
Abstract
The aim was to assess the ability of nasopharyngeal SARS-CoV-2 viral load at first patient’s hospital evaluation to predict unfavorable outcomes. We conducted a prospective cohort study including 321 adult patients with confirmed COVID-19 through RT-PCR in nasopharyngeal swabs. Quantitative Synthetic SARS-CoV-2 RNA cycle threshold values were used to calculate the viral load in log10 copies/mL. Disease severity at the end of follow up was categorized into mild, moderate, and severe. Primary endpoint was a composite of intensive care unit (ICU) admission and/or death (n = 85, 26.4%). Univariable and multivariable logistic regression analyses were performed. Nasopharyngeal SARS-CoV-2 viral load over the second quartile (≥ 7.35 log10 copies/mL, p = 0.003) and second tertile (≥ 8.27 log10 copies/mL, p = 0.01) were associated to unfavorable outcome in the unadjusted logistic regression analysis. However, in the final multivariable analysis, viral load was not independently associated with an unfavorable outcome. Five predictors were independently associated with increased odds of ICU admission and/or death: age ≥ 70 years, SpO2, neutrophils > 7.5 × 103/µL, lactate dehydrogenase ≥ 300 U/L, and C-reactive protein ≥ 100 mg/L. In summary, nasopharyngeal SARS-CoV-2 viral load on admission is generally high in patients with COVID-19, regardless of illness severity, but it cannot be used as an independent predictor of unfavorable clinical outcome.
Similar content being viewed by others

Introduction
The novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), causative agent of coronavirus disease 2019 (COVID-19), has spread worldwide, becoming a pandemic of historic dimensions1. The clinical spectrum of COVID-19 ranges from asymptomatic disease to pneumonia, life-threatening complications, and, ultimately, death2,3. Despite most infected individuals develop solely a mild illness, the mortality rate for severe cases is as high as that caused by other etiologies of severe community-acquired pneumonia4.
For coping with the best clinical attention to COVID-19 patients it is crucial to perform prognosis estimations at the first clinical evaluation, offering personalized attention based on early and easily detectable predictors that support decision making, guide level of care, and optimize the allocation of health resources. Different studies have already addressed this issue, identifying clinical signs and several biomarkers as predictors of unfavorable outcome5,6,7.
In this regard, different studies have addressed the possible association between the viral load in nasopharyngeal (NP) swabs and the clinical outcomes. Some studies have reported that a high number of virus copies in NP swabs, mainly defined as a cycle threshold (Ct) < 25 or < 22 in the real-time polymerase chain reaction (RT-PCR), was an independent risk factor for intubation and/or death8,9,10,11. However, other studies have not found independent association between low Ct values and critical care admission or death12,13. In short, the real impact of initial SARS-CoV-2 viral load in NP swabs on COVID-19 patients’ outcomes is not been fully elucidated, and this issue remains controversial14.
In the present prospective study on adult COVID-19 patients, stratified into mild disease (attended as outpatients) and hospital admitted with moderate or severe disease, we analyzed if the viral load of SARS-CoV-2 in NP swabs was associated with the disease severity, and the ability of NP SARS-CoV-2 viral load at the first hospital evaluation to predict unfavorable outcomes.
Results
Demographics, clinical characteristics, and outcome
The cohort included 321 adult patients, with the first evaluation at the Emergency room. Fifty-six (17.4%) patients had a mild disease and were discharged after the first evaluation, and subsequently attended as outpatients until the end of follow-up; 180 (56.1%) had a moderate course, being hospitalized in general wards, and with full recovery and hospital discharged; and 85 (26.5%) patients were categorized as severe COVID-19 because of required admission to the ICU (32 patients [10.0%]), in-hospital death (40 [12.5%]), or both (13 [4.0%]).
Demographics, symptoms, and signs of the total cohort and the three categories of disease severity are shown in Table 1. In the total cohort, males accounted for 169 (52.6%), median age was 63 (IQR 52–77) years, and 36.8% were ≥ 70 years old. The most common symptoms were fever (73.8%), cough (67.3%), and dyspnea (45.8%). Two hundred twenty-four (69.8%) patients had chest X-ray infiltrates at first hospital evaluation: 16.1% within the mild group, 77.8% in the moderate one, and 88.2% in the severe group (p < 0.001). During the follow-up, 100% of the patients in the moderate and severe groups showed pulmonary infiltrates in the evolutive chest X-ray after hospital admission. Between-group differences regarding baseline laboratory values were also identified and are detailed in Table 2.
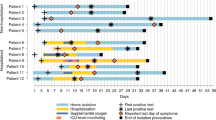
Seventy-eight (24.3%) patients required respiratory support with high flow therapy or non-invasive mechanical ventilation, which was more frequent in patients with severe than with moderate disease (55 [64.7%] vs. 23 [12.8%], respectively, being p = 0.001). Twenty-eight (32.9%) patients, all admitted to ICU, required invasive mechanical ventilation.
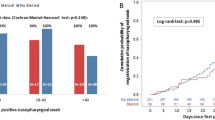
Median NP viral load at first hospital evaluation was not different among the mild, moderate, or severe groups according to their clinical outcomes (Table 2). However, we found higher frequencies of NP viral load above the first tertile, the 50th percentile, and the second tertile in the severe group when comparing the three groups (p = 0.01).
We also analyzed the possible differences among demographics, chronic underlying diseases, and the days from symptoms onset to diagnosis according to the SARS-CoV-2 viral load (Table 3). Although the median days from symptoms onset to diagnosis was lower in the group with higher SARS-CoV-2 viral load (2nd vs. 1st tertile) this difference was not significant. Additionally, we performed a linear regression analysis which did not show association between both variables (p = 0.389). The only significant differences (p < 0.05) were found for the frequency of cardiovascular diseases and age ≥ 70 years. Finally, we made a linear regression analysis between the SARS-CoV-2 viral load and age, finding a significant correlation between both variables (p < 0.001) though not clinically relevant (adjusted R2 0.036).
Predictors of unfavorable outcome
Twenty-three categorical variables at first hospital evaluation were identified as baseline risk factors for unfavorable outcome (admission to ICU or death) in the unadjusted logistic regression analysis: advanced age, arterial hypertension, cardiovascular disease, cancer, dyspnea, higher temperature and respiratory rate, lower diastolic blood pressure and capillary oxygen saturation, leukocytes > 11 × 103/µL, neutrophils > 7.5 × 103/µL, lymphocytes < 1 × 103/µL, and higher levels of creatinine, aspartate aminotransferase, lactate dehydrogenase (LDH), C-reactive protein (CRP), and D-dimer, among others (Table 4). Regarding the NP viral load, values over the second quartile and second tertile were also associated with unfavorable outcome in the unadjusted logistic regression analysis (Table 4).
In the final multivariable analysis, despite the previous link between a higher viral load and the occurrence of unfavorable outcome, the number of virus copies in the NP swabs was not independently associated with an unfavorable clinical result (Table 5). Five of the previous predictors were independently associated with increased odds of ICU admission and/or death: age ≥ 70 years (odds ratio [OR] 3.58, p < 0.001), SpO2 < 95% (OR 11.07, p < 0.001), neutrophils > 7.5 × 103/µL (OR 3.67, p = 0.001), LDH ≥ 300 U/L (OR 2.11, p = 0.04), and CRP ≥ 100 mg/L (OR 2.61, p = 0.01). Information on the overall apparent performance of the model is presented in Table 5 and Fig. 1.

Discrimination power of the final multivariable model: ROC Curve plot. Discrimination power of the model (including Age ≥ 70 years, SpO2 < 95%, neutrophils > 7.5 × 103/µL, LDH ≥ 300 U/L, and CRP ≥ 100 mg/L) expressed by an area under the ROC Curve of 0.89 (95% CI 0.85–0.93), standard error of 0.02 (under the non-parametric assumption), and p < 0.001 (being the null hypothesis a true area = 0.50).
Discussion
The main finding of the present study is that patients with SARS-CoV-2 infection, regardless of their illness severity, generally have a high rate of viral replication in the upper respiratory airways. Consequently, this parameter cannot be used as a predictor of COVID-19 unfavorable outcome, defined as admission to ICU and/or death. Moreover, this prospective cohort confirms that the independent risk factors for ICU admission or death are those previously identified by Salto-Alejandre S. et al7. Thus, at first hospital evaluation, advanced age, hypoxemia, neutrophilia, and increased levels of LDH and CRP have high sensitivity and specificity to accurately discriminate patients that would potentially develop a critical disease from those with a favorable course.
The evidence to date reveals that the relationship between SARS-CoV-2 viral load and the pathogenicity and virulence of this microorganism is not fully understood. Furthermore, as there are many methods to perform the molecular detection of SARS-CoV-2 genome, the interpretation and comparison of results in literature is highly controversial. As an example, droplet digital PCR (ddPCR) has shown slightly higher sensitivity than standard RT-PCR15.
Several previous studies have demonstrated that a high value of SARS-CoV-2 viral load in the upper respiratory tract (URT), defined as a Ct < 25 or < 22 in the RT-PCR, is an independent risk factor for respiratory failure8, intubation, or death9, using multivariate logistic regression and time-based analyses10. Pujadas et al., using a Cox proportional hazards model, also showed an independent association between viral load in the URT and mortality11.
Such results have often led to the thought that viral load could be used along with other features to decide upon the need for hospital admission, and even that a stratification for baseline NP viral load would benefit the design of clinical trials. Nevertheless, other studies show contradictory results. Maltezou et al., using a Ct < 25 to define high URT viral load, reported an association between higher viral load and the development of COVID-19 disease, while no association was found with ICU admission, mechanical ventilation or death12. Amodio et al. demonstrated that the median PCR Ct was significantly lower in patients who died or needed critical care than in those who were hospitalized and discharged alive, or exclusively attended at home, but after adjusting for age and sex, there was not and independent association with critical care need or death13.
Similarly, in our study, despite the patients with higher viral load (above the first tertile, the 50th percentile, and the second tertile) often belonged to the severe disease group, the adjusted multivariable model did not find an association between the copies per mL and the need for critical care or mortality. Argyropoulos et al., on the other hand, showed that viral load was inversely correlated with disease severity, being higher in patients with mild COVID-1916. The reason for this conflictive result was, however, that NP sampling in patients with severe or critical symptoms was obtained at a later time point in the disease course. Lastly, Lee et al. found that viral load quantification was similar among symptomatic and asymptomatic patients17, and our results support this conclusion. Certainly, most patients in the present cohort who suffered an unfavorable outcome had a high SARS-CoV-2 viral load quantification (above the 50th percentile) at hospital admission, but half of the patients with mild COVID-19 also exceeded said limit. This corroborates that the number of virus copies is not strongly related to COVID-19 prognosis.
To further test our hypothesis, we stratified the patients according to disease severity at the end of follow up, and having confirmed that the medium time from symptoms onset to diagnosis was similar among groups, we performed multiple comparations for each viral load cut-off value. Mild patients could only be distinguished through the first tertile, above which a small increment of moderate and severe cases was found. For higher viral load cut-off points, the probability of belonging to the mild or moderate group was similar. The percentage of patients having NP viral load over the 50th percentile and second tertile was significantly higher for those with severe COVID-19, and the univariable analysis showed that a viral load quantification over the mentioned levels could be a risk factor for ICU admission or death. However, through the multivariable model, we concluded that a high viral load could not be used as an independent predictor of such outcomes.
Our study highlights several substantial issues. First, there is not a clear viral load cut-off point capable of discriminating between the various levels of COVID-19 severity, as the ROC Curve analysis demonstrated. Secondly and contrary to expectations, a higher number of SARS-CoV-2 copies in NP swabs at first patient’s evaluation is not predictive of whether ICU admission or death might occur. Nevertheless, according to the Spanish nationwide seroepidemiological study, this finding should not be surprising: a third of the population with positive PCR was asymptomatic, and 20% of the seropositive symptomatic participants did not have previous SARS-CoV-2 genome detection18. Finally, through the external cohort validation of hypoxemia, neutrophilia, and increased levels of LDH and CRP as independent predictors of unfavorable outcome7, we contribute to the identification of higher-risk patients with COVID-19 in whom suitable and prompt management is vital.
The main strength of the present study is that a wide spectrum of COVID-19 severity, from mild symptomatic to critically ill patients, is represented in the analyzed cohort, allowing novel conclusions to be drawn about the efficacy and predictive reliability of previously studied clinical factors. The study has also some limitations. The viral load quantification in the URT samples, through NP swabs, was only performed at a single time point, and we have not data on the dynamics according to the clinical outcomes. Additional synchronous and longitudinal sampling from other sources, such as blood or stools, would have been important comparators. Regarding the quantification of SARS-CoV-2 viral load, further studies are required to refine the use of the standard and novel techniques, which is especially important due to variabilities in specimen collection, the lack of systematic quantification assays, and inconsistencies in protocols between different laboratories. Also, the lack of association of NP viral load with unfavorable outcome, should be confirmed when COVID-19 be caused by the new SARS-CoV-2 variants.
In summary, we found that higher values of SARS-CoV-2 viral load in NP samples at first hospital evaluation are more frequent in patients with unfavorable in-hospital outcome, but that a high viral load is not an independent risk factor for ICU admission or death among adult patients with COVID-19.
Methods
Design, patients, and data collection
We conducted a prospective observational cohort study in Virgen del Rocío University Hospital, a Spanish care-teaching center with 1177 beds (including 72 adult ICU beds). The study protocol was approved by the Ethics Committee of Virgen Macarena and Virgen del Rocío University Hospitals (C.I. 0771-N-20), and complied the Declaration of Helsinki. An informed consent was established as a mandatory requirement for all patients. Consecutive patients with confirmed COVID-19 by RT-PCR assay for SARS-CoV-2 in NP samples were enrolled, from February 29th to May 1st, 2020. Baseline was the date of first hospital evaluation. Follow-up censoring date was May 29th, 2020, for a minimum observation period in each patient of 28 days.
The clinical data source was the electronic medical record system. Variables registered included demographics, comorbidities, symptoms and signs at admission, baseline laboratory tests and chest X-ray findings, complications during hospitalization, and clinical outcome.
SARS-CoV-2 infection diagnosis and viral load
SARS-CoV-2 total RNA was extracted from NP swabs using EZ1 Virus Mini Kit v2.0 (Qiagen Inc., Valencia, CA, USA) following manufacturer’s instruction. SARS-CoV-2 genomic RNA was amplified by LightCycler 96 Instrument (Roche, Germany) using CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel and the GoTaq® Probe 1-Step RT-qPCR System (Wisconsin, USA) following the CDC’s instructions. The Quantitative Synthetic SARS-CoV-2 RNA: ORF, E, N kit (ATCC, VA, USA) for each NP sample was run and Ct values were interpolated into the curve obtained to calculate the viral load in log10 copies/mL. The lower and upper limits of quantification for our RT-PCR were 3.9 and 8.9 log10 copies/mL, respectively.
Statistical analysis
Primary endpoint was the occurrence of unfavorable outcome at the end of follow-up, defined as a composite of ICU admission and/or death. For analyzing the ability of NP SARS-CoV-2 viral load at first patient’s evaluation to predict an unfavorable outcome, the severity of COVID-19 at the end of the 28 days follow-up was categorized into (1) mild, patients exclusively attended as outpatients after the first hospital evaluation; (2) moderate, hospitalized with full recovery and discharged; and (3) severe, hospitalized and admitted to the ICU or dead.
A descriptive analysis of all data obtained was performed. Categorical variables were presented as n (%) and continuous as median (interquartile range [IQR]). We used the χ2-test, Fisher’s Exact Test, One-Way Analysis of Variance (ANOVA), Kruskal Wallis Test, Student’s t-test, or Welch’s t-test to compare between-group differences, and linear regression analysis to assess association between variables, as appropriate.
To examine the factors associated with unfavorable outcome, a univariable logistic regression analysis was performed. Additionally, bivariate correlations were thoroughly explored to account for potential confusion and interaction effects. To increase the applicability of our results within the scope of clinical practice, continuous variables were dichotomized based on normal ranges and cut-off values previously identified as predictors of unfavorable outcome7.
Regarding SARS-CoV-2 viral load, for which there is no prior clinical consensus for categorization, we tried to determine the optimal cut-off value through a ROC curve plot (figure not shown). However, all the points in the curve approached the diagonal segment, with an area underneath of 0.57 (close to the null value) that called into question the usefulness of this parameter. Finally, we decided to analyze viral load based on three prespecified cut-off points: the first tertile, the second quartile or 50th percentile, and the second tertile.
For identifying which of the predictors obtained from the univariable analysis were to be considered independent, a multivariable logistic regression model was built using three criteria to achieve the highest accuracy: relevance to clinical situation, statistical significance (p < 0.10), and adequate number of events to allow meaningful analysis. An automated backward stepwise selection was used for exclusion of variables, utilizing a probability threshold of 5%. The model was first assessed for sensitivity, specificity, positive and negative predictive values, and overall apparent performance. Secondly, the fraction of variance explained by said model was estimated through the Nagelkerke R2 value. The internal validity was finally evaluated using the area under the ROC curve, where ≥ 0.70 (being the null hypothesis a true area of 0.50) is considered as evidence of good discrimination ability.
Ethics approval
The study protocol was approved by the Ethics Committee of Virgen Macarena and Virgen del Rocío University Hospitals (C.I. 0771-N-20) and complied the Declaration of Helsinki.
Data availability
All data generated or analyzed during this study are included in this published article (and its Supplementary Information files).
References
Zhou, P. et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 579, 270–273 (2020).
Guan, W. J. et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 382, 1708–1720 (2020).
Chen, N. et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395, 507–513 (2020).
Sligl, W. I. & Marrie, T. J. Severe community-acquired pneumonia. Crit. Care Clin. 29, 563–601 (2013).
Gong, J. et al. A tool for early prediction of severe coronavirus disease 2019 (COVID-19): a multicenter study using the risk nomogram in wuhan and guangdong, China. Clin. Infect. Dis. 71, 833–840 (2020).
Ji, D. et al. Prediction for progression risk in patients with COVID-19 pneumonia: the CALL score. Clin. Infect. Dis. 71, 1393–1399 (2020).
Salto-Alejandre, S. et al. A quick prediction tool for unfavourable outcome in COVID-19 inpatients: development and internal validation. J. Infect. 82, e11–e15 (2021).
De la Calle, C. et al. Impact of viral load at admission on the development of respiratory failure in hospitalized patients with SARS-CoV-2 infection. Eur. J. Clin. Microbiol. Infect. Dis. https://doi.org/10.1007/s10096-020-04150-w (2021).
Bryan, A. et al. SARS-CoV-2 viral load on admission is associated with 30-day mortality. Open Forum Infect. Dis. 7, ofaa535 (2020).
Magleby, R. et al. Impact of SARS-CoV-2 viral load on risk of intubation and mortality among hospitalized patients with coronavirus disease 2019. Clin. Infect. Dis. https://doi.org/10.1093/cid/ciaa851 (2020).
Pujadas, E. et al. SARS-CoV-2 viral load predicts COVID-19 mortality. Lancet Respir. Med. 8, E70 (2020).
Maltezou, H. C. et al. Association between upper respiratory tract viral load, comorbidities, disease severity and outcome of patients with SARS-CoV-2 infection. J. Infect. Dis. 223, 1132–1138 (2021).
Amodio, E. et al. SARS-CoV-2 viral load, IFNλ polymorphisms and the course of COVID-19: an observational study. J. Clin. Med. 9, 3315 (2020).
Walsh, K. A. et al. SARS-CoV-2 detection, viral load and infectivity over the course of an infection. J. Infect. 81, 357–371 (2020).
Yu, F. et al. Quantitative detection and viral load analysis of SARS-CoV-2 in infected patients. Clin. Infect. Dis. 71, 793–798 (2020).
Argyropoulos, K. V. et al. Association of initial viral load in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) patients with outcome and symptoms. Am. J. Pathol. 190, 1881–1887 (2020).
Lee, S. et al. Clinical course and molecular viral shedding among asymptomatic and symptomatic patients with SARS-CoV-2 infection in a community treatment center in the Republic of Korea. JAMA Intern. Med. 180, 1447–1452 (2020).
Pollán, M. et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. Lancet 396, 535–544 (2020).
Funding
This work was supported by National Plan R+D+I 2013–2016 and Instituto de Salud Carlos III, Subdirección General de Redes y Centros de Investigación Cooperativa, Ministry of Economy, Industry, and Competitiveness, Spanish Network for Research in Infectious Diseases [REIPI RD16/0016/0009]; cofinanced by European Development Regional Fund “A way to achieve Europe”, Operative program Intelligent Growth 2014–2020; and supported by Grants from the Instituto de Salud Carlos III, Ministerio de Ciencia e Innovación, Proyectos de Investigación sobre el SARS-CoV-2 y la enfermedad COVID-19 [COV20/00370; COV20/00580]. J.S.C. is a researcher belonging to the program “Nicolás Monardes” (C-0059-2018), Servicio Andaluz de Salud, Junta de Andalucía, Spain.
Author information
Authors and Affiliations
Consortia
Contributions
J.S.-C., E.C., J.M.C., and J.P. conceived and designed the study; obtained public funding from the Spanish Ministry of Economy, Industry, and Competitiveness; and took responsibility for the integrity of the data and the accuracy of its analysis. J.P., J.B.-C., and S.S.-A. did the scientific literature search. P.C.-M., C.I.-D., M.C.-L., J.C.C.-R., E.M., J.M.L., C.B., R.A., and J.A.L. provided the data. JB-C and SS-A processed the data, did the statistical analysis, and wrote the draft of the manuscript. All authors critically revised the manuscript for important intellectual content and gave final approval for the version published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Salto-Alejandre, S., Berastegui-Cabrera, J., Camacho-Martínez, P. et al. SARS-CoV-2 viral load in nasopharyngeal swabs is not an independent predictor of unfavorable outcome. Sci Rep 11, 12931 (2021). https://doi.org/10.1038/s41598-021-92400-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-92400-y
This article is cited by
-
Bimodal distribution pattern associated with the PCR cycle threshold (Ct) and implications in COVID-19 infections
Scientific Reports (2022)
-
Nasopharyngeal viral load at admission is not an independent predictor of thromboembolic complications in unvaccinated COVID-19 hospitalized patients.
Journal of Thrombosis and Thrombolysis (2022)
-
Identification of Parameters Representative of Immune Dysfunction in Patients with Severe and Fatal COVID-19 Infection: a Systematic Review and Meta-analysis
Clinical Reviews in Allergy & Immunology (2022)
-
Excretion and viability of SARS-CoV-2 in feces and its association with the clinical outcome of COVID-19
Scientific Reports (2022)
-
Plasma SARS-CoV-2 nucleocapsid antigen levels are associated with progression to severe disease in hospitalized COVID-19
Critical Care (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
