kolmogorov–Smirnov and Shapiro–Wilk tests, and the equality of the variance between groups was assessed using Levene’s test. The between-group difference in the continuous variables was analyzed using a Student’s t-test or Mann–Whitney U-test. The relationship between continuous variables was analyzed using partial correlations adjusted by potential confounding variables. A mediation analysis, using the Mediation R package, was carried out to evaluate the possible mediating role of clinical or neuropsychological variables on an association between epigenetic age acceleration and relapse (indirect effect). Regression coefficients were constructed using conventional mediation analysis models with a bootstrap sample size of 1000 and a 95% confidence interval.
Data availability
The clinical data that support the findings of this study are not openly available due to contain human data and are available from the corresponding author upon reasonable request.
References
Garcia-Rizo, C., Fernandez-Egea, E., Bernardo, M. & Kirkpatrick, B. The thrifty psychiatric phenotype. Acta Psychiatr. Scand. 131, 18–20 (2015).
Nordentoft, M. et al. Excess mortality, causes of death and life expectancy in 270,770 patients with recent onset of mental disorders in Denmark, Finland and Sweden. PLoS ONE 8, e55176 (2013).
Saha, S., Chant, D. & Mcgrath, J. A systematic review of mortality in schizophrenia is the differential mortality gap worsening over time? Population-based studies that re-ported primary data on deaths in people with schizo-phrenia. Arch. Gen. Psychiatry 64, 1123–1131 (2007).
Momen, N. C. et al. Mortality associated with mental disorders and comorbid general medical conditions. JAMA Psychiatry (2022) https://doi.org/10.1001/JAMAPSYCHIATRY.2022.0347.
Kirkpatrick, B., Messias, E., Harvey, P. D., Fernandez-Egea, E. & Bowie, C. R. Is schizophrenia a syndrome of accelerated aging? Schizophr. Bull 34, 1024–1032 (2008).
Kirkpatrick, B. & Kennedy, B. K. Accelerated aging in schizophrenia and related disorders: future research. Schizophr. Res 196, 4–8 (2018).
López-Otín, C., Blasco, M. A., Partridge, L., Serrano, M. & Kroemer, G. The hallmarks of aging. Cell 153, 1194 (2013).
Horvath, S. DNA methylation age of human tissues and cell types. Genome Biol. 14, R115 (2013).
Hannum, G. et al. Genome-wide methylation profiles reveal quantitative views of human aging rates. Mol. Cell 49, 359–367 (2013).
Horvath, S. & Raj, K. DNA methylation-based biomarkers and the epigenetic clock theory of ageing. Nat. Rev. Genet. 19, 371–384 (2018).
Marioni, R. E. et al. DNA methylation age of blood predicts all-cause mortality in later life. Genome Biol. 16, 25 (2015).
Richetto, J. & Meyer, U. Epigenetic modifications in schizophrenia and related disorders: molecular scars of environmental exposures and source of phenotypic variability. Biol. Psychiatry 89, 215–226 (2021).
McKinney, B. C., Lin, H., Ding, Y., Lewis, D. A. & Sweet, R. A. DNA methylation age is not accelerated in brain or blood of subjects with schizophrenia. Schizophr. Res. 196, 39–44 (2018).
McKinney, B. C., Lin, H., Ding, Y., Lewis, D. A. & Sweet, R. A. DNA methylation evidence against the accelerated aging hypothesis of schizophrenia. NPJ Schizophr. 3, 13 (2017).
Okazaki, S. et al. Epigenetic clock analysis of blood samples from Japanese schizophrenia patients. NPJ Schizophr. 5, 4 (2019).
Kowalec, K. et al. Methylation age acceleration does not predict mortality in schizophrenia. Transl. Psychiatry 9, 157 (2019).
Voisey, J. et al. Epigenetic analysis confirms no accelerated brain aging in schizophrenia. NPJ Schizophr 3, 26 (2017).
Viana, J. et al. Schizophrenia-associated methylomic variation: molecular signatures of disease and polygenic risk burden across multiple brain regions. Hum. Mol. Genet. 26, 210–225 (2017).
Wu, X., Ye, J., Wang, Z. & Zhao, C. Epigenetic age acceleration was delayed in schizophrenia. Schizophr. Bull. 47, 803–811 (2021).
Levine, M. E. et al. An epigenetic biomarker of aging for lifespan and healthspan. Aging 10, 573–591 (2018).
Lu, A. T. et al. DNA methylation-based estimator of telomere length. Aging 11, 5895–5923 (2019).
Higgins-Chen, A. T., Boks, M. P., Vinkers, C. H., Kahn, R. S. & Levine, M. E. Schizophrenia and epigenetic aging biomarkers: increased mortality, reduced cancer risk, and unique clozapine effects. Biol. Psychiatry 88, 224–235 (2020).
Dada, O. et al. Biological aging in schizophrenia and psychosis severity: DNA methylation analysis. Psychiatry Res. 296, 113646 (2021).
Wolf, E. J. et al. Traumatic stress and accelerated DNA methylation age: a meta-analysis. Psychoneuroendocrinology 92, 123–134 (2018).
Wolf, E. J. et al. Posttraumatic psychopathology and the pace of the epigenetic clock: a longitudinal investigation. Psychol. Med. 49, 791–800 (2019).
Chen, B. H. et al. DNA methylation-based measures of biological age: meta-analysis predicting time to death. Aging 8, 1844–1865 (2016).
Franceschi, C. et al. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann. N. Y. Acad. Sci. 908, 244–254 (2000).
Ermakov, E. A., Melamud, M. M., Buneva, V. N. & Ivanova, S. A. Immune system abnormalities in schizophrenia: an integrative view and translational perspectives. Front. Psychiatry 13, 880568 (2022).
Luo, C. et al. Subtypes of schizophrenia identified by multi-omic measures associated with dysregulated immune function. Mol. Psychiatry 26, 6926–6936 (2021).
Rebouças, D. B. et al. Accelerated aging signatures in subjects with schizophrenia and their unaffected siblings. J. Psychiatr. Res. 139, 30–37 (2021).
Aas, M. et al. Telomere length is associated with childhood trauma in patients with severe mental disorders. Transl. Psychiatry 9, (2019).
Squassina, A. et al. Telomere attrition and inflammatory load in severe psychiatric disorders and in response to psychotropic medications. Neuropsychopharmacology 45, 2229–2238 (2020).
Yu, W. Y., Chang, H. W., Lin, C. H. & Cho, C. L. Short telomeres in patients with chronic schizophrenia who show a poor response to treatment. J. Psychiatry Neurosci. 33, 244–247 (2008).
Fernandez-Egea, E. et al. Telomere length and pulse pressure in newly diagnosed, antipsychotic-naive patients with nonaffective psychosis. Schizophr. Bull. 35, 437–442 (2009).
Kota, L. N., Purushottam, M., Moily, N. S. & Jain, S. Shortened telomere in unremitted schizophrenia. Psychiatry Clin. Neurosci. 69, 292–297 (2015).
Czepielewski, L. S. et al. Telomere length in subjects with schizophrenia, their unaffected siblings and healthy controls: evidence of accelerated aging. Schizophr. Res. 174, 39–42 (2016).
Galletly, C. et al. Shorter telomere length in people with schizophrenia: a preliminary study from Australia. Schizophr. Res. 190, 46–51 (2017).
Monroy-Jaramillo, N. et al. Leukocyte telomere length in Hispanic schizophrenia patients under treatment with olanzapine. J. Psychiatric Res. 90, 26–30 (2017).
Czepielewski, L. S. et al. Telomere length and CCL11 levels are associated with gray matter volume and episodic memory performance in schizophrenia: evidence of pathological accelerated aging. Schizophr. Bull. 44, 158–167 (2018).
Russo, P. et al. Shorter telomere length in schizophrenia: evidence from a real-world population and meta-analysis of most recent literature. Schizophr. Res. 202, 37–45 (2018).
Polho, G. B., De-Paula, V. J., Cardillo, G., dos Santos, B. & Kerr, D. S. Leukocyte telomere length in patients with schizophrenia: a meta-analysis. Schizophr. Res. 165, 195–200 (2015).
Rao, S., Ye, N., Hu, H., Shen, Y. & Xu, Q. Variants in TERT influencing telomere length are associated with paranoid schizophrenia risk. Am. J. Med. Genet. 171, 317–324 (2016).
Vaez-Azizi, L. M. et al. Telomere length variability is related to symptoms and cognition in schizophrenia. Schizophr. Res. 164, 268–269 (2015).
Schürhoff, F. et al. No alteration of leukocyte telomere length in first episode psychosis. Psychiatry Res. 301, 113941 (2021).
Malaspina, D. et al. Telomere length, family history, and paternal age in schizophrenia. Mol. Genet. Genomic Med. 2, 326–331 (2014).
Riley, G. et al. Telomere length and early trauma in schizophrenia. Schizophr. Res. 199, 426–430 (2018).
Mansour, H. et al. Does telomere length mediate associations between inbreeding and increased risk for bipolar I disorder and schizophrenia? Psychiatry Res. 188, 129–132 (2011).
Çevik, B. et al. Psychometric liability to psychosis and childhood adversities are associated with shorter telomere length: a study on schizophrenia patients, unaffected siblings, and non-clinical controls. J. Psychiatric Res. 111, 169–185 (2019).
Wolkowitz, O. M. et al. Leukocyte telomere length: effects of schizophrenia, age, and gender. J. Psychiatric Res. 85, 42–48 (2017).
Lin, P. Y. Shortened leukocyte telomere length in patients with schizophrenia is related to disease status. Schizophr. Res. 168, 597–598 (2015).
Nieratschker, V. et al. Longer telomere length in patients with schizophrenia. Schizophr. Res. 149, 116–120 (2013).
Talarico, F. et al. Aging biological markers in a cohort of antipsychotic-naïve first-episode psychosis patients. Psychoneuroendocrinology 132, 105350 (2021).
Pawelczyk, T., Szymanska, B., Grancow-Grabka, M., Kotlicka-Antczak, M. & Pawelczyk, A. Telomere length in blood cells is related to the chronicity, severity, and recurrence rate of schizophrenia. Neuropsychiatr. Dis. Treat. 11, 1493–1503 (2015).
Squassina, A. et al. Telomere attrition and inflammatory load in severe psychiatric disorders and in response to psychotropic medications. Neuropsychopharmacology 45, 2229–2238 (2020).
Palmos, A. B. et al. Telomere length and human hippocampal neurogenesis. Neuropsychopharmacology (2020) https://doi.org/10.1038/s41386-020-00863-w.
Shivakumar, V. et al. Telomere length and its association with hippocampal gray matter volume in antipsychotic-naïve/free schizophrenia patients. Psychiatry Res. Neuroimaging 282, 11–17 (2018).
Amoretti, S. et al. The impact of cognitive reserve in the outcome of first-episode psychoses: 2-year follow-up study. Eur. Neuropsychopharmacol. 26, 1638–1648 (2016).
Amoretti, S. et al. Cognitive reserve as an outcome predictor: first-episode affective versus non-affective psychosis. Acta Psychiatr. Scand. 138, 441–455 (2018).
González-Ortega, I. et al. Influence of social cognition as a mediator between cognitive reserve and psychosocial functioning in patients with first episode psychosis. Psychol. Med. 50, 2702–2710 (2020).
Amoretti, S. et al. The impact of cognitive reserve, cognition and clinical symptoms on psychosocial functioning in first-episode psychoses. Psychol. Med. 52, 526–537 (2022).
Amoretti, S. et al. Identifying clinical clusters with distinct trajectories in first-episode psychosis through an unsupervised machine learning technique. Eur. Neuropsychopharmacol. 47, 112–129 (2021).
Clark, S. L. et al. Methylomic investigation of problematic adolescent cannabis use and its negative mental health consequences. J. Am. Acad. Child Adolesc. Psychiatry 60, 1524–1532 (2021).
Zannas, A. S. Epigenetics as a key link between psychosocial stress and aging: concepts, evidence, mechanisms. Dialogues Clin. Neurosci. 21, 389–396 (2019).
Hoare, J. et al. Accelerated epigenetic aging in adolescents from low-income households is associated with altered development of brain structures. Metab. Brain Dis. 35, 1287–1298 (2020).
Marini, S. et al. Adversity exposure during sensitive periods predicts accelerated epigenetic aging in children. Psychoneuroendocrinology 113, 104484 (2020).
Coimbra, B. M. et al. The impact of neighborhood context on telomere length: a systematic review. Health Place 74, 102746 (2022).
Bioque, M. et al. Clinical and treatment predictors of relapse during a three-year follow-up of a cohort of first episodes of schizophrenia. Schizophr. Res. 243, 32–42 (2022).
Donaldson, K. R. et al. Dynamic interplay between life events and course of psychotic disorders: 10-year longitudinal study following first admission. Psychol. Med. (2020) https://doi.org/10.1017/S0033291720003992.
Acknowledgements
This study was supported by the Carlos III Healthcare Institute, the Spanish Ministry of Science, Innovation and Universities, the European Regional Development Fund (ERDF/FEDER) (PI08/0208, PI11/00325, PI14/00612); Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM); CERCA Program; Catalan Government, the Secretariat of Universities and Research of the Department of Enterprise and Knowledge (2017SGR1562 and 2017SGR1355) and Institut de Neurociències, Universitat de Barcelona. The authors thank the Language Advisory Service at the University of Barcelona for manuscript revision. The authors also thank all subjects and their families for the time and effort spent on this study as well as Ana Meseguer for sample collection assistance.
Author information
Authors and Affiliations
Consortia
Contributions
The results presented here are part of a broader project, the 2EPS study. M.Be. is the coordinator of the 2EPS study. A.G.S. and L.l.P. performed the sample isolation and preparation, performed the statistical analysis and wrote the first draft of the manuscript, and both authors contributed equally to this work. G.M., S.A. and M.B. participated in the coordination of the sample shipment, the maintenance of the 2EPS database and in the recruitment and assessment of the sample. E.B. is the coordinator of the Biological module of the 2EPS study. M.R., X.G.-B., L.R. D.B., R.R.-J., A.R., E.P.-C., A.I., J.U., M.G.-P., M.J.C., M.P. and A.G.-P. participated in the recruitment and assessment of the sample. S.M. designed, supervised and performed the statistical analysis, performed the interpretation of the results and wrote the first draft of the manuscript. All the authors, including the 2EPSs group authors listed in the acronym, contributed to the final draft of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
A.I. has received research support from or served as speaker or advisor for Janssen-Cilag, Lundbeck and Otsuka. A.G.-P. has received grants and served as consultant, advisor or CME speaker for the following entities: Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Sanofi-Aventis, Exeltis, the Spanish Ministry of Science and Innovation (CIBERSAM), the Ministry of Science (Carlos III Institute), and the Basque Government. J.S.-R. has been as speaker for and on the advisory boards of Adamed, Lundbeck, Servier, Medtronic, Casen Recordati, Neurofarmagen, Otsuka, Indivior, Lilly, Schwabe, Janssen and Pfizer, outside the submitted work. M.B. has been a consultant for, received grant/research support and honoraria from, and been on the speakers/advisory board of ABBiotics, Adamed, Angelini, Casen Recordati, Janssen-Cilag, Menarini and Rovi. T.M.B. has been a consultant for, received grant/research support and honoraria from, and been on the speakers/advisory board of has received honoraria from talks and/or consultancy of Adamed, Angelini, Ferrer, Janssen-Cilag, Lundbeck, Neuraxpharm, Otsuka, Pfizer and Sanofi, and grants from Spanish Ministry of Health, Instituto de Salud Carlos III. M.G.F. has been on the speakers/advisory board of Janssen-Cilag. P.A.S. has been a consultant to and/or has received honoraria or grants from Adamed, CIBERSAM, European Comission, Government of the Principality of Asturias, Instituto de Salud Carlos III, Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Plan Nacional Sobre Drogas and Servier. R.R.-J. has been a consultant for, spoken in activities of, or received grants from: Instituto de Salud Carlos III, Fondo de Investigación Sanitaria (FIS), Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Madrid Regional Government (S2010/ BMD-2422 AGES; S2017/BMD-3740), JanssenCilag, Lundbeck, Otsuka, Pfizer, Ferrer, Juste, Takeda, Exeltis, Casen-Recordati, Angelini. The rest of the authors reported no biomedical financial interests or potential conflicts of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Segura, ÀG., Prohens, L., Mezquida, G. et al. Epigenetic clocks in relapse after a first episode of schizophrenia. Schizophr 8, 61 (2022). https://doi.org/10.1038/s41537-022-00268-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41537-022-00268-2
This article is cited by
-
Time to relapse in chronic lymphocytic leukemia and DNA-methylation-based biological age
Clinical Epigenetics (2023)
