
Abstract
The aim of this study was to cross-sectionally explore the association of obesity with spinal posture and mobility, commonly associated with musculoskeletal problems, by comparing the spinal parameters between 90 obese and 109 normal-weight children and adolescents. A non-invasive electromechanical device, the Idiag M360 (Idiag, Fehraltorf, Switzerland), was used to measure the spinal parameters. An age-and-sex-adjusted two-way analysis of variance (ANOVA) was used to determine postural and mobility differences between the two groups. Children and adolescents with obesity had significantly greater thoracic kyphosis [difference between groups (Δ) = 13.00, 95% CI 10.10–15.80, p < 0.0001] and thoracic extension (Δ = 6.50, 95% CI 2.90–11.60, p = 0.005), as well as smaller mobility in thoracic flexion (Δ = 5.00, 95% CI 1.20–8.80, p = 0.01), thoracic lateral flexion (Δ = 17.70, 95% CI 11.60–23.80, p < 0.0001), lumbar flexion (Δ = 12.10, 95% CI 8.70–15.50, p < 0.0001), lumbar extension (Δ = 7.10, 95% CI 3.10–12.20, p = 0.003) and lumbar lateral flexion (Δ = 9.10, 95% CI 5.50–12.80, p < 0.0001) compared to the normal-weight children and adolescents. These findings provide important information about the characteristics of the spine in children and adolescents with obesity and unique insights into obesity-related mechanical challenges that the spine has to withstand and strategies designed to improve spinal mobility in this young population.
Similar content being viewed by others

Introduction
The prevalence of obesity among children and adolescents has been increasing across worldwide populations, causing both psychological and physical consequences1,2. Between 1975 and 2016, the global prevalence of obesity increased eight-fold in children and adolescents3. Obesity can negatively affect various body systems and lead to an increased risk of numerous health conditions, including musculoskeletal conditions, cardiovascular diseases, metabolic syndrome and gastrointestinal and pulmonary conditions2. Exercise, motion, diet and behavioural changes still play a crucial role in the management of obesity and obesity-related conditions in paediatric practice compared to medications2,4,5. Physical inactivity, reduced body motion and sedentary lifestyle contributing to obesity2 are also considered to be modifiable risk factors for common musculoskeletal conditions, such as knee osteoarthritis and low back pain6,7,8.
Obesity appears to alter spinal postures and movement in adult populations9,10,11. Spinal posture and flexibility commonly examined in clinical practice as part of a musculoskeletal assessment, are reported to play an important role in the performance of daily activities, as well as many occupational and recreational tasks. Additionally, alterations in spinal movement are often associated with low back pain12,13. Obesity is not only associated with low back pain, which is one of the most common musculoskeletal conditions but it also increases the risk of low back pain14. Low back pain is a common problem in school-aged children as well. A subsequent increase in the prevalence of low back pain in children becomes similar to the rates of low back pain in adult populations when they reach 18 years of age1. Low back pain is multifactorial and the biophysical aspect is considered one of the factors that substantially contribute to it15. For example, alterations in spine mobility may increase abnormal loading that leads to tissue degeneration, potentially resulting in pain and other clinical symptoms16. Importantly, prospective studies have shown that restriction in the lumbar range of motion in the frontal plane as well as reduced lumbar lordosis has been found to increase the risk of developing low back pain17, emphasizing the importance of preserving spinal flexibility and normal spinal curvature. However, obese adults have been found to have smaller lumbar flexion and lumbopelvic ratios in the frontal and horizontal plane than normal-weight people9. Nevertheless, it remains unclear whether spinal mobility is affected by obesity in children and adolescents, as studies to date that have examined this association between obesity in children, as well as adolescents and spinal mobility are lacking. Therefore, investigating this association in children and adolescents may help to better understand the spinal flexibility of children and adolescents with obesity and provide unique insights into the management of reduced spinal flexibility among this young population.
The aim of this study was to explore the association of obesity with spinal postures as well as spinal and hip mobility in children and adolescents and compare the parameters to those of the same age group with normal weight.
Methods
The present study employed a cross-sectional design to explore the association of obesity with spinal posture as well as mobility and followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Participants
Obese and normal-weight children and adolescents as defined by the World Health Organization guidelines were recruited, with an age range between 6 and 18 years18. Participants suffering from past and present orthopaedic or neurological conditions, including limb length discrepancy, spina bifida, spinal deformities and surgeries determining physical disabilities and those taking anti-inflammatory drugs, were excluded from the study.
Normal-weight participants were recruited from elementary schools and sports clubs in the Canton of Zurich, Switzerland. Participants with obesity were recruited at the Division of Auxology, Istituto Auxologico Italiano, IRCCS, Piancavallo (VB), Italy, where they were hospitalized for a three-week multidisciplinary body weight reduction program. The study was approved by the Ethics Committee of the Istituto Auxologico Italiano (Milan, Italy; research project code: 01C124; acronym: PRORIPONATFIS) and the Ethics Committee of Zurich (BASEC-no. 2018-00979) and was in accordance with the Helsinki Declaration of 1975, as revised in 2008. The purpose and objective of the study were explained to each subject and his/her parents and written informed consent was obtained. The recruitment periods were between 26 October 2018 and 11 December 2019 for normal-weight children and adolescents and between 24 July 2020 and 21 April 2021 for children and adolescents with obesity.
Measurements
Spinal and hip mobility
For children and adolescents with obesity, the measurements were performed on the 2nd–3rd day of hospitalization, between 8 and 10 a.m., at a comfortable ambient temperature (about 20 °C), by the same well-trained operator. The same condition of measurement (i.e. time, ambient) was adopted for the control group.
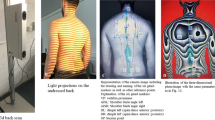
Spinal posture, as well as spinal and hip mobility, were measured using the Idiag M360 scan tool (Idiag, Fehraltorf, Switzerland)19. The Idiag M360, a non-invasive, radiation-free, reliable, computer-aided skin-surface device is designed to quantify the spinal posture and mobility through computer-assisted analysis and records angles of each vertebral joint and sacral inclination in the sagittal and frontal plane. Vertebral distances, positions of the vertebral bodies and the sacrum, the angles between them, as well as the mobility of each individual spinal segment are calculated during the recording. The device consists of two rolling wheels that measure vertebral distances and angles whilst they follow the vertebral spinous processes. The parameters measured by the rolling wheels are transferred radiographically by an analogue–digital converter to a personal computer. As the rolling wheels follow the spinous processes, data are sampled every 1.3 mm at a frequency of 150 Hz20,21,22. The validity of measuring segmental and global lumbar mobility using the Idiag M360 was determined in comparison with an X-ray examination, which, however, remains the gold standard for assessing spinal deformities23,24,25. Thoracic, lumbar and hip movement were measured in the sagittal and frontal plane when participants were asked to bend forward as far as they can into flexion followed by extension and lateral flexion from an upright standing position. Variables of interest for spinal mobility were thoracic and lumbar flexion, extension and lateral flexion, as well as hip flexion and extension. Spinal posture and mobility were measured once according to the protocol, also containing pictures illustrating the measurement procedures, provided by previous studies20,21. Furthermore, both operators who measured the spinal parameters in the normal-weight and obese participants had been adequately trained by the Idiag staff with the support of educational videos.
Reliability of the device
To ensure the reliability of the device in obese patients, a pilot test was conducted that included two repeated measurements of the same subject in ten adolescents with obesity. The standard error of measurement (SEM) of the spinal parameters measured in the present study was computed as SD·√(1 − ICC), where SD and ICC are the standard deviation and intraclass correlation coefficient of each spinal posture or mobility. We estimated the intrarater ICCs for the spinal postures, ranging from 0.86 to 0.94 and the SEM values ranged from 0.580 to 0.700. The intrarater ICCs for spinal mobility in the sagittal and frontal plane ranged from 0.87 to 0.98 and 0.57–0.80, respectively. The SEM values ranged from 0.290 to 1.450 for the sagittal plane measurements and 3.40–3.50 for the frontal plane measurements.
As far as the reliability of the device for spinal posture and mobility measurements in normal-weight children and adolescents is concerned, fair to high reliability was previously demonstrated21. The intrarater and interrater ICCs ranged from 0.61 to 0.96 and 0.70–0.93, respectively, while the SEM values ranged from 0.610 to 13.18021.
Data processing
Each range of motion value for the variables of interest was determined by the difference between the range of motion values measured at the standing position and the end of motion ranges in the anatomical planes. The device measures the range of motion in each segment of the spine, i.e. five motion values for the lumbar spine and twelve for the thoracic spine. The total range of motion of the lumbar and thoracic spine was determined by the sum of the respective range of motion values. Hip range of motion was determined by the sacral inclination relative to the frontal plane.
Statistical analysis
Descriptive statistics and inferential analyses were performed using the R version 3.6.026. In descriptive statistics, mean values and standard deviations (SD) for participant characteristics, including age, sex, posture and mobility of the hip, thoracic and lumbar spine, as well as lumbar-hip ratio were determined. The Shapiro–Wilk test was used to check for data normality. The independent samples t-test for normally distributed data and the Wilcoxon’s test for non-normally distributed parameters were employed to compare demographic and anthropometric characteristics between the two groups (normal-weight and obese). The chi-square test was used for categorical variables. Age and sex-adjusted two-way analysis of variance (ANOVA) was performed for determining statistically significant postural and mobility differences between the normal-weight and obese groups. Pairwise post hoc tests were performed following the ANOVA tests using the software package “emmeans”27. A p-value of less than 0.05 was considered statistically significant.
Results
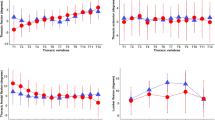
A total of 109 children and adolescents with obesity and 90 normal-weight age-matched individuals were recruited for the study. The main demographic and anthropometric characteristics of the participants are presented in Table 1. The average age, height and sex ratio were not different between the two groups (p > 0.05). Segmental posture and mobility of the spine in the normal-weight and obese groups are presented in Fig. 1.

Posture and mobility of each individual spinal segment in the normal-weight and obese groups (mean ± standard deviations). Normal normal-weight group, Obese obese group.
Association between obesity and spinal postures as well as the mobility of the spine and hip
The age- and sex-adjusted ANOVA test showed statistically significant differences in thoracic kyphosis and lumbar, thoracic and hip range of motion between the two groups (Table 2). Thoracic kyphosis was larger in the obese group than in the normal-weight group, whereas no statistically significant differences between the groups were found in the other spinal postures. The lumbar, thoracic and hip range of motion measured in the two anatomical planes was larger in the normal-weight group than in the obese group except for the thoracic extension. In the post hoc test, the largest differences observed in spinal and hip mobility between the two groups were in thoracic lateral flexion, followed by hip extension, which was 17.70 and 14.80, respectively, larger in the normal-weight group than in the group of obese children and adolescents (Table 2). The remaining lumbar and hip range of motion values were also larger in the normal-weight individuals compared to the obese individuals, except for the thoracic extension, which was 6.50 larger in the obese participants. The lumbar-hip ratio was not different between the two groups, but a statistically significant difference was observed between the male and female individuals. The lumbar-hip ratio was smaller in the female participants than in the male subjects (p < 0.0001).
Discussion
The purpose of the current study was to examine the association of obesity with spinal posture and mobility in children and adolescents, with the key finding being that obesity is associated with alterations in spinal and hip mobility, as well as some spinal postures. Obesity in children and adolescents was associated with increased thoracic kyphosis and thoracic extension but decreased mobility in thoracic flexion and lateral flexion, lumbar flexion, extension and lateral flexion and hip flexion and extension. Obesity appears to have an influence on increased thoracic kyphosis, which in turn may require increased thoracic extension but no effect on lumbar and sacral postures.
Obesity was associated with increased thoracic kyphosis, but no significant association was observed with lumbar and sacral postures. Although studies determining thoracic kyphosis in children and adolescents with obesity using a skin-surface device are lacking, the average kyphosis in the normal-weight participants determined at 350 in the current study was similar to estimates for thoracic kyphosis defined by a previous study involving subjects with a mean age of 10.6 years21. The results from the current study are also consistent with previous study findings in relation to the association between obesity and thoracic kyphosis. A retrospective comparative cohort study of 70 nonscoliotic adolescents and 1551 adolescent idiopathic scoliosis patients that explored the relationship between BMI (body mass index) and thoracic kyphosis, found that an increased BMI was associated with increased thoracic kyphosis in both individuals with and without spinal deformities28. The authors suggested that excess weight may hinder anterior vertebral growth by increasing compressive load on the growth plates of the vertebrae, potentially resulting in increased kyphosis. Additionally, they highlighted that this association needs to be taken into consideration when correcting sagittal plane deformities. In the current study, the thoracic spine was further examined segmentally (proximal T1_6 and distal T7_12) in relation to obesity. An increase in proximal thoracic kyphosis was associated with obesity, whereas no significant association was observed with distal thoracic kyphosis, thus suggesting that obesity may contribute more to alterations in the sagittal posture of the upper thoracic spine (T1_6) than the lower thoracic spine. Increased thoracic kyphosis appears to be correlated with some musculoskeletal conditions. For example, a previous case–control study found that increased thoracic kyphosis was associated with the shoulder impingement syndrome29, implying the importance of taking into account thoracic kyphosis in the management of the shoulder impingement syndrome. Additionally, extensive knowledge of thoracic posture and mobility is crucial for an effective strategy in the management and prevention of thoracic disorders, as well as the evaluation of rehabilitation outcomes11. A previous systematic review exploring the shape and mobility of the thoracic spine in asymptomatic individuals found that thoracic kyphosis increased with ageing, an increase of approximately 3 degrees per decade11, implying that alterations in thoracic kyphosis tend to increase over time. Thoracic kyphosis also appears to change between sitting and standing positions30,31. For example, a comparative study of 58 individuals with a mean age of 23 years found that thoracic kyphosis decreased from standing to sitting due to the forward displacement of the sagittal vertical axis, likely as a result of the change in the centre of gravity30. The results from the current study provide important information about the characteristics of the thoracic spine in obese children and adolescents and unique insights into obesity-related mechanical challenges such as excess weight in the anterior part of the trunk that the thoracic spine must withstand. These findings also imply the importance of taking obesity into account when assessing thoracic kyphosis and when treating or correcting thoracic kyphosis in this paediatric population.
Lumbar and sacral postures were not different between obese and normal-weight children and adolescents in the current study. The result was in line with previous cross-sectional studies that analysed the influence of the BMI on lumbar and pelvic postures determined by using X-rays32,33. A cross-sectional study of 200 adult participants categorized into normal-weight, overweight and obese groups that investigated the relationship between obesity and spinopelvic parameters, including lumbar lordosis, pelvic tilt and sacral slope, showed no statistically significant differences in the parameters across the three different BMI groups33. Another cross-sectional study of 89 elderly females analysing the influence of the BMI on lumbar and pelvic postures found that lumbopelvic postures appear to be unaffected by the BMI32, suggesting that the BMI may not influence lumbopelvic postures, regardless of age. The findings of the current study also suggest that obesity appears to contribute less to alterations in lumbopelvic postures than thoracic kyphosis. However, studies that explore the association between obesity and lumbopelvic postures in children and adolescents are lacking, suggesting that more research is needed to confirm the findings from the current study.
All the spinal movement measured in the sagittal and frontal plane were significantly different between obese and normal-weight children and adolescents. Alterations in spinal mobility are often associated with musculoskeletal conditions, particularly low back pain12,13. Regarding the thoracic spine, it was found that thoracic flexion and lateral flexion were lower in obese patients than in normal-weight individuals, suggesting that obesity may contribute to reduced thoracic flexibility in this paediatric population. Although studies analysing the association between obesity and spinal mobility in children and adolescents are lacking, the previous systematic review that included 45 studies of adult populations showed that obesity was associated with reduced thoracic movement11, which was consistent with the findings from the current study. However, the thoracic extension was larger in obese children and adolescents than in normal-weight individuals, which could potentially be specific to this age group. This could also be explained by increased thoracic kyphosis found in obese individuals, which in turn may require an increased thoracic extension. Thus, the different thoracic positions in standing (mid position) between the normal-weight and obese groups may explain the range of motion differences in the sagittal plane. These range of motion differences may not be related to their flexibility but rather to the different thoracic positions in standing. These results may have important implications regarding the assessment of thoracic movement and strategies aiming to improve thoracic mobility in children and adolescents.
Lumbar flexion, extension and lateral flexion were found to be smaller in obese patients than in normal-weight individuals. Studies examining the relationship between obesity and lumbar mobility in adolescent children are also lacking to date. Nevertheless, several studies have examined this association in adult populations. The reduced lumbar flexion observed in the obese population in the current study was in line with a previous cross-sectional study of 18 obese and normal-weight adults comparing lumbar movement measured by using a Vicon motion capture system9. Another cross-sectional study that compared lumbar mobility determined by using a back range of motion instrument, the BROM II, between 20 obese and 20 non-obese males, found no effect of obesity on lumbar flexion, showing some inconsistencies with the association between obesity and reduced lumbar flexion in adult populations34. Nevertheless, this study found that obesity was associated with reduced lumbar extension and lateral flexion, which was consistent with our findings. Reduced lumbar movement associated with obesity appear to be explained by excess adipose tissues obstructing vertebral intersegmental mobility34. Additionally, reduced lumbar mobility is often associated with low back pain12,13. For example, a meta-analysis of prospective studies showed that a restriction in the lumbar range of motion in the frontal plane increases the risk of developing low back pain17. Overall, the findings suggested that obesity appears to contribute to reduced lumbar mobility in the sagittal and frontal plane, which may be taken into account when developing strategies designed to prevent a reduction in lumbar mobility-associated obesity and promote lumbar flexibility in this paediatric population.
Obesity was found to be associated with reduced hip flexion and extension, whereas no associations were observed with the lumbar–hip ratio. Hip flexion and extension were approximately 10.5 (6.3–14.6) and 14.8 (10.6–19.0) degrees smaller in the obese subjects, respectively, suggesting that obesity may contribute more to a reduction in hip extension than to a hip flexion range of motion. Although hip flexion was found to be smaller in obese children and adolescents, no statistically significant differences were observed in the lumbar-hip ratio between the obese and normal-weight populations. This may be explained by a decrease in both the lumbar and hip flexion range of motion, as the lumbar-hip ratio was determined by the proportion of these two parameters. However, a statistically significant difference in the lumbar-hip ratio was observed between the male and female individuals, implying that gender potentially influences the lumbar-hip ratio more than obesity. These findings highlight that obesity may contribute more to alterations in the hip range of motion, particularly hip extension, than the lumbar-hip ratio in children and adolescents.
The main limitation of the current study is the cross-sectional design, which cannot provide evidence on whether the nature of the association between obesity and alterations in spinal and hip mobility is causal. The current study examines spinal posture and the mobility of the spine and hip only in children and adolescents, thus hampering a generalization of the results to people outside this age range. Spinal mobility, particularly lumbar extension, in individuals with obesity, could be underestimated due to a greater percentage of soft tissue, as we used a skin surface device in the current study. Spinal mobility (range of motion) was determined by the change in angles between the static positions defining the starting point and the end of the spinal range of motion, suggesting that the range of motion values estimated in the current study could not be generalized to a dynamic range or motion or dynamic flexibility. Spinal parameter differences found in the current study between normal-weight participants recruited in elementary schools and sports clubs and the hospitalized children and adolescents with obesity may not be generalized to comparisons of these parameters between normal-weight children and adolescents who do not engage in sports activities and non-hospitalized children and adolescents with obesity.
In conclusion, alterations in spinal postures, as well as spinal and hip mobility, were associated with obesity in children and adolescents. Obesity was associated with increased thoracic kyphosis and thoracic extension but reduced spinal and hip mobility, including thoracic flexion and lateral flexion, lumbar flexion, extension and lateral flexion, as well as hip flexion and extension except for the thoracic extension. Obesity appears to contribute to increased thoracic kyphosis, which in turn may require increased thoracic extension but has no effect on lumbar and sacral postures or the hip-to-lumbar ratio. These findings provide important information about the characteristics of the spine in obese children and adolescents and unique insights into obesity-related mechanical challenges that the spine has to withstand. These results also imply the importance of taking into account obesity in the assessment of spinal postures, as well as strategies designed to improve spinal and hip mobility in children and adolescents.
Data availability
The data presented in this study are available from the corresponding author upon reasonable request.
References
MacDonald, J., Stuart, E. & Rodenberg, R. Musculoskeletal low back pain in school-aged children: A review. JAMA Pediatr. 171, 280–287. https://doi.org/10.1001/jamapediatrics.2016.3334 (2017).
Güngör, N. K. Overweight and obesity in children and adolescents. J. Clin. Res. Pediatr. Endocrinol. 6, 129–143. https://doi.org/10.4274/Jcrpe.1471 (2014).
Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 390, 2627–2642. https://doi.org/10.1016/s0140-6736(17)32129-3 (2017).
Fock, K. M. & Khoo, J. Diet and exercise in the management of obesity and overweight. J. Gastroenterol. Hepatol. 28(Suppl 4), 59–63. https://doi.org/10.1111/jgh.12407 (2013).
Kumar, S. & Kelly, A. S. Review of childhood obesity: From epidemiology, etiology, and comorbidities to clinical assessment and treatment. Mayo Clin. Proc. 92, 251–265. https://doi.org/10.1016/j.mayocp.2016.09.017 (2017).
White, D. K. et al. Daily walking and the risk of incident functional limitation in knee osteoarthritis: An observational study. Arthritis Care Res. (Hoboken) 66, 1328–1336. https://doi.org/10.1002/acr.22362 (2014).
Iijima, H. et al. Relationship between pedometer-based physical activity and physical function in patients with osteoarthritis of the knee: A cross-sectional study. Arch. Phys. Med. Rehabil. 98, 1382-1388.e1384. https://doi.org/10.1016/j.apmr.2016.12.021 (2017).
Alzahrani, H., Mackey, M., Stamatakis, E., Zadro, J. R. & Shirley, D. The association between physical activity and low back pain: A systematic review and meta-analysis of observational studies. Sci. Rep. 9, 8244. https://doi.org/10.1038/s41598-019-44664-8 (2019).
Ghasemi, M. & Arjmand, N. Spinal segment ranges of motion, movement coordination, and three-dimensional kinematics during occupational activities in normal-weight and obese individuals. J. Biomech. 123, 110539. https://doi.org/10.1016/j.jbiomech.2021.110539 (2021).
Vismara, L. et al. Effect of obesity and low back pain on spinal mobility: A cross-sectional study in women. J. Neuroeng. Rehabil. 7, 3. https://doi.org/10.1186/1743-0003-7-3 (2010).
Pan, F., Firouzabadi, A., Reitmaier, S., Zander, T. & Schmidt, H. The shape and mobility of the thoracic spine in asymptomatic adults—A systematic review of in vivo studies. J. Biomech. 78, 21–35. https://doi.org/10.1016/j.jbiomech.2018.07.041 (2018).
Scholtes, S. A., Gombatto, S. P. & Van Dillen, L. R. Differences in lumbopelvic motion between people with and people without low back pain during two lower limb movement tests. Clin. Biomech. (Bristol, Avon) 24, 7–12. https://doi.org/10.1016/j.clinbiomech.2008.09.008 (2009).
Zhou, J., Ning, X. & Fathallah, F. Differences in lumbopelvic rhythm between trunk flexion and extension. Clin. Biomech. (Bristol, Avon) 32, 274–279. https://doi.org/10.1016/j.clinbiomech.2015.10.012 (2016).
Shiri, R., Karppinen, J., Leino-Arjas, P., Solovieva, S. & Viikari-Juntura, E. The association between obesity and low back pain: A meta-analysis. Am. J. Epidemiol. 171, 135–154. https://doi.org/10.1093/aje/kwp356 (2010).
Hartvigsen, J. et al. What low back pain is and why we need to pay attention. Lancet 391, 2356–2367. https://doi.org/10.1016/s0140-6736(18)30480-x (2018).
Iorio, J. A., Jakoi, A. M. & Singla, A. Biomechanics of degenerative spinal disorders. Asian Spine J. 10, 377–384. https://doi.org/10.4184/asj.2016.10.2.377 (2016).
Sadler, S. G., Spink, M. J., Ho, A., De Jonge, X. J. & Chuter, V. H. Restriction in lateral bending range of motion, lumbar lordosis, and hamstring flexibility predicts the development of low back pain: A systematic review of prospective cohort studies. BMC Musculoskelet. Disord. 18, 179–179. https://doi.org/10.1186/s12891-017-1534-0 (2017).
World Health Organization. Growth reference data for 5–19 years. https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age (2007). Accessed 15 January 2022.
Idiag. Idiag M360. https://www.idiag.ch/en/idiag-m360-en/ (2021). Accessed 15 January 2022.
Livanelioglu, A., Kaya, F., Nabiyev, V., Demirkiran, G. & Fırat, T. The validity and reliability of “Spinal Mouse“ assessment of spinal curvatures in the frontal plane in paediatric adolescent idiopathic thoraco-lumbar curves. Eur. Spine J. 25, 476–482. https://doi.org/10.1007/s00586-015-3945-7 (2016).
Kellis, E., Adamou, G., Tzilios, G. & Emmanouilidou, M. Reliability of spinal range of motion in healthy boys using a skin-surface device. J. Manipulative Physiol. Ther. 31, 570–576. https://doi.org/10.1016/j.jmpt.2008.09.001 (2008).
Mannion, A. F., Knecht, K., Balaban, G., Dvorak, J. & Grob, D. A new skin-surface device for measuring the curvature and global and segmental ranges of motion of the spine: Reliability of measurements and comparison with data reviewed from the literature. Eur. Spine J. 13, 122–136. https://doi.org/10.1007/s00586-003-0618-8 (2004).
Nouh, M. R. Imaging of the spine: Where do we stand?. World J. Radiol. 11, 55–61. https://doi.org/10.4329/wjr.v11.i4.55 (2019).
Raso, V. J. et al. Trunk distortion in adolescent idiopathic scoliosis. J. Pediatr. Orthop. 18, 222–226 (1998).
Guermazi, M. et al. Validity and reliability of Spinal Mouse to assess lumbar flexion. Ann. Readapt. Med. Phys. 49, 172–177. https://doi.org/10.1016/j.annrmp.2006.03.001 (2006).
R Core Team. R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, 2019).
Lenth R. emmeans: Estimated Marginal Means, aka Least-Squares Means. R package version 1.6.3. (2021).
Valdovino, A. G. et al. Obesity is associated with increased thoracic kyphosis in adolescent idiopathic scoliosis patients and nonscoliotic adolescents. Spine Deform. 7, 865–869. https://doi.org/10.1016/j.jspd.2019.03.010 (2019).
Hunter, D. J., Rivett, D. A., McKeirnan, S., Smith, L. & Snodgrass, S. J. Relationship between shoulder impingement syndrome and thoracic posture. Phys. Ther. 100, 677–686. https://doi.org/10.1093/ptj/pzz182 (2020).
Hey, H. W. D. et al. How the spine differs in standing and in sitting—Important considerations for correction of spinal deformity. Spine J. 17, 799–806. https://doi.org/10.1016/j.spinee.2016.03.056 (2017).
Tsagkaris, C. et al. The sitting vs standing spine. N. Am. Spine Soc. J. (NASSJ). 9, 100108. https://doi.org/10.1016/j.xnsj.2022.100108 (2022).
Canbek, U. et al. The effect of age, BMI, and bone mineral density on the various lumbar vertebral measurements in females. Surg. Radiol. Anat. 43, 101–108. https://doi.org/10.1007/s00276-020-02560-1 (2021).
Romero-Vargas, S. et al. The impact of body mass index and central obesity on the spino-pelvic parameters: A correlation study. Eur. Spine J. 22, 878–882. https://doi.org/10.1007/s00586-012-2560-0 (2013).
Park, W., Ramachandran, J., Weisman, P. & Jung, E. S. Obesity effect on male active joint range of motion. Ergonomics 53, 102–108. https://doi.org/10.1080/00140130903311617 (2010).
Acknowledgements
We are grateful to the children and adolescents (and their parents) participating in the present study, the nursing staff at the Division of Auxology, Istituto Auxologico Italiano, IRCCS, Piancavallo (VB) and participants and their parents in Switzerland as well as Idiag AG, for their qualified assistance during the execution of the functional tests.
Funding
This research is funded by the Italian Ministry of Health.
Author information
Authors and Affiliations
Contributions
Conceptualization: A.S., C.E.S.; data acquisition: C.E.S., R.D.M., G.T.; formal analysis: M.E.B.; funding acquisition: A.S.; investigation: R.D.M., G.T., C.E.S.; supervision, A.S., H.L.; writing original draft: M.E.B.; writing, review and editing: A.S., H. L, M.E.B., C.E.S. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bayartai, M.E., Schaer, C.E., Luomajoki, H. et al. Differences in spinal posture and mobility between children/adolescents with obesity and age-matched normal-weight individuals. Sci Rep 12, 15570 (2022). https://doi.org/10.1038/s41598-022-19823-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-19823-z
This article is cited by
-
Differences in spinal posture and mobility between adults with obesity and normal weight individuals
Scientific Reports (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
