
Abstract
Cigarette smoking has a negative effect on respiratory and skeletal muscle function and is a risk factor for various chronic diseases. To assess the effects of 14 days of smoking cessation on respiratory and skeletal muscle function, markers of inflammation and oxidative stress in humans. Spirometry, skeletal muscle function, circulating carboxyhaemoglobin levels, advanced glycation end products (AGEs), markers of oxidative stress and serum cytokines were measured in 38 non-smokers, and in 48 cigarette smokers at baseline and after 14 days of smoking cessation. Peak expiratory flow (p = 0.004) and forced expiratory volume in 1 s/forced vital capacity (p = 0.037) were lower in smokers compared to non-smokers but did not change significantly after smoking cessation. Smoking cessation increased skeletal muscle fatigue resistance (p < 0.001). Haemoglobin content, haematocrit, carboxyhaemoglobin, total AGEs, malondialdehyde, TNF-α, IL-2, IL-4, IL-6 and IL-10 (p < 0.05) levels were higher, and total antioxidant status (TAS), IL-12p70 and eosinophil numbers were lower (p < 0.05) in smokers. IL-4, IL-6, IL-10 and IL-12p70 had returned towards levels seen in non-smokers after 14 days smoking cessation (p < 0.05), and IL-2 and TNF-α showed a similar pattern but had not yet fully returned to levels seen in non-smokers. Haemoglobin, haematocrit, eosinophil count, AGEs, MDA and TAS did not significantly change with smoking cessation. Two weeks of smoking cessation was accompanied with an improved muscle fatigue resistance and a reduction in low-grade systemic inflammation in smokers.
Similar content being viewed by others


Introduction
Cigarette smoking still is a public health concern and a risk factor for many chronic diseases, including chronic obstructive pulmonary disease (COPD), lung cancer and cardiovascular diseases1,2. It is the leading cause of preventable death and 77,900 deaths in the United Kingdom were directly or indirectly attributable to smoking in 2016 3. In England, between 2017 and 2018, an estimated 489,300 smoking-related admissions to hospitals were reported4.
The adverse health effects are a consequence of a combination of thousands of toxic and/or carcinogenic substances, including carbon monoxide (CO), reactive glycation compounds, known as glycotoxins, and nicotine in cigarette smoke5,6,7. In addition, the low-grade systemic inflammation and oxidative stress in smokers increases the risk of atherosclerosis8,9,10,11,12. Smoking is associated with elevated serum cholesterol and triglyceride levels, impaired glucose tolerance and reduced insulin sensitivity13. It has been reported that in diabetic people, a reduced insulin sensitivity could lead to glycation of myofibrillar proteins14 that may be further aggravated by glycotoxins in cigarette smoke that can also react with serum proteins to form advanced glycation end products (AGEs)6.
In addition to the health burden of cigarette smoking and the potential adverse effect on respiratory function15,16, smoking can also have a negative impact on muscle function17,18,19. Part of the potential detrimental effect of cigarette smoking may be attributable to the negative impact on the oxygen delivery to tissues, including skeletal muscles, that may in turn result in exercise intolerance and a reduced muscle fatigue resistance20,21,22. Such an impaired oxygen delivery is at least partly attributable to the CO in the cigarette smoke that strongly binds to haemoglobin (Hb), forming carboxyhaemoglobin (COHb)23. This not only reduces the oxygen carrying capacity of the blood, but also causes a left-shift of the Hb-dissociation curve. The significance of elevated COHb levels has been illustrated by an acute CO-induced reduction in muscle fatigue resistance in healthy people24. In addition, CO and cyanide may also directly impair mitochondrial respiration25,26. As fatigue resistance was similar in COPD patients who had quit smoking and healthy age-matched non-smokers27, we hypothesised that the effect of smoking on skeletal muscle fatigue is readily reversible by smoking cessation .
Smoking cessation is an important step to stop or reverse many of the detrimental effects of smoking and is considered a highly effective way to reduce morbidity and mortality28 and slow down the accelerated decline in FEV129,30. In fact, smoking cessation is considered one of the main actions to attenuate the progression of COPD31,32. In line with this, it has been seen in mice, that the smoking-induced lung inflammation, mitochondrial dysfunction, limb and diaphragm muscle atrophy, and elevated IL-1α and TNF-α levels were normalised after smoking cessation26,33. In addition, if CO is an important cause of a reduced muscle fatigue resistance and exercise tolerance, we expect that smoking cessation, resulting in a quick normalisation of the COHb levels34, will be associated with a concomitant improvement in muscle function. Therefore, we hypothesise, that just two weeks of smoking cessation is sufficient to detect measurable improvements in muscle fatigue resistance, and diminished levels of circulating inflammatory markers and oxidative stress. As there is some indication that smoking may cause a larger reduction in pulmonary function than in men35 and that women have a higher muscle fatigue resistance than men36 we were also interested in potential sex differences in the response to smoking cessation.
Methods
Participants
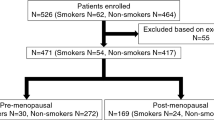
Cigarette smokers (men n = 28; women n = 20) and non-smokers (men n = 23; women n = 15) were recruited from the local community and Manchester Metropolitan University (MMU). Participants were 18 to 44 years old, and smokers had smoked for ≥ 1 year and ≤ 17 years. All participants self-reported as being free of symptoms of chronic diseases. In cigarette smokers, all measurements were repeated after 14 days of smoking cessation. The study was approved by the Science and Engineering Research Ethics and Governance Committee at MMU (Ethics reference number: 5944) and performed in accordance to the principles stated in the Declaration of Helsinki. All participants provided written informed consent before participating.
Height and body mass were assessed using a stadiometer and digital scales, respectively. Body mass index (BMI) was calculated. Smoking history was assessed by questionnaire. Smoking volume (SV) was given as pack years, calculated as the current number of packs of cigarettes smoked per day times the number of years smoked.
Outcome measures
Carboxyhaemoglobin (COHb)
A hand-held CO meter (Micro Smokerlyzer, Bedfont Scientific Ltd.; Kent, UK) was used to measure the percentage of the haemoglobin (Hb) oxygen binding sites occupied by CO (%COHb). The measurements were performed according to the recommendations of the manufacturer37.
Spirometry
Spirometry was conducted using a Micro Medical Spiro USB Spirometer and analysed with Spida 5 software (Cardinal Health, UK). Spirometry was completed in accordance with the American Thoracic Society and European Respiratory Society guidelines38. Each participant completed a minimum of three successful manoeuvres with at least 1–2 min rest between each manoeuvre while wearing a nose clip. The manoeuvres were rejected if: participants prematurely stopped exhalation, coughed during the first second of exhalation, lips were not fully sealed around the mouthpiece and/or the effort appeared submaximal. The test session was concluded when the largest two FEV1 and the largest two FVC were each within 0.15 L of each other in at least 3 manoeuvres38. If these criteria were not met, a maximum of eight manoeuvres were repeated until the criteria were met. Parameters assessed included: FEV1, FVC, FEV1/FVC ratio, Peak Expiratory Flow (PEF), and predicted values. The coefficient of variation (CV) for FEV1, FVC and PEF was 2.09%, 2.25% and 2.80%, respectively.
Maximal voluntary contraction (MVC)
A dynamometer chair was used to measure the MVC during knee extension. Participants were seated with the hip joint in 90° flexion, knee joint angle at 80° and the pelvis strapped to minimise accessory movements. All the measurements were performed on the right thigh. During the MVC, participants received verbal encouragement and visual feedback of the torque signal18,19,24,27. Participants performed the MVC twice with two minutes rest between each contraction to prevent development of fatigue. Knee extensor (KE) torque was recorded with a digital acquisition system (Acknowledge, Biopac Systems, Santa Barbara, CA, USA) at 200 Hz, and the highest value was reported as maximal muscle strength18. The CV for the MVC was 4.24%.
Voluntary activation (VA) and muscle fatigue resistance
To assess the VA and muscle fatigue resistance of the quadriceps muscle, carbon–rubber pads (7.5 cm × 13 cm, Axelgaard, USA) were used to apply percutaneous electrical stimulation (square wave, pulse width 200 μs; DSV Digitimer Stimulator, Digitimer Ltd., Herts, UK). The cathode was placed over the distal third of the thigh and the anode over the proximal part of the quadriceps. The electrical stimulation voltage was set at 400 V. To assess the supra-maximal current, single pulses were administered at 30-s intervals with increases in current of 50–100 mA to the relaxed muscle until no further increase in torque was noticed.
To assess the VA during an MVC, the interpolated twitch technique was used18,19 and calculated as:
and had a CV of 5.96%.
The fatigue resistance of the quadriceps muscles was determined by a series of electrically-evoked isometric 30-Hz trains, 1 s on 1 s off, for 2 min at a current that elicited 30% MVC at the start of the test19,27. The fatigue index (FI) was calculated as the final torque as a percentage of the initial torque during the series of the isometric contractions. The CV was 6.44%.
Haematology parameters and oxidative stress biomarkers
From 9 non-smokers and 20 smokers venous blood was collected from the antecubital vein and repeated after 2 weeks of smoking cessation from smokers only. After determination of the haematocrit (%Hct) the blood was collected in 4-mL vacutainers without anticoagulants (BD Vacutainer, Becton Dickinson Company, USA). The blood samples were allowed to clot for 15 min and serum was separated from whole blood by centrifugation (20 min; 500 × g) at room temperature. Following centrifugation, the serum was aliquoted in 1-mL microcentrifuge tubes, frozen and stored at − 80 °C until further analysis.
Serum protein, albumin and glucose concentrations were measured colourimetrically using Biuret reagent Randox kits using RandoxRX Daytona analyser (Randox Laboratories Ltd., Belfast, Ireland). The glucose concentration was determined after enzymatic oxidation in the presence of glucose oxidase. The Hb concentration was determined with a HemoCue (HemoCue® Hb 201 + System). Blood cell counts included agranulocytes (lymphocytes, monocytes) and granulocytes (neutrophils, eosinophils and basophils). Serum cytokines levels were quantified using flow cytometry. Briefly, positive and negative controls were used to set up the flow cytometer (BD FACScalibur, Becton Dickinson Company, USA) and analysed using the high flow setting (FL2 channel), using Cell Quest Pro software and flowcytomix software. The software translated the flow cytometric results into cytokine concentrations (pg mL−1). Serum malondialdehyde (MDA), a marker of lipid peroxidation, was quantified spectrophotometrically using a lipid peroxidation kit (Oxford Biomedical Research, UK). The serum total antioxidant status (TAS) in was analysed using the TAS kit (Randox Laboratories Ltd., Belfast, Ireland) according to the recommendations by the manufacturer. The abundance of low molecular weight (LMW) AGEs were assessed using a spectrofluorimeter (BioTek, USA), and total AGEs were assessed by ELISA (Cell Biolabs, United States). All tests were carried out in duplicate and averaged.
Statistical analysis
Statistical analyses were performed using SPSS 24.0 (IBM Corporation, NY, US). Data were assessed for normality with the Shapiro–Wilk tests. If the data were not normally distributed, non-parametric Kruskal–Wallis H test was performed. A two-way univariate ANOVA with as between factors group (smokers, non-smokers and smoking cessation) and sex was used. If a significant group effect, or a group * sex interaction was found, a Dunnet post-hoc test with as standard group the smokers was performed to locate the significant differences. For the blood parameters, comparisons between smokers and non-smokers, and comparison of smokers before and after cessation were performed with unpaired student t-tests. Differences were considered significant at p < 0.05. All data are presented as mean ± SD.
Results
Anthropometric details of the participants are presented in Table 1. The smoking women in our study had smoked longer and had smoked more pack years than the smoking men (p < 0.05; Table 1). For none of the parameters group * sex interactions were found, indicating that there were no significant differences in the responses to smoking and smoking cessation between men and women.
The total protein, albumin and glucose concentrations did not differ significantly between smokers and non-smokers (Table 2). Smokers had higher levels of COHb than non-smokers (p < 0.001) and the COHb levels had returned to levels similar to that in non-smokers after 14 days of smoking cessation (Table 3).
Spirometry
PEF, FEV1 and FVC were higher in men than women (p < 0.001), but FEV1/FVC, FEV1pred%, FVCpred% and PEFpred% did not differ significantly between men and women (Table 4). There was no significant difference in FEV1, FEV1pred%, FVCpred% and PEFpred% between smokers and non-smokers (Table 4), but PEF (p = 0.004; Table 4) and FEV1/FVC (p = 0.037; Fig. 1) were lower in smokers than in non-smokers. Neither changed significantly over the 14 days of smoking cessation (p > 0.05; Fig. 1 and Table 4).

The effect of smoking and 14 days smoking cessation on FEV1/FVC: Forced expiratory volume in one second/forced vital capacity; data are mean ± SD; *: significantly different from Non-smokers at p < 0.05.
Muscle function
Knee extension MVC was higher in men than women (p < 0.001; Table 4) and FI was higher in women than men (p < 0.001), but there were no significant sex differences in VA (p = 0.096; Table 4). There was no significant difference in MVC and VA between smokers and non-smokers (Table 4). While there was no significant difference in FI between smokers and non-smokers, smoking cessation resulted in an increased FI (p < 0.001; Fig. 2).

The effect of smoking and 14 days smoking cessation on fatigue index. Data are mean ± SD; ∞: significantly different from men at p < 0.05; α: significantly different from smokers at p < 0.05.
Haematology
There were no significant differences in total white blood cell, neutrophil, lymphocyte, monocyte and basophil counts between smokers and non-smokers (Table 3). The eosinophil count was lower in smokers than non-smokers (p < 0.05) even after 14 days smoking cessation (Table 3). Smokers had a higher haemoglobin concentration and haematocrit than non-smokers (p < 0.001) and was not changed significantly after 14 days of smoking cessation (Table 3).
Circulating markers of oxidative stress
The total antioxidant status was lower in smokers than non-smokers (p < 0.001) and was not significantly changed after 14 days of smoking cessation (Fig. 3a). Lipid peroxidation, in the form of the concentration of MDA was higher in smokers compared to non-smokers (p < 0.001) and were not significantly changed after 14 days of smoking cessation (Fig. 3b). Although the low molecular weight AGE levels did not differ significantly between smokers and non-smokers (Fig. 3c), the total AGE levels were higher in smokers compared to non-smokers (p < 0.05; Fig. 3d). Smoking cessation did not have a significantly alter the concentration of AGEs (Fig. 3c,d).

Effects of smoking and 14 days smoking cessation. (a) Total antioxidant status (TAS); (b) Malondialdehyde concentration; (c) Low molecular weight (LMW) advanced glycation end products (AGEs) fluorescence; (d) AGEs concentration; data are mean ± SD; *: significantly different from Non-smokers at p < 0.05.
Circulating levels of cytokines
Smokers had higher circulating levels of TNF-α, IL-2, IL-4, IL-6 and IL-10 levels than non-smokers (All p < 0.001; Fig. 4a–e), while IL-12p70 levels were lower in smokers than in non-smokers (p < 0.001; Fig. 4f). Almost all circulating cytokines concentrations returned to levels seen in non-smokers after 14 days of smoking cessation, except for TNF-α and IL-2 that though reduced, where still elevated in comparison to non-smokers (p < 0.05; Fig. 4a,b). TNF-β, IFN-γ, IL-1β, IL-5 did not differ significantly between smokers and non-smokers (Table 5).

Effects of smoking and 14 days smoking cessation (a) TNF-α: tumour necrosis factor-alpha; (b) IL-2: interleukin-2; (c) IL-4: interleukin-4; (d) IL-6: interleukin-6; (e) IL-10: Interleukin-10; (f) IL-12p70: interleukin-12p70; data are presented as mean ± SD; *: significantly different from Non-smokers at p < 0.05; α: significantly different from smokers at p < 0.05.
Discussion
The main observation of the present study was that in smokers with normal spirometry 14 days of smoking cessation resulted in a normalisation of skeletal muscle fatigue resistance and a return of circulating markers of inflammation. This indicates that even as little as 14 days of smoking cessation can confer measurable benefits that may encourage smokers in their smoking cessation efforts.
Differences between smokers and non-smokers
Spirometry
The present study confirms that FEV1, FVC and PEF were higher in men than women39. The spirometry in smokers was similar to that of non-smokers, except for a lower FEV1/FVC, indicative of some minor developing airway obstruction.
Muscle function
In line with previous observations18,19,40, we found that the maximal strength of the knee extensor muscles in smokers was similar to that in non-smokers. Others, however, have reported a lower force generating capacity in smokers41,42,43,44. Although part of a lower strength may at least in theory be attributable to a lower ability to voluntarily activate the muscle, we found no difference in voluntary activation between smokers and non-smokers, and if anything, even an increased VA has been reported in smokers19. The latter may be the result of an increased sympathetic nerve activity in smokers, possibly due to a central stimulant action of nicotine45,46. Whatever the cause of the discrepancy between studies concerning the impact of smoking on the MVC, it indicates that smoking per se is not necessarily associated with muscle weakness.
Somewhat unexpected was the absence of lower fatigue resistance in smokers that was seen in previous studies using the same fatigue protocol18,19. This reduced fatigue resistance in the previous smokers was thought to be at least partly attributable to elevated COHb levels, seen also in the current and other studies23,47 that not only reduces the oxygen carrying capacity, but also the release of oxygen due to the left-shift of the Hb-dissociation curve17,24. It should be noted, however, that 6% COHb reduced skeletal muscle fatigue resistance24 and the 3% COHb in our participants may not have had a measurable impact on the oxygen delivery to the skeletal muscle, and hence the fatigue resistance.
Blood parameters
While we did not see a significant difference in the albumin and total protein concentrations in the blood of smokers and non-smokers, others did see that smokers had a lower total protein and albumin concentration compared to non-smokers48 or even a higher protein concentration49. Consistent with previous studies50,51,52, the haemoglobin concentration and haematocrit were higher in smokers compared to non-smokers. The higher haemoglobin concentration may well be an adaptation to maintain the oxygen carrying capacity in the face of elevated COHb levels53,54.
Although there were no significant differences in monocytes and lymphocytes between smokers and non-smokers in the current and previous studies52,55, except for a reduction in the number of eosinophils, we observed a significant increase in TNF-α, IL-2, IL-4, IL-6 and IL-10. This suggests that smoking activates mononuclear cells to release cytokines. In line with this, it has been observed that cigarette smoke induces the release of TNF-α in an in vitro macrophage model system56, but others found no increased release of TNF-α peripheral blood mononuclear cells to cigarette smoke extracts57. It should be noted, however, that TNF-α is not only produced by blood mononuclear cells, but also by epithelial cells, fibroblasts and smooth muscle cells58, p. 229 and perhaps mononuclear and epithelial cells in the lung of smokers59. In line with this, it has been observed that there was a significantly elevated number of macrophages and neutrophils in the broncheo-alveolar lavage fluid of smoking mice26. Therefore, lung-derived cytokines may well be the prime explanation of the higher TNF-α, IL-2, IL-4, IL-6 and IL-10 concentrations and the lower level of the anti-inflammatory IL-12p70 concentration in smokers than non-smokers, indicating that even young-adult asymptomatic smokers suffer from a low-grade systemic inflammation.
It is possible that the lower TAS and higher MDA levels in smokers, also reported by others60, may be due to this low-grade systemic inflammation. The oxidative stress in smokers may well have contributed to their elevated AGE levels6,61,62. Although AGEs are often considered to represent indirectly a high level of glucose63,64, we and others49 did not find elevated glucose levels in smokers. It should be noted that not only high glucose concentrations, but also toxic constituents of cigarette smoke might induce glycotoxins that rapidly react with protein to form AGE6. Therefore, we suggest that the increased AGEs in asymptomatic young-adult smokers is primarily attributable to glycotoxins, oxidative stress, and to some extent secondary to the low-grade systemic inflammation.
Smoking cessation
Spirometry
The present study showed that 14 days of smoking cessation did not result in an improvement in the smoking-induced decrement of FEV1/FVC. This is supported by numerous studies suggesting that pulmonary changes induced by smoking are irreversible, even though smoking cessation is the best approach to stop the accelerated decline in lung function in smokers65,66,67,68,69,70.
Muscle function
In support of our hypothesis, we found an improved skeletal muscle fatigue resistance after 14 days of smoking cessation that was accompanied with a return of the COHb levels to that seen in non-smokers. It therefore does appear that the improved fatigue resistance after smoking cessation was at least to some extent attributable to an improved oxygen delivery, and perhaps also improved mitochondrial function. Indeed, 2 weeks smoking cessation has been shown to improve mitochondrial function in mouse muscle, although in mice this was not accompanied by an improved muscle fatigue resistance26. Nevertheless, our data suggest that even in smokers with only 3% COHb smoking cessation can still enhance muscle fatigue resistance, even when the fatigue resistance was not significantly less than that in non-smokers. Perhaps the enhanced fatigue resistance after smoking cessation is to some extent also attributable to the elevated haemoglobin concentration and haematocrit that enhance the oxygen carrying capacity and oxygen delivery with smoking cessation even above that seen in the non-smokers17,53, similar to that seen after doping with erythropoietin71. In addition, smoking cessation also improves exercise-induced vasodilation72,73. Overall, our data indicate that even smoking cessation for as short a period as 2 weeks can result in measurable improvements in muscle fatigue resistance.
Blood parameters
Another significant observation in our smokers was evidence of low-grade systemic inflammation and oxidative stress. It was therefore particularly interesting to assess the impact of smoking cessation on these parameters. Here we found that most of the abnormal blood parameters were normalised by 14 days of smoking cessation.
The present study showed that both TAS and MDA did not return to normal levels after 14 days of smoking cessation. This may occur later as it has been shown that after 28 days of smoking cessation, TAS was increased and MDA levels reduced back to normal levels74. AGE levels also did not show a significant decrement after 14 days of smoking cessation. The 3-week half-life of AGEs75,76,77 may explain that despite the diminished low-grade systemic inflammation AGEs remained elevated. Therefore, 14 days of smoking cessation might not be long enough to cause a normalisation in TAS, MDA and AGEs to levels similar to that in non-smokers.
Smoking cessation interrupts the exposure to chemicals in cigarette smoke 28 and it is likely that the reduced concentration of smoking-related chemicals in the blood that induce inflammation will result in a reduction in cytokine levels78,79,80. For example, the elevated levels of TNF-α after 20 weeks smoking was back to baseline levels after 8 weeks smoking cessation in the broncho-alveolar lavage fluid of mice33 and similarly 30 days smoking cessation resulted in a significant reduction in TNF-α in humans28. Here we showed that IL-6, IL-10, IL-12p70, IL-4 returned to normal levels and TNF-α was reduced after 14 days of smoking cessation. It has been suggested that the lungs are the primary cause of the low-grade systemic inflammation in patients with chronic obstructive pulmonary disease81. In line with this it has been shown that 2 weeks smoking cessation in mice led to a return in the number of leucocytes in the broncheo-alveolar lavage fluid to normal levels26. Eosinophil numbers remained lower in smokers than non-smokers after 14 days of smoking cessation, which may be secondary to the higher concentration of IL-2 in smokers, even after 14 days of smoking cessation.
Future directions
We showed significant improvements in muscle fatigue resistance and inflammatory status that may well be sufficient to stimulate smokers in their attempts to quit smoking. Future studies are recommended to conduct longer duration of smoking cessation programmes with larger sample size to assess whether also the markers of oxidative stress and circulating AGEs return to normal values. Although it remains to be seen to what extent the effects observed are related to the duration of smoking, in our previous work we have shown that at least the lower fatigue resistance in smokers was not related to the duration of smoking or smoking pack years19.
Conclusion
Even in smokers with normal spirometry there is significant evidence of oxidative stress and systemic inflammation. A short period of smoking cessation of just 2 weeks is enough to improve the inflammatory status to almost back to normal levels and induce an improvement in muscle fatigue resistance. These benefits will undoubtedly stop the progression of detrimental effects of low-grade systemic inflammation and encourage smokers in their attempts to quit smoking.
Data availability
When appropriate and reasonable, anonymised data are available upon request from the corresponding author.
References
Warren, G. W., Alberg, A. J., Kraft, A. S. & Cummings, K. M. The 2014 surgeon General’s report: “the health consequences of smoking–50 Years of progress”: a paradigm shift in cancer care. Cancer 120, 1914–1916 (2014).
Health, U. D. O. & Services, H. A Report of the Surgeon General: How Tobacco Smoke Causes Disease: What It Means to You (Consumer Booklet). Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health (2010).
Office for National Statistics. (Dandy Booksellers Ltd, 2017).
Lifestyles Team, N. D. (ed The Health and Social Care Information Centre) (NHS Digital, part of the Government Statistical Service, England, 2019).
Glantz, S. A., Bero, L. A., Slade, J., Barnes, D. E. & Hanauer, P. The cigarette papers. (Univ of California Press, 1998).
Cerami, C. et al. Tobacco smoke is a source of toxic reactive glycation products. Proc. Natl. Acad. Sci. 94, 13915–13920 (1997).
Harris, J. E. Cigarette smoke components and disease: cigarette smoke is more than a triad of tar, nicotine, and carbon monoxide. Smok. Tobacco Control Monogr. 7, 59–75 (1996).
Aula, F. A. & Qadir, F. A. Effects of cigarette smoking on some immunological and hematological parameters in male smokers in Erbil city. Jordan J. Biol. Sci. 147, 1–8 (2013).
Abdul-Rasheed, O. F. & Al-Rubayee, W. T. Effects of cigarette smoking on lipid peroxidation and antioxidant status in Iraqi men at Baghdad city. Int. J. Basic Appl. Sci. 2, 47 (2013).
Lykkesfeldt, J., Viscovich, M. & Poulsen, H. E. Plasma malondialdehyde is induced by smoking: a study with balanced antioxidant profiles. Br. J. Nutr. 92, 203–206 (2004).
Morrow, J. D. et al. Increase in circulating products of lipid peroxidation (F2-isoprostanes) in smokers—smoking as a cause of oxidative damage. N. Engl. J. Med. 332, 1198–1203 (1995).
Bloomer, R. J. Decreased blood antioxidant capacity and increased lipid peroxidation in young cigarette smokers compared to nonsmokers: impact of dietary intake. Nutr. J. 6, 39 (2007).
Frati, A. C., Iniestra, F. & Ariza, C. R. Acute effect of cigarette smoking on glucose tolerance and other cardiovascular risk factors. Diabetes Care 19, 112–118 (1996).
Syrový, I. & Hodný, Z. Non-enzymatic glycosylation of myosin: effects of diabetes and ageing. Gen. Physiol. Biophys. 11, 301–307 (1992).
Darabseh, M. Z., Selfe, J., Morse, C. I. & Degens, H. Is vaping better than smoking for cardiorespiratory and muscle function?. Multidiscip. Respir. Med. 15, 674 (2020).
Stănescu, D. et al. Airways obstruction, chronic expectoration, and rapid decline of FEV1 in smokers are associated with increased levels of sputum neutrophils. Thorax 51, 267–271 (1996).
Degens, H., Gayan-Ramirez, G. & van Hees, H. W. Smoking-induced skeletal muscle dysfunction. From evidence to mechanisms. Am. J. Respir. Crit. Care Med. 191, 620–625 (2015).
Morse, C. I., Wüst, R. C., Jones, D. A., De Haan, A. & Degens, H. Muscle fatigue resistance during stimulated contractions is reduced in young male smokers. Acta Physiol. 191, 123–129 (2007).
Wüst, R. C. et al. Skeletal muscle properties and fatigue resistance in relation to smoking history. Eur. J. Appl. Physiol. 104, 103 (2008).
Larsson, L., Örlander, J., Ansved, T. & Edström, L. Effects of chronic nicotine exposure on contractile enzyme-histochemical and biochemical properties of fast-and slow-twitch skeletal muscles in the rat. Acta Physiol. Scand. 134, 519–527 (1998).
Prior, B. M., Yang, H. & Terjung, R. L. What makes vessels grow with exercise training?. J. Appl. Physiol. 97, 1119–1128 (2004).
Wüst, R. C., Jaspers, R. T., van der Laarse, W. J. & Degens, H. Skeletal muscle capillarization and oxidative metabolism in healthy smokers. Appl. Physiol. Nutr. Metab. 33, 1240–1245 (2008).
Pojer, R. et al. Carboxyhemoglobin, cotinine, and thiocyanate assay compared for distinguishing smokers from non-smokers. Clin. Chem. 30, 1377–1380 (1984).
Morse, C. I., Pritchard, L., Wüst, R. C., Jones, D. A. & Degens, H. Carbon monoxide inhalation reduces skeletal muscle fatigue resistance. Acta Physiol. 192, 397–401 (2008).
Alonso, J. R., Cardellach, F., López, S., Casademont, J. & Miró, Ò. Carbon monoxide specifically inhibits cytochrome c oxidase of human mitochondrial respiratory chain. Pharmacol. Toxicol. 93, 142–146 (2003).
Ajime, T. T. et al. Two weeks of smoking cessation reverse cigarette smoke-induced skeletal muscle atrophy and mitochondrial dysfunction in mice. Nicotine Tob. Res. 23, 143–151 (2021).
Degens, H., Sanchez Horneros, J. M., Heijdra, Y. F., Dekhuijzen, P. & Hopman, M. T. Skeletal muscle contractility is preserved in COPD patients with normal fat-free mass. Acta Physiol. Scand. 184, 235–242 (2005).
Rodrigues, F. M. M. et al. Nasal and systemic inflammatory profile after short term smoking cessation. Respir. Med. 108, 999–1006 (2014).
Kanner, R. E., Connett, J. E., Williams, D. E., Buist, A. S. & Group, L. H. S. R. Effects of randomized assignment to a smoking cessation intervention and changes in smoking habits on respiratory symptoms in smokers with early chronic obstructive pulmonary disease: the Lung Health Study. Am. J. Med. 106, 410–416 (1999).
Anthonisen, N. Epidemiology and the lung health study. Eur. Respir. Rev. 7, 202–205 (1997).
Faulkner, M. A., Lenz, T. L. & Stading, J. A. Cost-effectiveness of smoking cessation and the implications for COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 1, 279 (2006).
American Thoracic Society. Skeletal muscle dysfunction in chronic obstructive pulmonary disease. A statement of the American Thoracic Society and European Respiratory Society. Am. J. Respir. Crit. Care Med. 159, S1-40 (1999).
Braber, S., Henricks, P. A., Nijkamp, F. P., Kraneveld, A. D. & Folkerts, G. Inflammatory changes in the airways of mice caused by cigarette smoke exposure are only partially reversed after smoking cessation. Respir. Res. 11, 99 (2010).
Kambam, J. R., Chen, L. H. & Hyman, S. A. Effect of short-term smoking halt on carboxyhemoglobin levels and P50 values. Anesth. Analg. 65, 1186–1188 (1986).
Xu, X., Li, B. & Wang, L. Gender difference in smoking effects on adult pulmonary function. Eur. Respir. J. 7, 477–483 (1994).
Wüst, R. C., Morse, C. I., De Haan, A., Jones, D. A. & Degens, H. Sex differences in contractile properties and fatigue resistance of human skeletal muscle. Exp. Physiol. 93, 843–850 (2008).
Hajek, P. & Belcher, M. Improved CO monitors for validating smoking abstinence by expired-air carbon monoxide level. Br. J. Addict. 86, 1029–1030 (1991).
Miller, M. R. et al. Standardisation of spirometry. Eur. Respir. J. 26, 319–338 (2005).
Crapo, R. O., Morris, A. H. & Gardner, R. M. Reference spirometric values using techniques and equipment that meet ATS recommendations. Am. Rev. Respir. Dis. 123, 659–664 (1981).
Larsson, L. & Örlander, J. Skeletal muscle morphology, metabolism and function in smokers and non-smokers. A study on smoking-discordant monozygous twins. Acta Physiol. Scand. 120, 343–352 (1984).
Al-Obaidi, S. M., Anthony, J., Al-Shuwai, N. & Dean, E. Differences in back extensor strength between smokers and nonsmokers with and without low back pain. J. Orthop. Sports Phys. Ther. 34, 254–260 (2004).
Barreiro, E. et al. Cigarette smoke–induced oxidative stress: a role in chronic obstructive pulmonary disease skeletal muscle dysfunction. Am. J. Respir. Crit. Care Med. 182, 477–488 (2010).
Örlander, J. K. & Larsson, L. Skeletal muscle metabolism, morphology and function in sedentary smokers and nonsmokers. Acta Physiol. Scand. 107, 39–46 (1979).
Seymour, J. et al. The prevalence of quadriceps weakness in COPD and the relationship with disease severity. Eur. Respir. J. 36, 81–88 (2010).
Mündel, T. & Jones, D. A. Effect of transdermal nicotine administration on exercise endurance in men. Exp. Physiol. 91, 705–713 (2006).
Narkiewicz, K. et al. Cigarette smoking increases sympathetic outflow in humans. Circulation 98, 528–534 (1998).
Wald, N. J., Idle, M., Boreham, J. & Bailey, A. Carbon monoxide in breath in relation to smoking and carboxyhaemoglobin levels. Thorax 36, 366–369 (1981).
Alsalhen, K. S. & Abdalsalam, R. D. Effect of cigarette smoking on liver functions: a comparative study conducted among smokers and non-smokers male in El-beida City, Libya. Int. Curr. Pharm. J. 3, 291–295 (2014).
Alhemieri, A. A. Effect of cigarette smoking on some heamatological and biochemical factors in blood of men with aging. Basrah J. Sci. 26, 56–67 (2008).
Nordenberg, D., Yip, R. & Binkin, N. J. The effect of cigarette smoking on hemoglobin levels and anemia screening. JAMA 264, 1556–1559 (1990).
Shah, B., Nepal, A., Agrawal, M. & Sinha, A. The effects of cigarette smoking on hemoglobin levels compared between smokers and non-smokers. Sunsari Tech. Coll. J. 1, 42–44 (2012).
Malenica, M. et al. Effect of cigarette smoking on haematological parameters in healthy population. Med. Arch. 71, 132 (2017).
Aitchison, R. & Russell, N. Smoking-a major cause of polycythaemia. J. R. Soc. Med. 81, 89–91 (1988).
Roethig, H. J. et al. Short term effects of reduced exposure to cigarette smoke on white blood cells, platelets and red blood cells in adult cigarette smokers. Regul. Toxicol. Pharmacol. 57, 333–337 (2010).
Tulgar, Y. et al. The effect of smoking on neutrophil/lymphocyte and platelet/lymphocyte ratio and platelet indices: a retrospective study. Eur. Rev. Med. Pharmacol. Sci. 20, 3112–3118 (2016).
Demirjian, L., Abboud, R. T., Li, H. & Duronio, V. Acute effect of cigarette smoke on TNF-α release by macrophages mediated through the erk1/2 pathway. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 1762, 592–597 (2006).
Ouyang, Y. et al. Suppression of human IL-1β, IL-2, IFN-γ, and TNF-α production by cigarette smoke extracts. J. Allergy Clin. Immunol. 106, 280–287 (2000).
Brenner, S. & Miller, J. H. Brenner's Encyclopedia of Genetics. Vol. 7 229 (Elsevier Science, 2014).
Lee, J., Taneja, V. & Vassallo, R. Cigarette smoking and inflammation: cellular and molecular mechanisms. J. Dent. Res. 91, 142–149 (2012).
Mahmood, I. H., Abdullah, K. S. & Othman, S. H. The total antioxidant status in cigarette smoking individuals. Med. J. Basrah Univ. 25, 46–50 (2007).
Vlassara, H. & Palace, M. Diabetes and advanced glycation endproducts. J. Intern. Med. 251, 87–101 (2002).
Moldogazieva, N. T., Mokhosoev, I. M., Mel’nikova, T. I., Porozov, Y. B. & Terentiev, A. A. Oxidative stress and advanced lipoxidation and glycation end products (ALEs and AGEs) in aging and age-related diseases. Oxid. Med. Cell. Longevity 2019 (2019).
Goldin, A., Beckman, J. A., Schmidt, A. M. & Creager, M. A. Advanced glycation end products: sparking the development of diabetic vascular injury. Circulation 114, 597–605 (2006).
Singh, V. P., Bali, A., Singh, N. & Jaggi, A. S. Advanced glycation end products and diabetic complications. Korean J. Physiol. Pharmacol. 18, 1–14 (2014).
Fletcher, C. & Peto, R. The natural history of chronic airflow obstruction. Br. Med. J. 1, 1645–1648 (1977).
Lange, P. et al. Effects of smoking and changes in smoking habits on the decline of FEV1. Eur. Respir. J. 2, 811–816 (1989).
Aparici, M., Fernández González, A. L. & Alegria, E. Respiratory function tests. Differences between smokers and non-smokers. Effects of withdrawal. Rev. Clin. Espanola 192, 169–172 (1993).
Burchfiel, C. M. et al. Effects of smoking and smoking cessation on longitudinal decline in pulmonary function. Am. J. Respir. Crit. Care Med. 151, 1778–1785 (1995).
Buist, A. S., Nagy, J. M. & Sexton, G. J. The effect of smoking cessation on pulmonary function: a 30-month follow-up of two smoking cessation clinics. Am. Rev. Respir. Dis. 120, 953–957 (1979).
Pezzuto, A., Spoto, C., Vincenzi, B. & Tonini, G. Short-term effectiveness of smoking-cessation treatment on respiratory function and CEA level. J. Comp. Effective. Res. 2, 335–343 (2013).
Rasmussen, P. et al. Effects of erythropoietin administration on cerebral metabolism and exercise capacity in men. J. Appl. Physiol. 109, 476–483 (2010).
Celermajer, D. S. et al. Cigarette smoking is associated with dose-related and potentially reversible impairment of endothelium-dependent dilation in healthy young adults. Circulation 88, 2149–2155 (1993).
Johnson, H. M. et al. Effects of smoking and smoking cessation on endothelial function: 1-year outcomes from a randomized clinical trial. J. Am. Coll. Cardiol. 55, 1988–1995 (2010).
Polidori, M. C., Mecocci, P., Stahl, W. & Sies, H. Cigarette smoking cessation increases plasma levels of several antioxidant micronutrients and improves resistance towards oxidative challenge. Br. J. Nutr. 90, 147–150 (2003).
Biemel, K. M., Friedl, D. A. & Lederer, M. O. Identification and quantification of major Maillard cross-links in human serum albumin and lens protein evidence for glucosepane as the dominant compound. J. Biol. Chem. 277, 24907–24915 (2002).
Klöpfer, A., Spanneberg, R. & Glomb, M. A. Formation of arginine modifications in a model system of N α-tert-butoxycarbonyl (Boc)-arginine with methylglyoxal. J. Agric. Food Chem. 59, 394–401 (2011).
Ahmed, N., Argirov, O. K., Minhas, H. S., Cordeiro, C. A. & Thornalley, P. J. Assay of advanced glycation endproducts (AGEs): surveying AGEs by chromatographic assay with derivatization by 6-aminoquinolyl-N-hydroxysuccinimidyl-carbamate and application to N∊-carboxymethyl-lysine-and N∊-(1-carboxyethyl) lysine-modified albumin. Biochem. J. 364, 1–14 (2002).
Mio, T. et al. Cigarette smoke induces interleukin-8 release from human bronchial epithelial cells. Am. J. Respir. Crit. Care Med. 155, 1770–1776 (1997).
McCarty, M. Interleukin-6 as a central mediator of cardiovascular risk associated with chronic inflammation, smoking, diabetes, and visceral obesity: down-regulation with essential fatty acids, ethanol and pentoxifylline. Med. Hypotheses 52, 465–477 (1999).
Helmersson, J., Larsson, A., Vessby, B. & Basu, S. Active smoking and a history of smoking are associated with enhanced prostaglandin F2α, interleukin-6 and F2-isoprostane formation in elderly men. Atherosclerosis 181, 201–207 (2005).
Gan, W. Q., Man, S., Senthilselvan, A. & Sin, D. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax 59, 574–580 (2004).
Acknowledgements
Catrin Austin for help with data collection.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
H.D. and R.W. contributed to the study conception. H.D., R.W. and T.M.W. designed and prepared the study. M.D., T.M.K., G.W. and H.A. conducted experiments. M.D. and H.D. analysed the data. M.D. and H.D. wrote the first draft of the manuscript. All authors commented on previous versions of the manuscript, read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Darabseh, M.Z., Maden-Wilkinson, T.M., Welbourne, G. et al. Fourteen days of smoking cessation improves muscle fatigue resistance and reverses markers of systemic inflammation. Sci Rep 11, 12286 (2021). https://doi.org/10.1038/s41598-021-91510-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-91510-x
This article is cited by
-
A modelling approach to disentangle the factors limiting muscle oxygenation in smokers
European Journal of Applied Physiology (2024)
-
Obesity and tobacco smoking are independently associated with poor patient-reported outcomes in SLE: a cross-sectional study
Rheumatology International (2024)
-
Circulating levels of IL-6 and TGF-β1 in patients with prostate cancer undergoing radiotherapy: associations with acute radiotoxicity and fatigue symptoms
BMC Cancer (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
