
Key Points
-
Explores some of the most relevant questions faced by dental practitioners when diagnosing early erosive tooth wear (ETW) and implementing non-operative management of this condition over time.
-
Early diagnosis and risk assessment should be implemented at younger ages
-
The non-operative management strategies arrest and/or reduce the rate of ETW progression and avoid its advance to pathological stages.
Abstract
This paper explores some of the most relevant questions faced by dental practitioners when diagnosing early erosive tooth wear (ETW) and implementing non-operative management of this condition over time. It focuses on the identification of clinical signs and common locations of ETW lesions, the assessment of individual risk and the implementation of non-operative management strategies, aiming to arrest and/or reduce the rate of ETW progression and avoid its advance to pathological stages. To this end, we present a novel and comprehensive approach that considers the whole dentition of patients rather than individual groups of teeth or dental surfaces only, illustrating it with a series of clinical photographs. Dental practitioners may find this approach particularly helpful as it closely simulates the clinical examinations of patients of all age groups carried out in daily practice. The clinical signs of early ETW lesions are subtle and often not perceived as relevant by unaware clinicians. However, the early diagnosis and implementation of non-operative management strategies, especially at younger ages, is fundamental for the proper control of ETW over time.
Similar content being viewed by others

Introduction
The early diagnosis of erosive tooth wear (ETW) lesions is a fundamental clinical procedure that allows dentists to implement necessary management strategies to either control or arrest the progression of this condition. Ideally, dentists should have competences and tools to estimate the likelihood of a patient to develop new clinically identifiable ETW lesions as well as the progress of existing ones, within a certain period. Unfortunately, no accurate chair-side tests are available to detect and predict ETW lesions.1 Therefore, a thorough anamnesis and a comprehensive clinical examination must form the basis for erosion diagnosis, risk assessment and treatment decisions in daily practice.
During the anamnesis, the dental practitioner gains insight into the patient's intake of medications, oral hygiene habits, use of oral health care products, occupation, lifestyle and the reason for the visit. It is of utmost importance to listen to what patients tell when explaining the reason for the visit and the description of any possible signs or symptoms. For example, if patients complain about 'sensitive teeth' when drinking cold water or brushing teeth, ETW should be considered along with other conditions associated with tooth hypersensitivity. Another frequent ETW-related complaint is the shortening of maxillary incisors and the yellowish appearance of the teeth, which represent more advanced stages of the process.2
From a clinical perspective, it is important to bear in mind that a certain degree of tooth wear occurs with ageing and it may be considered as physiological in contrast to the pathological condition characterised by signs of ETW lesions, even in its early stages of development. Bearing in mind that age is a determinant factor for erosion, clinical examination for diagnosis of ETW lesions is indicated for patients of all age groups, that is, children, adolescents, young adults and adults. So, what should a dentist look for when examining patients for erosion? Where in the dentition are the early signs of ETW lesions? How do more severe ETW lesions manifest themselves? Which steps should be taken to control, treat and monitor the erosion process over time?
The present paper deals with these relevant questions for dental practitioners in their daily practice. It describes the clinical features of the dental erosive process, illustrating them with clinical cases of ETW, ranging from early to more severe forms in the deciduous and/or permanent dentitions of children, adolescents and young adults. It introduces a comprehensive and useful approach for the diagnosis of the ETW process in early and subsequent stages of progression, by illustrating the condition in the whole dentition of patients rather than in individual groups of teeth or dental surfaces only. Dental practitioners may find this approach particularly helpful in the diagnosis and management of early clinical signs of erosion.
Erosive tooth wear
Diagnosis
The clinical features of early erosive tooth wear (ETW) lesions in deciduous and young permanent teeth are probably the most difficult to diagnose as subtle changes on the relief of tooth surfaces must be identified. In particular, the clinician needs to observe the absence of the perichymata pattern from the facial aspect and the cingulum of maxillary anterior teeth seen from the palatal perspective,3 in addition to a less defined groove-fossa system on occlusal surfaces of premolars and molars. In deciduous teeth, the perichymata pattern is less defined than in young permanent teeth, which adds to difficulties in the diagnosis of early appearance of ETW lesions. Moreover, the enamel frequently acquires a rounded and shiny feature, generally observed from the facial and palatal perspective on maxillary anterior teeth, and on the marginal ridges, as well as on the cusps of the occlusal aspect of posterior teeth.3 Even in this early stage, a thin band of intact enamel at the gingival margin may be observed on the facial aspect of the maxillary incisors (Fig. 1B),4 provided the dental practitioner examines the dentition from the incisal perspective. The deciduous/permanent first molars are the earliest and seem to be the most severely attacked posterior teeth,5,6 probably due to the longer time of exposure in the mouth environment in comparison with deciduous/permanent second molars. Figure 1 shows these features in individual groups of teeth and surfaces in order to highlight the clinical characteristics of early signs of ETW lesions. ETW will also be illustrated later using the whole dentition of individual patients as a didactic platform.

The perichymata pattern is absent from the labial aspect of permanent maxillary incisors (a) while a thin band of intact enamel at the gingival margin indicates enamel loss on the rest of the surface (b). The occlusal surface of the deciduous first molar seems more severely eroded than the surface on the second deciduous molar. The palatal surface of the deciduous canine also shows eroded enamel (c)
Although possible, the diagnosis of subtle changes is, as expected, not straightforward. The inter-examiner reliability of diagnosis of early signs of ETW was recently tested in adolescents participating in a controlled clinical trial (Brazilian register number 1.096.882, unpublished data). Thirty patients, clinically diagnosed as either having this condition or not, were initially assessed by one examiner (JCC). Occlusal views of the patients' dentitions were then photographed, and further assessed by a second examiner (HDM). The inter-examiner reliability showed a non-weighted kappa value of 0.60 indicating only moderate agreement.7
Figure 2 illustrates early signs of erosive wear in deciduous dentition of a 5-year-old boy who had consumed soft drinks in a baby's bottle for an extended period of time. An enlarged view of the facial and palatal aspects of maxillary incisors shows a thin band of intact enamel at the gingival margin indicating ETW, combined with attrition of incisal edges. On the occlusal views, the enamel acquired a slight rounded and shiny feature on the marginal ridges.

The occlusal surface enamel of deciduous molars presents as slightly rounded and shiny on the marginal ridge (b and c)
The presence of cupping on occlusal surfaces is also a clinical feature of early ETW lesions.4 Dental practitioners should always try to diagnose such early signs when examining patients. The dentition of a 24-year-old female, who reported consuming soft drinks several times per week, showing a combination of erosive and abrasive wear on the buccal aspect of the dentition, is shown in Figure 3A. This case also shows cupping with different degrees of severity on the occlusal surfaces of the first permanent molars (Figs 3B and C).

The presence of cupping of different degrees of severity is seen on the occlusal surfaces of first permanent molars (b and c)
Further developed and more severe ETW lesions often present as a loss of the enamel on the palatal surfaces of maxillary anterior teeth in such a way that the incisal edges become more transparent and irregular. This may lead to a formation of a bluish shadow identified when the patient slightly opens the mouth. On the palatal aspect, a thin band of intact enamel at the gingival margin is readily identified together with the presence of cupping on occlusal surfaces of premolars and/or molars. Typically, restored areas on the occlusal surfaces of teeth are at a higher level than the surrounding dental tissue that has been eroded.8
Advanced ETW lesions on maxillary anterior teeth are characterised by reduced tooth height due to erosion of the incisal edges, most often combined with attrition. In general the incisal edges are irregular, and yellowish areas of exposed dentine may be present on facial surfaces.2 On eroded occlusal surfaces, the groove-fossa-system is no longer identifiable; the rounded contours of marginal ridges and cups are accompanied by localised exposure of the dentine.4 Bitewing radiographs may show a flat eroded occlusal surface compatible with erosion and/or attrition. Figure 4 shows a clinical case of a female suffering from bulimia who sought dental treatment due to the poor aesthetic appearance of her anterior teeth. The patient complained that her maxillary anterior teeth became 'small and yellowish'. The reader may observe that in this case even the distal surfaces of the maxillary premolars presented with ETW wear.

A yellowish area of exposed dentine on tooth 21 can be seen (arrow). Severe erosive lesions are located on the palatal aspect of the maxillary teeth (b). The occlusal surfaces of the premolars are eroded to a greater extent than the molars, compatible with acid impacts due to vomiting (b and c)
An important aspect of early ETW lesions diagnosis is their differentiation from other existing dental hard-tissue pathologies, in particular early dental caries lesions. These two common types of lesions present distinct aetiologies and may occur in the same patient at the same time, but not usually at the same location. While dental caries is mediated by the presence of a cariogenic biofilm, ETW lesions are associated with biofilm-free surfaces, as they develop from the direct contact between extrinsic/intrinsic acids and the tooth.9 As a result dental caries lesions are mostly confined to areas of biofilm accumulation, while erosive lesions may occur in any tooth surface subjected to intrinsic or extrinsic acids. In the latter the dissolution of the dental tissue occurs layer by layer as the surface tooth substance is etched away, as opposed to caries lesions where the bacterial acids only dissolve the tooth substance that is in direct contact with dental plaque.8
Following the oral clinical examination of patients, the dental practitioner should decide about the need to perform analysis of saliva. Measurements of the salivary flow is recommended for patients with symptoms of xerostomia, signs of hyposalivation, those that are treated with radiation in the head and neck or have general medical conditions and take medications that may affect the salivary flow.10
Risk assessment and management
The dental practitioner should combine the information obtained from both the anamnesis and the clinical examination in order to assess the risk of individual patients developing new ETW lesions and/or progression of existing lesions. More detailed information about patients' daily habits may be obtained by asking them to record their intake of foods, beverages, medications and use of oral health care products during four days and specifying the time points for intake/use of these.1 The findings of the complete risk assessment should be discussed with the patient.
The dental practitioner should take the time to discuss with their patients, children, adolescents and their parents as well as adults, their risk of developing new ETW lesions caused by extrinsic or intrinsic agents, based on the information collected at the individual level. The main idea is to establish realistic goals together with the patients/parents to eliminate or reduce as much as possible the episodes of erosive challenge. The patients must take responsibility for control of the erosion process in their own mouths and therefore need to understand how to proceed to achieve this goal.
Despite the evidence that most acidic beverages, foods and medicines present erosive potential, it does not always translate clinically into an erosive effect, or lead to the development of ETW lesions. For the dental practitioner it is important to realise that although the majority of cases of extrinsic erosion are associated with behavioural and lifestyle factors, some chemical and physical properties of acidic foodstuffs can influence their erosive effect. Low pH values have been considered the most important aspect of foods and drinks that cause erosion,11 but other characteristics should also be taken in account. There is some evidence to suggest recommending the intake of beverages supplemented with calcium as a substitute for normal soft drinks.12,13 Theoretically, the higher the calcium concentration the lower the potential erosive effect. This approach may be beneficial for patients who are reluctant to drink water or who complain about the counselling given, and should be considered as an additional measure to arrest the erosion process. The main question that remains is whether these patients will comply with this measure in the long term. However, there is a hypothetical risk of exceeding the tolerable upper limit (level that may cause adverse health effects) of calcium (2.5 g/day for children over one-year-old and adults), including increased risk of hypercalcaemia, kidney stones, and interference in the absorption of other minerals such as zinc, magnesium, and phosphorus.14
Most dietary acids are considered weak acids; however, citric acid is known to have greater erosive potential due to its ability to chelate the calcium from the saliva, and contributes to reducing the saturation of the oral fluids in the tooth surface.15 Examples of foods/drinks with citric acid are citric fruit juices (orange, lemon), soft drinks, canned foods, sports drinks, and iced teas. Drinks with high buffer capacity require more time for the saliva to neutralise the acid, thereby the teeth are eroded for longer periods of time.16 An example of a beverage with relatively high buffer capacity is orange juice. When compared to a cola drink, its buffering capacity is 5.5 times higher, despite its higher pH value (3.7 versus 2.7).17 This implies that within the first minutes of acid exposure, the cola drink would be more erosive; however, in prolonged acid challenges, the orange juice would have a more harmful effect. Prolonged exposure to acids may occur when the patient drinks a beverage in small sips over a long period of time, or when retaining the drink in the mouth for some time before swallowing. The temperature of the beverage is also important, as in vitro data have shown that higher temperatures can cause more erosion than lower temperatures, and patients at risk of erosion should therefore preferably drink cooled acidic beverages.18,19 The rate of tooth dissolution appears to be higher at higher fluid agitation in vitro, due to continuous renewal of the reagents participating in the chemical demineralisation reaction.20 In view of this, patients should avoid swirling the beverage around the mouth.
Patients with regular and frequent intake of acidic beverages run a higher risk of developing erosive lesions.21 In these cases, the first, and probably most important, message to be delivered is about the healthy habit of drinking water. Intake of water is important for hydration and suppressing thirst (mechanism involved in the fluid balance). We postulate that the intake of acidic beverages to suppress the body thirst's sensation has a very short-term effect. The sensation of thirst will reappear within a short span of time and the tendency is to repeatedly sip small amounts of acid beverages, and such provide multiple erosive challenges. Based on the reappearing sensation of thirst, some people may adopt the habit of having a can of acidic beverage at their side and drinking it independently of the time of day or activity being performed. In extreme cases, the consumption of soft drinks starts at breakfast and does not end before bed time, with no ingestion of water at all. Other factors such as the satisfaction of tasting acidic beverages and life style may equally play a role in the repeatedly intake of acid beverages on a daily basis. The deleterious consequences of frequent intake of acid beverages should in any case be addressed. From a health perspective, the benefits and advantages of drinking water should be a priority message from any governmental and non-governmental health agencies, including dental associations. Actions should be implemented at day care facilities, primary and high schools as well as nursery homes since many people are not well informed about the consequences of replacing water intake with acidic beverages.
The influence of age on erosion severity should also be underlined in particular for children, adolescents and young adults who are most concerned with the intake of acidic beverages, in order to keep their dentition functional throughout lifetime. If the patient does not present ETW lesions, and consequently his/her own mouth may not be used as an educational platform, pictures illustrating ETW lesions could be used taking into consideration different age groups and severity. Once diagnosed, the ETW lesions should be shown to the patients. Patients should look at their mouths using a hand mirror, while the dentist uses a mouth mirror to show them the lesions.
Dentine hypersensitivity can be associated with early ETW in adolescents and young adult patients. In addition to the total or at least partial removal of the possible causative agents, the clinician should take clinical photographs of the dentition, implement fluoride therapy (as described later), including the use of low abrasive dentifrices and establish regular visits to the dentist according to the individual needs of the patient. The benefits of recommending patients not to brush their teeth following the intake of acidic beverages or foods to allow remineralisation by the saliva and to prevent further tooth abrasion is still a matter of debate among researchers. Nevertheless, studies using intra-oral models have indicated that 1-2 hours of waiting periods before toothbrushing may help, although were not sufficient to completely prevent abrasion of the eroded enamel.22,23
Patients suffering from chronic medical conditions and taking regular oral medication with erosive potential should be informed about the risk of developing erosion lesions. They should be informed about the deleterious effect of intake of acid drinks to compensate for bitter taste medications or the reduced salivary flow possibly caused by tranquilisers, antihistamine, anti-emetic, anti-Parkinson, antidepressant, anti-hypertensive, antipsychotic or diuretic medications. Other factors such as prolonged and frequent ingestion of acidic medications, and bedtime and in-between meals consumption of these should be taken into account as this may increase the risk for medication-induced ETW. Considering the reported erosive potential of some analgesics,24 dentists should advise patients who habitually use soluble/chewable analgesics for chronic conditions to select analgesic options with no or minimal erosive potential or to change to tablets.
Acidic sweets are often consumed by sucking or licking as a means to alleviate symptoms of xerostomy or possibly hyposalivation. Patients suffering from xerostomia and/or hyposalivation may thus be at high risk of erosion25,26,27,28 and should be instructed to drink water whenever the symptoms appear and always have a small bottle of water available. The increased risk of erosion in these patients occurs because all salivary protective functions against erosion become compromised with reduced salivary flows.10 Patients treated with radiation in the head and neck area may suffer from severe impairment of the salivary glands with consequences for their (oral and general) quality of life.29 These patients may have difficulties eating dry food or even speaking. Drinking water in small sips during meals or even during a conversation may relieve these symptoms. Additional measures are required to control the rate of ETW progression in these cases. The use of saliva substitutes based on formulations with calcium phosphate and fluoride may give some relief to the symptoms and provide some protection against erosion as previously mentioned. It was also shown that chewing gum after an acid attack can stimulate the salivary flow and protect against erosive wear.30
Fluoride agents should also be considered for ETW management. High concentrated professionally applied fluoride products such as gels and varnishes may be options. However, for a patient with high frequency of acid exposure, the protection offered by these fluoride forms may be of short duration, requiring frequent application. Due to this fact, they are considered less cost-effective than the home-use products.31 Dentifrices can offer some protection against erosion, although relatively limited.27,32 Fluoridated solutions for mouth rinsing have also demonstrated some anti-erosive potential, mostly when the formulations are themselves acidic.33,34 The use of fluoridated products containing metal cations such as stannous fluoride have been shown to make the tooth surfaces less soluble, and has been considered a better approach to prevent erosion.31,35 Some of these dentifrices have polymers added to their formulation, such as sodium hexametaphosphate36 and chitosan, a natural organic polymer.37 These polymers have the ability to adsorb to the dental surfaces, thereby creating an additional protective layer against ETW. Moreover, low-abrasive dentifrices are indicated in cases of patients at moderate and higher risk of ETW.38
Professional wine tasters are a high risk group for developing erosion lesions due to the high frequency of erosive challenge they are exposed to over their working lifetime.39 Rinsing the mouth with water after each wine tasting is a simple measure to reduce the acid challenge, although the extent of the benefit this brings is unknown. Fluoride products should also be recommended on a regular basis for patients who are wine tasters in order to reduce the rate of erosion progression. These patients also need careful monitoring by their dental practitioner.
Patients suffering from alcoholism may also be in the high risk category for erosion due to frequent erosive challenge caused by acid of both extrinsic and intrinsic origin (for a review, see Schlueter and Tveit40 and Scaramucci et al.41). The complex treatment of alcohol addiction or any other type of drug addiction should involve a multidisciplinary approach, with the dentist being a member of the health professionals team. The same measures as for wine tasters are recommended, but patients' compliance may be difficult to obtain.
In any of the above-mentioned situations of erosive challenges the frequency of erosive exposure to teeth has a major role in the development of clinically identifiable erosive lesions. Advice on this aspect should also be given on an individual basis. However, as a general rule, the consumption of beverages and foods with erosive potential should preferably take place during meals. If indicated, patients' intake of medications with erosive potential should be discussed with the physician.
In patients with erosion caused by intrinsic acids, a suggested preventive approach is the use of agents that accelerate an increase in intra-oral pH after vomiting or heartburn, such as antacid tablets/suspensions or bicarbonate solution.42,43,44 For the more aggressive cases, for example, erosion lesions involving dentine, the use of resin-based materials to cover the eroded dentine, such as an adhesive was also been suggested. However, a clinical study involving a resin sealing system showed that the protection was limited to a period of three months.45 In an attempt to increase the survival rate of coatings, a more durable material, a fissure sealant, was also tested and found to reduce erosion progression for a period of up to nine months.46
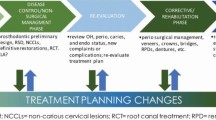
Collectively, all the measures described to arrest and/or to reduce the rate of erosion lesion progression, including sealing in rapidly progressing lesions, are considered as non-operative treatment for erosion and form the basis for any treatment of patients. Additionally, operative treatments may be required in cases of advanced erosion lesions associated with either dentine hypersensitivity, poor aesthetics or reduced tooth function. Composite resins are indicated as the restorative material in more severe erosion lesions though their retention may be particularly compromised in advanced erosion lesions. Onlay restorations and/or crowns are inevitable forms of treatment in the restoration of advanced ETW.
Monitoring
Regular monitoring of ETW should be carefully considered by the dentist and established on an individual basis. Appropriate documentation of the ETW arrest or progression will help confirm the aetiology of the lesion, but more importantly, will provide information on the efficacy of the measures implemented. Currently, the clinical assessment and monitoring of the occurrence as well as the severity of ETW can be performed by visual examination using clinical indices,47 or a series of good quality study casts or clinical photos. Many different indices have been proposed, and a recommendation for the use of a single method (the Basic Erosive Wear Examination, BEWE) has been made by experts in the area. This method uses a grading system, based on four scores (score 0: no erosion; 1: loss of enamel surface texture; 2: enamel loss of <50% of surface area; 3: enamel loss of >50% of surface area). However, as any other clinical index, it is subjective and it does not clearly differentiate early ETW lesion. Thus, efforts have been made to develop objective methods/clinical tools for the monitoring of ETW. While no clear consensus currently exists on appropriate objective methods, some have been reported to have potential, including optical coherence tomography,48,49 3D topographical analysis,50,51 as well as several other quantitative methods. Research advances in this field should be expected in the near future, facilitating the objective monitoring of ETW lesions.
Figure 5 shows a clinical case of a 14-year-old girl who underwent a routine clinical oral examination and who reported daily consumption of soft drinks. The most important signs of early erosive lesions are seen on the occlusal surfaces of the permanent first molars in which the groove-fossa-system was eroded, particularly in the mandibular teeth, in contrast to that of second permanent molars which appears almost intact. The patient was informed about ETW wear and aetiological factors associated with lifestyle. Photographs of the patient's own condition were shown as part of an educational platform and recommendation was given to drink water and at the same time minimise the consumption of soft drinks. The patient participated in an oral health programme, including toothbrushing with fluoride gel (1.23% F−) four times per year. Reassessment was carried out after one and two years. Clinical photographs were taken after two years. Comparing the clinical features of the ETW lesions did not show lesion progression, indicating success of the implemented management strategies.

On the palatal aspect of maxillary incisors, a very thin band of intact enamel can be seen at the gingival margin. Photographs taken at baseline examination (left) and two year follow-up (right). Monitoring of the patient does not indicate a progression of the erosive lesions
Conclusion
In summary, the clinical signs of early ETW lesions are subtle and may not be perceived as relevant by unaware clinicians. Emphasis should therefore be placed on the training of dentists and oral care providers to properly identify ETW at early stages. Clearly, the early diagnosis and implementation of non-operative management strategies, especially at younger ages, is fundamental for the proper control of ETW over time. Not all early signs of tooth wear will necessarily advance into ETW lesions, nevertheless a preventive approach based on patient education and preventive measures has shown to be clinically successful and should always be recommended.
References
Lussi A, Hellwig E . Risk assessment and causal preventive measures. Monogr Oral Sci 2014; 25: 220–229.
Schlueter N, Jaeggi T, Lussi A . Is dental erosion really a problem? Adv Dent Res 2012; 24: 68–71.
Larsen M L . Erosion of the teeth. In Fejeskov O, Kidd E A M (ed). Dental caries: the disease and its clinical management. 2nd ed. pp 234–247. Blackwell Munksgaard, 2008.
Ganss C, Lussi A . Diagnosis of erosive tooth wear. Monogr Oral Sci 2014; 25: 22–31.
Mulic A, Fredriksen Ø, Jacobsen I D, Tveit A B, Espelid I, Crossner C G . Dental erosion: Prevalence and severity among 16-year-old adolescents in Troms, Norway. Eur J Paediatr Dent 2016; 17: 197–201.
Tschammler C, Müller-Pflanz C, Attin T, Müller J, Wiegand A . Prevalence and risk factors of erosive tooth wear in 3–6 year old German kindergarten children – A comparison between 2004/05 and 2014/15. J Dent 2016; 52: 45–49.
Landis J R, Koch G G . The measurement of observer agreement for categorical data. Biometrics 1977; 33: 159–174.
Lussi A, Schlueter N, Rakhmatullina E, Ganss C . Dental erosion – An overview with emphasis on chemical and histopathological aspects. Caries Res 2011; 45: 2–12.
Lussi A, Carvalho T S . Erosive tooth wear: a multifactorial condition of growing concern and increasing knowledge. Monogr Oral Sci 2014; 25: 1–15.
Hara A T, Zero D T . The potential of saliva in protecting against dental erosion. Monogr Oral Science 2014; 25: 197–205.
Barbour M E, Lussi A, Shellis R P . Screening and prediction of erosive potential. Caries Res 2011; 45: 24–32.
Hara A T, Zero D T . Analysis of the erosive potential of calcium-containing acidic beverages. Eur J Oral Sci 2008; 116: 60–65.
Scaramucci T, Hara A T, Zero D T, Ferreira S S, Aoki I V, Sobral M A P . In vitro evaluation of the erosive potential of orange juice modified by food additives in enamel and dentine. J Dent 2011; 39: 841–848.
Straub D A . Calcium supplementation in clinical practice: a review of forms, doses, and indications. Nutr Clin Pract 2007; 22: 286–296.
Lussi A, Jaeggi T . Chemical factors. Monogr Oral Sci 2006; 20: 77–87.
Wang X, Lussi A . Assessment and management of dental erosion. Dent Clin North Am 2010; 54: 565–578.
Jensdottir T, Holbrook P, Nauntofte B, Buchwald C, Bardow A . Immediate erosive potential of cola drinks and orange juices. J Dent Res 2006; 85: 226–230.
West N X, Hughes J A, Addy M . Erosion of dentine and enamel in vitro by dietary acids: the effect of temperature, acid character, concentration and exposure time. J Oral Rehabil 2000; 27: 875–880.
Eisenburger M, Addy M . Influence of liquid temperature and flow rate on enamel erosion and surface softening. J Oral Rehabil 2003; 30: 1076–1080.
Shellis R P . The dental erosion process. In Amaechi (ed). Dental erosion and its clinical management. 1st ed. pp 13–33. Springer International Publishing, 2015.
Richards D . Impact of diet on tooth erosion. Evid Based Dent 2016; 17: 40.
Attin T, Knöfel S, Buchalla W, Tütüncü R . In situ evaluation of different remineralization periods to decrease brushing abrasion of demineralized enamel. Caries Res 35: 216–222.
Ganss C, Schlueter N, Friedrich D, Klimek J . Efficacy of waiting periods and topical fluoride treatment on toothbrush abrasion of eroded enamel in situ. Caries Res 2007; 41: 146–151.
Hellwig E, Lussi A . Oral hygiene products, medications and drugs – hidden aetiological factors for dental erosion. Monogr Oral Sci 2014; 25: 155–162.
Järvinen V, Rytömaa I, Heinonen O . Risk factors in dental erosion. J Dent Res 1991; 70: 942–947.
Young W, Khan F, Brandt R, Savage N, Razek A A, Huang Q . Syndromes with salivary dysfunction predispose to tooth wear: Case reports of congenital dysfunction of major salivary glands, Prader-Willi, congenital rubella, and Sjögren's syndromes. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001; 92: 38–48.
Scaramucci T, Borges A B, Lippert F, Frank N E, Hara A T . Sodium fluoride effect on erosion-abrasion under hyposalivatory simulating conditions. Arch Oral Biol 2013; 58: 1457–1463.
Borges A B, Scaramucci T, Lippert F, Zero D T, Hara A T . Erosion protection by calcium lactate/sodium fluoride rinses under different salivary flows in vitro. Caries Res 2014; 48: 193–199.
Turner M D, Ship J A . Dry mouth and its effects on the oral health of elderly people. J Am Dent Assoc 2007; 138: 15S–20S.
Rios D, Honório H M M, Magalhães A C et al. Effect of salivary stimulation on erosion of human and bovine enamel subjected or not to subsequent abrasion: An in situ/ex vivo study. Caries Res 2006; 40: 218–223.
Huysmans M C, Young A, Ganss C . The role of fluoride in erosion therapy. Monogr Oral Sci 2014; 25: 230–243.
Magalhães A C, Rios D, Delbem A C, Buzalaf M A, Machado M A . Influence of fluoride dentifrice on brushing abrasion of eroded human enamel: An in situ/ex vivo study. Caries Res 2007; 41: 77–79.
Wiegand A, Waldheim E, Sener B, Magalhães A C, Attin T . Comparison of the effects of TiF4 and NaF solutions at ph 1.2 and 3.5 on enamel erosion in vitro. Caries Res 2009; 43: 269–277.
Scaramucci T, Borges A B, Lippert F, Zero D T, Aoki I V, Hara A T . Anti-erosive properties of solutions containing fluoride and different film-forming agents. J Dent 2015; 43: 458–465.
Ganss C, Lussi A, Grunau O, Klimek J, Schlueter N . Conventional and anti-erosion fluoride toothpastes: Effect on enamel erosion and erosion-abrasion. Caries Res 2011; 45: 581–589.
Hooper S M, Newcombe R G, Faller R, Eversole S, Addy M, West N X . The protective effects of toothpaste against erosion by orange juice: Studies in situ and in vitro. J Dent 2007; 35: 476–481.
Ganss C, von Hinckeldey J, Tolle A, Schulze K, Klimek J, Schlueter N . Efficacy of the stannous ion and a biopolymer in toothpastes on enamel erosion/abrasion. J Dent 2012; 40: 1036–1043.
Magalhães A C, Wiegand A, Rios D, Honório H M, Buzalaf M A . Insights into preventive measures for dental erosion. J Appl Oral Sci 2009; 17: 75–86.
Mulic A, Tveit A B, Hove L H, Skaare A B . Dental erosive wear among Norwegian wine tasters. Acta Odontol Scand 2010; 69: 21–26.
Schlueter N, Tveit A B . Prevalence of erosive tooth wear in risk groups. Monogr Oral Sci 2014; 25: 74–98.
Scaramucci T, Carvalho J C, Hara A T, Zero D T . Causes of dental erosion: intrinsic factors. In Amaechi (ed.) Dental erosion and its clinical management. 1st ed. pp 35–67. Springer International Publishing, 2015.
Messias D C F, Turssi C P, Hara A T, Serra M C . Sodium bicarbonate solution as an anti-erosive agent against simulated endogenous erosion. Eur J Oral Sci 2010; 118: 385–388.
Lindquist B, Lingström P, Fändriks L, Birkhed D . Influence of five neutralizing products on intra-oral pH after rinsing with simulated gastric acid. Eur J Oral Sci 2011; 119: 301–304.
Turssi C P, Vianna L M F F, Hara AT, do Amaral F L B, França F M G, Basting R T . Counteractive effect of antacid suspensions on intrinsic dental erosion. Eur J Oral Sci 2012; 120: 349–352.
Sundaram G, Wilson R, Watson T F, Bartlett D . Clinical measurement of palatal tooth wear following coating by a resin sealing system. Oper Dent 2007; 32: 539–543.
Bartlett D, Sundaram G, Moazzez R . Trial of protective effect of fissure sealants, in vivo, on the palatal surfaces of anterior teeth, in patients suffering from erosion. J Dent 2011; 39: 26–29.
Ganss C, Lussi A . Diagnosis of erosive tooth wear. Monogr Oral Sci 2014; 25: 22–31.
Wilder-Smith C H, Wilder-Smith P, Kawakami-Wong H, Voronets J, Osann K, Lussi A . Quantification of dental erosions in patients with GERD using optical coherence tomography before and after double-blind, randomized treatment with esomeprazole or placebo. Am J Gastroenterol 2009; 104: 2788–2795.
Algarni A, Kang H, Fried D, Eckert G J, Hara A T . Enamel thickness determination by optical coherence tomography: in vitro validation. Caries Res 2016; 50: 400–406.
Tantbirojn D, Pintado M R, Versluis A, Dunn C, Delong R . Quantitative analysis of tooth surface loss associated with gastroesophageal reflux disease: a longitudinal clinical study. J Am Dent Assoc 2012; 143: 278–285.
Ahmed K, Whitters J, Ju X, Pierce S, MacLeod C, Murray C . Clinical monitoring of tooth wear progression in patients over a period of one year using CAD/CAM. Int J Prosthodont 2017; 30: 153–155.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Carvalho, J., Scaramucci, T., Aimée, N. et al. Early diagnosis and daily practice management of erosive tooth wear lesions. Br Dent J 224, 311–318 (2018). https://doi.org/10.1038/sj.bdj.2018.172
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2018.172
This article is cited by
-
Effect of arginine-fluoride varnish on preventing enamel erosion by paediatric liquid medicaments
BMC Oral Health (2023)
-
S-PRG-based composites erosive wear resistance and the effect on surrounding enamel
Scientific Reports (2022)
