
Abstract
Data on the management of atrial fibrillation (AF) in the Balkan Region are limited. The Serbian AF Association (SAFA) prospectively investigated contemporary ‘real-world’ AF management in clinical practice in Albania, Bosnia&Herzegovina, Bulgaria, Croatia, Montenegro, Romania and Serbia through a 14-week (December 2014-February 2015) prospective, multicentre survey of consecutive AF patients. We report the results pertinent to stroke prevention strategies. Of 2712 enrolled patients, 2663 (98.2%) with complete data were included in this analysis (mean age 69.1 ± 10.9 years, female 44.6%). Overall, 1960 patients (73.6%) received oral anticoagulants (OAC) and 762 (28.6%) received antiplatelet drugs. Of patients given OAC, 17.2% received non-vitamin K antagonist oral anticoagulants (NOACs). CHA2DS2-VASc score was not significantly associated with OAC use. Of the ‘truly low-risk’ patients (CHA2DS2-VASc = 0 [males], or 1 [females]) 56.5% received OAC. Time in Therapeutic Range (TTR) was available in only 18.7% of patients (mean TTR: 49.5% ± 22.3%). Age ≥ 80 years, prior myocardial infarction and paroxysmal AF were independent predictors of OAC non-use. Our survey shows a relatively high overall use of OAC in AF patients, but with low quality of vitamin K antagonist therapy and insufficient adherence to AF guidelines. Additional efforts are needed to improve AF-related thromboprophylaxis in clinical practice in the Balkan Region.
Similar content being viewed by others


Introduction
In parallel with increasing global burden of atrial fibrillation (AF), accumulating high-quality evidence from randomized clinical trials on AF management inform frequent updates of AF guidelines1. However, guideline implementation into daily clinical practice might be incomplete for many reasons and monitoring of routine practice through ongoing large, well-conducted long-term registries2,3 helps to understand and attenuate barriers for evidence-based management of AF in ‘real-world’ setting.
Recent reports from contemporary European AF registries have provided important insights into AF management in clinical practice2,3,4,5, including the observation of certain regional differences in management across Europe6. Most countries from the Balkan Region (comprising an area of >50 million inhabitants) were not participating in prior registries and in contrast to other European regions, ‘real-world’ data on the management of AF in Balkan countries are limited.
In this study, we investigated contemporary real-world patterns of AF management in the Balkan Region through a prospective 14-week survey of consecutive AF patients in clinical practice and we report the results pertinent to stroke prevention.
Methods
Study design and patient selection
A detailed report on the Balkan-AF study protocol has been published7. A 14-week prospective, multicentre ‘snapshot’ Balkan-AF survey of consecutive patients with electrocardiographically documented AF, who were seen by cardiologists or internal medicine specialists (in centres where a cardiologist was not available), was conducted from December 2014 to February 2015 in Albania, Bosnia & Herzegovina, Bulgaria, Croatia, Montenegro, Romania and Serbia (a total of ~40 million inhabitants). The survey was designed and conducted by the Serbian Atrial Fibrillation Association (SAFA), which is a non-profit multidisciplinary association of expert physicians involved in AF management and AF research.
The survey was announced to the National Cardiology Societies and relevant Working Groups or associations in Albania, Bosnia & Herzegovina, Bulgaria, Croatia, Former Yugoslav Republic Macedonia, Montenegro, Romania, Slovenia and Serbia. In the participating countries Balkan-AF survey was approved by the national and/or local Institutional Review Board, or the need for approval was waived according to the regulations in the respective country. In concordance with the local policy, a signed patient informed consent was obtained from each patient before enrolment. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
Each country participated with university and non-university hospitals and outpatient health centres in- and outside the capital cities. Patients younger than 18 years and patients with prosthetic mechanical heart valves or significant valve disease requiring surgical repair were not included.
Data collection
Data were collected via a web-based electronic case report form (CRF) with a range of pre-specified plausibility checks for the entries. The CRF was formulated to obtain the information on patients’ characteristics including demographics, cardiovascular risk factors, medical history, AF-related data regarding symptoms, prior history of AF, AF clinical type, prior use of antithrombotic medication, antiarrhythmic drugs or other therapies, health care setting (i.e., university/non-university health centre, in- or outside the capital city, in-hospital or outpatient, internal medicine specialist/cardiologist, main reason for current visit/hospitalization, emergency or non-emergency setting, length of hospitalization, etc.) and patient’s presentation, AF management at enrolling visit or hospitalization (i.e., medication, cardioversion, AF ablation) and further management strategy post discharge and diagnostic procedures performed due to AF during enrolling visit/hospitalization or within the last 12 months (the latter was not applicable to patients with first-diagnosed AF). A detailed list of cardiovascular risk factors, diseases and risk scores definitions used in the Balkan-AF survey is provided in the Supplementary Appendix 1.
Systematic monitoring of centres was not performed due to the relatively short duration of the survey. The national coordinators and all investigators are the guarantors of the consecutiveness of enrolment, accuracy and completeness of data. The CRF, patient files and medical records (paper or database) serve as source documents.
Statistical analysis
Following a test of statistical normality, continuous variables were presented as mean with standard deviation (SD), or with a skewed distribution as median with interquartile range (IQR, 25th–75th quartile). Categorical variables were reported as counts with percentages. The Student t-test was used for comparison of continuous variables with normal distribution and Mann-Whitney test for continuous variables with skewed distribution. Differences in categorical variables were tested by Chi-square test.
Univariate and multivariable logistic regression analyses were used to investigate the associations of variables shown in Table 1 (that is, demographic data, patient clinical characteristics and AF characteristics) and health care setting with the use of oral anticoagulants (OAC) and other antithrombotic therapies (that is, antiplatelet drugs), as prescribed at discharge from enrolling visit or hospitalization. Variables statistically significant on univariate analysis were entered into the multivariable model to identify independent predictors of OAC use. All analyses were adjusted for country code, to account for differences in the health care systems among the participating countries.
Because the main reason for enrolling visit or hospitalization could have been either AF or some other condition, we have performed two sensitivity analyses. First, we excluded patients seen for other reasons (in whom the use of OAC might have been influenced by other condition) and performed the analysis of OAC use as in the main cohort. Second, we excluded patients presenting with an acute coronary syndrome and then performed the OAC use analyses in the rest of the main cohort.
All results are reported as Odds Ratio (OR) with 95% Confidence Interval (CI). All statistical analyses were performed using SPSS 20.0 software package (SPSS Inc., Chicago, Illinois). A two-sided P value of <0.05 was considered statistically significant.
Results
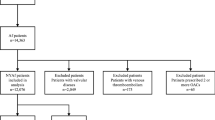
A total of 2712 patients were enrolled in 49 centres from seven Balkan countries; 27 centres (55.1%) were university hospitals enrolling 2161 patients (86.6%). Eighteen centres (36.7%) were situated in the capital cities and enrolled 1241 patients (45.8%). A total of 2147 patients (79.2%) were enrolled by cardiologists and 717 patients (26.8%) were seen in outpatient setting. Full data on antithrombotic therapy prescribed at current visit/hospitalization were available in 2663 patients (98.2%) and those patients were included in this analysis.
Demographic data (mean age 69.1 ± 10.9 years, range 18–96; female 44.6%), clinical characteristics of the study population and AF characteristics are shown in Table 1.
Stroke and bleeding risk profile
Mean CHA2DS2-VASc score was 3.48 ± 1.77 (range 0–9, median 3.0, IQR 2.0–5.0) and a score of ≥2 was present in 2290 patients (86.0%). The mean CHADS2 score was 2.15 ± 1.29 (≥2 in 65.6% of patients) and mean HASBLED score was 1.97 ± 1.23 (range 0–6). Country-specific stroke and bleeding risk distribution is shown in Table 1, Fig. 1 and Supplemental Table 1.

Stroke and bleeding risk.
‘Truly low-risk’: CHA2DS2-VASc = 0 in males, or CHA2DS2-VASc = 1 in females; B&H: Bosnia & Herzegovina.
Antithrombotic therapies
Country-specific distribution of antithrombotic therapies is shown in Table 2. Overall, 264 patients (9.9%) were not given any antithrombotic therapy, 1960 patients (73.6%) were prescribed OAC and 762 patients (28.6%) received an antiplatelet drug. OAC as only antithrombotic drug was given to 1637 patients (61.5%), whilst an antiplatelet drug only was given to 320 patients (12.0% and in 91.2% of patients that was aspirin).
NOACs (i.e., dabigatran, rivaroxaban or apixaban) were given to 338 patients (12.7% of the whole study population or 17.2% of patients receiving OAC).
One patient previously underwent a left atrial appendage closure device implantation.
Adherence to guidelines
The proportions of OAC and other antithrombotic therapies by CHA2DS2-VASc and HASBLED score strata are shown in Fig. 2.

The use of antithrombotic therapies by CHA2DS2-VASc and HASBLED risk strata.
APLT: antiplatelet therapy; DAPT: dual antiplatelet therapy; OAC: oral anticoagulant.
In the ‘truly’ low-risk group (that is, CHA2DS2-VASc score of 0 in males, or 1 in females) only 44 patients (33.6%) were not given any antithrombotic therapy, whilst 74 patients (56.5%) received OAC and 18 patients (13.7%) received an antiplatelet therapy, alone or in combination with OAC (3.8%). The use of OAC in ‘truly’ low-risk patients could be attributed to planned cardioversion or AF catheter ablation in only 21 patients (16.0%).
Of 2290 patients with CHA2DS2-VASc ≥2, 194 (8.5%) received no antithrombotic therapy, 1401 (61.2%) were given OAC only and 393 patients (17.2%) received an antiplatelet drug alone. A combination of OAC and an antiplatelet drug was given to 302 patients (13.2%).
There was no significant association between the CHA2DS2-VASc score and OAC prescription on multivariate analysis (Table 3). The non-relationship to CHADS2 score was similar (OR 1.06; 95% CI, 0.98–1.13, p = 0.119). The use of OAC increased with increasing HASBLED score, but the difference was significant only on univariate analysis (p = 0.042), Table 3.
The use of antiplatelet drugs was significantly associated with CHA2DS2-VASc score only on univariate analysis (Table 3).
Determinants of OAC use
Independent predictors of the use of antithrombotic therapies are shown in Table 3, including significant univariate associations with the use of OAC or antiplatelet drug only (full univariate analyses list is shown in Supplemental Table 2).
OAC monotherapy
On univariate analysis, most of the CHA2DS2-VASc score components were not significantly associated with OAC use, including prior stroke (OR 1.02; 0.76–1.37; p = 0.878). Patients with hypertension were more likely to use OAC, whilst older age (≥80 years) and coronary artery disease (CAD) were inversely associated with OAC use (Supplemental Table 2).
Increasing body mass index (BMI), mitral valve disease, dilated cardiomyopathy and thyroid disease were associated with increased use of OAC, whilst patients with chronic kidney disease (CKD) on dialysis and patients with chronic obstructive pulmonary disease (COPD) were less likely to use OAC (Supplemental Table 2).
The proportions of OAC use according to AF clinical type are shown in Fig. 3. Known history of AF was associated with increased use of OAC, whilst patients with paroxysmal AF were less likely to receive OAC. Patients treated in the health centres situated in the capital city or in university centres and patients managed by a cardiologist were more likely to use OAC compared to other patients (Supplemental Table 2).

The use of oral anticoagulation by AF clinical type.
APLT: antiplatelet therapy; OAC: oral anticoagulant.
Independent predictors of OAC use were hypertension, mitral valve disease, dilated cardiomyopathy, known history of AF and treatment in the capital city health centres, whilst age ≥80 years, prior MI and paroxysmal AF were independent predictors of OAC non-use (Table 3).
Antiplatelet drug (aspirin) monotherapy
Independent predictors of aspirin monotherapy were age ≥80 years, CAD, aortic valve disease, COPD and paroxysmal AF, whilst BMI, known history of AF and treatment in the capital city health centre or treatment by a cardiologist were negatively associated with aspirin use (Table 3). On univariate analysis, increasing CHA2DS2-VASc score and prior transient ischemic attack (TIA) were also associated with increased use of aspirin only (Table 3).
Other antithrombotic therapies
Independent predictors of dual antiplatelet drug therapy (DAPT) use were PCI, any CAD, COPD and paroxysmal AF, whilst patients with known history of AF were less likely to receive DAPT (Table 3). Independent predictors of the use of OAC combined with one or two antiplatelet drugs were CAD, PCI and treatment in a hospital-based centre, whilst patients aged ≥80 years were less likely to be given such therapy. Increasing HASBLED score was positively associated with the use of combined therapy (Table 3).
Indices of VKA anticoagulation quality
An International Normalized Ratio (INR) obtained within previous 3 weeks was available in 946 (79.0%) of 1198 patients who were previously taking a VKA for at least 6 months or longer. The most recent INR value ranged from 1 to 10 (mean 2.42, SD 1.0, median 2.28) and was within the target range of 2.0 to 3.0 in 522 patients (55.2%) whilst in 281 (29.5%) and 143 patients (15.1%) the INR was below and above the target range, respectively.
The Time in Therapeutic Range (TTR) from the previous 3 months was available in only 224 patients (18.7%). Mean TTR was 49.5% ± 22.3% (median 50.0%, range 10–100%) and only 66 patients (29.5%) had a TTR of ≥65%. Labile INR was reported in 439 patients (36.6%) in whom TTR was not available.
Sensitivity analyses
AF was the main reason for enrolling visit or hospitalization in 1329 patients (49.9%). Compared to the main cohort, these patients were younger (mean age 66.9 ± 11.3 years), with lower CHA2DS2-VASc (mean 2.95 ± 1.74) and lower HASBLED score (1.72 ± 1.19), all p < 0.01. OAC was given to 1000 patients (75.2%). Univariate and multivariable determinants of OAC use in patients with AF as the main reason for enrolling visit or hospitalization are shown in Supplemental Table 4. Similar to the main cohort, there was no significant relationship between the CHA2DS2-VASc score and the use of OAC in the multivariable analysis. The use of OAC was driven by the presence of hypertension, younger age (<75 years), increasing BMI, non-cardiac comorbidities (thyroid disease), centre localization (capital city) and university centre type, whilst patients with COPD, malignancy and paroxysmal AF were less likely to be prescribed OAC (Supplemental Table 4).
An acute coronary syndrome was the main reason for enrolling hospitalization in 206 patients (7.7%) and they were excluded from this analysis. In the remaining cohort of 2457 patients (mean age 68.9 ± 11.0 years, mean CHA2DS2-VASc 3.42 ± 1.77, mean HASBLED 1.97 ± 1.23) OAC was prescribed to 1843 patients (75.0%) and the use of OAC was driven by broadly similar determinants as in the main cohort (Supplemental Table 5).
Discussion
This snapshot survey provides, for the first time, a contemporary insight into routine clinical practice in AF management from a large region of Europe where data on AF management are generally scarce, especially since countries participating in this survey were largely under-represented in recent European AF surveys2,4,5. This survey therefore complements the European AF data and reduces a gap in the European ‘map’ of contemporary real-world management of AF.
Our findings suggest that the overall use of OAC for stroke prevention in the Balkan region is relatively high (~74%), but poorly associated with individual patient stroke risk as recommended by the European Society of Cardiology guidelines1. Whilst mostly VKA were used, the quality of anticoagulation was poor, with less than a third of patients having a TTR of ≥65%. Overall, the use of NOACs was slightly higher than recently reported in a ‘real-world’ European survey3 and the use of antiplatelet drugs was comparably high as in other parts of Europe. We also observed significant differences in the use of antithrombotic therapies according to the physician specialty and health centre location. Our results have important practical implications and may help in recognizing the ‘action points’ needed to improve the management of AF patients at risk of stroke in daily clinical practice in the Balkan region.
The Balkan-AF cohort stroke risk profile was broadly similar to recent data from the EURObservational Pilot AF Registry3, with some minor differences (e.g., hypertension, diabetes mellitus and prior stroke were slightly more prevalent, whilst CAD, HF and valvular disease were slightly less frequent in the Balkan-AF cohort). However, bleeding risk was higher and the difference might possibly be driven by labile INRs in many patients.
The overall use of OAC in Balkan-AF cohort was close to that in recent European reports3,4, but was not significantly associated with CHA2DS2-VASc score, even when categorised to <2 vs. ≥2. Despite clear evidence of low stroke risk in male AF patients with a CHA2DS2-VASc score of 0 and those with a score of 1 due to female sex8,9,10,11,12, in whom no antithrombotic therapy is recommended1, as many as 56.5% of such patients in the Balkan-AF cohort received OAC despite only a minority being scheduled for cardioversion or AF ablation.
Some deviations from evidence-based stroke prevention strategies were evident in the Balkan-AF cohort. For example, elderly patients were more likely to receive aspirin, despite clear evidence of net benefit with OAC in elderly13,14. Also, patients with stable CAD were more likely to receive aspirin or DAPT, or OAC plus antiplatelet drugs instead of OAC monotherapy, although evidence showed that combining OAC with antiplatelet drugs in AF patients with stable vascular disease resulted only in increased risk of major bleeding with no additional reduction of thromboembolism15,16. Such patterns of OAC use were also noted in other European countries6.
Independent predictors of increased OAC use in the Balkan-AF survey were hypertension, dilated cardiomyopathy and mild-to-moderate mitral valve disease (essentially mitral regurgitation). In contrast to mitral stenosis, data on the risk of stroke in AF patients with mitral regurgitation are controversial17 and decisions on OAC should be driven by the presence of well documented stroke risk factors.
The ‘chronicity’ of AF strongly influenced OAC use in the Balkan-AF cohort, with a 56% lower probability for OAC in paroxysmal AF and a 49% greater probability of OAC therapy in patients with history of AF. A large body of evidence suggests that stroke risk is comparable with paroxysmal or permanent AF18,19. Recently, this has been challenged by a meta-analysis of two non-anticoagulated AF cohorts with systematically adjudicated adverse events which showed AF type to be a strong independent predictor of stroke20, but the annual stroke rate with paroxysmal AF was still sufficiently high (2.1%) to warrant OAC therapy1. Hence, the decision on OAC should be guided by the presence of conventional stroke risk factors.
The use of aspirin alone was high across all CHA2DS2-VASc score strata and increased from 10% to 17.2% with increasing score. Despite sufficient evidence of only modest efficacy and similar safety compared to OAC13,14, aspirin is still used as monotherapy in around 15% of AF patients in Europe2. Independent predictors of aspirin use in the Balkan-AF survey (i.e., advanced age, paroxysmal AF, COPD, mild-to-moderate aortic valve disease) likely reflect a mixture of misperceptions of aspirin better safety (e.g., in elderly) or of lower stroke risk (e.g., paroxysmal AF, COPD, etc.) and an unjustified favouring of aspirin over OAC (e.g., in patients with stable CAD or aortic valve disease).
However, the HASBLED score was not a significant determinant of OAC use in our cohort (indeed, the use of OAC increased with increasing HASBLED), suggesting that either the role of HASBLED was correctly interpreted (that is, the score was used to flag up modifiable bleeding risk factors and not to preclude OAC use) or perhaps the score was ignored. The latter seems to be the case particularly with the use of combined OAC plus antiplatelet drug therapy, which increased with increasing HASBLED score. Alternatively, sicker patients might have needed such therapy more often.
Around 80% of AF patients in our survey were managed by a cardiologist and these patients were less likely to receive aspirin. Patients managed in health centres in the capital cities less often received aspirin and more often were given OAC, the latter likely resulting from the clustering of tertiary health centres in the capital cities in most of participating countries. Of note, similar influence of clinical background and specialty of treating physicians on antithrombotic treatment strategies in AF patients has been also described in other European countries21. However, the availability of a cardiologist with proper level of expertise for stroke risk management in AF patients in real-world clinical practice may significantly differ among countries.
The signal of poor quality of anticoagulation with VKA in the Balkan-AF cohort (as reflected by a low proportion of patients with a TTR of ≥65% and high proportion of patients with labile INRs) is particularly worrisome and calls for urgent action, as suboptimal TTR (<65–70%) is associated with an excess of both stroke and bleeding (and mortality)15,22,23. Indeed, a TTR of >70% is recommended in guidelines and position documents, when VKAs are used15. Also, missing TTR in >80% of patients in the Balkan-AF cohort might indicate that the calculation of TTR is not commonly used in routine clinical practice in Balkan countries. Given the low quality of therapy with VKA compared to other European countries24, increasing use of NOACs (17% of all patients taking OAC) is encouraging, as it could facilitate adequate stroke prevention in Balkan countries. An analysis of factors influencing the choice of NOAC over VKA in Balkan countries is underway.
This study is limited by its observational snapshot registry design, but we made every effort to include consecutive patients. Although we tried to capture a sample representative of real-world clinical practice by recruiting a range of different types of centres in each country (i.e., university and non-university hospitals and outpatient centres in- and outside the capital cities), there still may be a selection bias due to variable health care setting in the participating countries.
The proportion of cardiologists versus internal medicine specialists participating in the Balkan-AF survey may not fully reflect daily practice in the participating countries, since we might have not adequately covered the rural areas. Still, participating centres situated outside capital cities enrolled about 55% of patients and in smaller countries many AF patients are often referred to the tertiary centres at least for initial evaluation.
Since TTR was available in a small proportion of patients treated with OAC, our results may under- or overestimate the quality of VKA treatment in our cohort and we cannot conclude whether or not VKA therapy is systematically monitored in clinical practice.
Conclusion
This survey provide important insights into contemporary routine practices for stroke prevention in AF patients in Balkan countries, thus reducing a gap in the European ‘map’ of contemporary real world management of AF. Our results show a broadly similar patient stroke risk profile in the Balkan Region and similar OAC use as in other European countries. However, routine practices for stroke prevention in AF patients in Balkan countries are less influenced by the presence of conventional well documented stroke risk factors in AF patients and the quality of VKA therapy is low. Thus, additional efforts are needed to increase the adherence to AF guidelines and improve the management of AF-related risk of stroke in routine clinical practice in the Balkan Region.
Additional Information
How to cite this article: Potpara, T. S. et al. Stroke prevention in atrial fibrillation and ‘real world’ adherence to guidelines in the Balkan Region: The BALKAN-AF Survey. Sci. Rep. 6, 20432; doi: 10.1038/srep20432 (2016).
References
Camm, A. J. et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J 33, 2719–47 (2012).
Lip, G. Y. et al. A prospective survey in European Society of Cardiology member countries of atrial fibrillation management: baseline results of EURObservational Research Programme Atrial Fibrillation (EORP-AF) Pilot General Registry. Europace 16, 308–19 (2014).
Lip, G. Y. et al. Prognosis and treatment of atrial fibrillation patients by European cardiologists: one year follow-up of the EURObservational Research Programme-Atrial Fibrillation General Registry Pilot Phase (EORP-AF Pilot registry). Eur Heart J 35, 3365–76 (2014).
Kirchhof, P. et al. Management of atrial fibrillation in seven European countries after the publication of the 2010 ESC Guidelines on atrial fibrillation: primary results of the PREvention oF thromboemolic events–European Registry in Atrial Fibrillation (PREFER in AF). Europace 16, 6–14 (2014).
Arbelo, E. et al. The atrial fibrillation ablation pilot study: a European Survey on Methodology and results of catheter ablation for atrial fibrillation conducted by the European Heart Rhythm Association. Eur Heart J 35, 1466–78 (2014).
Lip, G. Y. et al. Regional differences in presentation and treatment of patients with atrial fibrillation in Europe: a report from the EURObservational Research Programme Atrial Fibrillation (EORP-AF) Pilot General Registry. Europace 17, 194–206 (2015).
Potpara, T. S., Balkan, A. F. I. & Lip, G. Y. Patterns in atrial fibrillation management and ‘real-world’ adherence to guidelines in the Balkan Region: an overview of the Balkan-atrial fibrillation survey. Eur Heart J 36, 1943–4 (2015).
Olesen, J. B., Torp-Pedersen, C., Hansen, M. L. & Lip, G. Y. The value of the CHA2DS2-VASc score for refining stroke risk stratification in patients with atrial fibrillation with a CHADS2 score 0-1: a nationwide cohort study. Thromb Haemost 107, 1172–9 (2012).
Olesen, J. B. et al. Risks of thromboembolism and bleeding with thromboprophylaxis in patients with atrial fibrillation: A net clinical benefit analysis using a ‘real world’ nationwide cohort study. Thrombosis and Haemostasis 106, 739–749 (2011).
Friberg, L., Rosenqvist, M. & Lip, G. Y. Net clinical benefit of warfarin in patients with atrial fibrillation: a report from the Swedish atrial fibrillation cohort study. Circulation 125, 2298–307 (2012).
Potpara, T. S. et al. A 12-year follow-up study of patients with newly diagnosed lone atrial fibrillation: implications of arrhythmia progression on prognosis: the Belgrade Atrial Fibrillation study. Chest 141, 339–47 (2012).
Lip, G. Y. Stroke and bleeding risk assessment in atrial fibrillation: when, how and why? Eur Heart J 34, 1041–9 (2013).
Mant, J. et al. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet 370, 493–503 (2007).
Connolly, S. J. et al. Apixaban in patients with atrial fibrillation. N Engl J Med 364, 806–17 (2011).
De Caterina, R. et al. Vitamin K antagonists in heart disease: current status and perspectives (Section III). Position paper of the ESC Working Group on Thrombosis–Task Force on Anticoagulants in Heart Disease. Thromb Haemost 110, 1087–107 (2013).
Bernard, A. et al. Anticoagulation in patients with atrial fibrillation undergoing coronary stent implantation. Thromb Haemost 110, 560–8 (2013).
De Caterina, R. & Camm, A. J. What is ‘valvular’ atrial fibrillation? A reappraisal. Eur Heart J 35, 3328–35 (2014).
Hart, R. G. et al. Stroke with intermittent atrial fibrillation: incidence and predictors during aspirin therapy. Stroke Prevention in Atrial Fibrillation Investigators. J Am Coll Cardiol 35, 183–7 (2000).
Friberg, L., Hammar, N. & Rosenqvist, M. Stroke in paroxysmal atrial fibrillation: report from the Stockholm Cohort of Atrial Fibrillation. Eur Heart J 31, 967–75 (2010).
Vanassche, T. et al. Risk of ischaemic stroke according to pattern of atrial fibrillation: analysis of 6563 aspirin-treated patients in ACTIVE-A and AVERROES. Eur Heart J 36, 281–7a (2015).
Kirchhof, P. et al. Impact of the type of centre on management of AF patients: surprising evidence for differences in antithrombotic therapy decisions. Thromb Haemost 105, 1010–23 (2011).
Gallagher, A. M., Setakis, E., Plumb, J. M., Clemens, A. & van Staa, T. P. Risks of stroke and mortality associated with suboptimal anticoagulation in atrial fibrillation patients. Thromb Haemost 106, 968–77 (2011).
Gallego, P. et al. Cessation of oral anticoagulation in relation to mortality and the risk of thrombotic events in patients with atrial fibrillation. Thromb Haemost 110, 1189–98 (2013).
Le Heuzey, J. Y. et al. Differences among western European countries in anticoagulation management of atrial fibrillation. Data from the PREFER IN AF registry. Thromb Haemost 111, 833–41 (2014).
Acknowledgements
We thank all Balkan-AF investigators and Ms Zlatiborka Mijatovic for their hard work and contribution.
Author information
Authors and Affiliations
Consortia
Contributions
T.S.P. study design, data collection, data analysis, writing of the manuscript, MMP: eCRF development, data collection, manuscript review, G.A.D., E.T., A.G., Z.K., S.M. and L.J.M. coordinating the study, data collection, manuscript reviewing, R.M., E.B., G.M., V.P., E.S.D., S.L.P., H.D.J., D.L., A.B. & S.B. data collection, manuscript reviewing, GYHL: study design, data analysis and interpretation, writing of the manuscript. The BALKAN-AF Investigators: data collection.
Ethics declarations
Competing interests
TSP: speaker fees from Pfizer and Bayer; MMP: no conflicts of interest to declare; GAD: speaker fees from Boehringer Ingelheim; ET: speaker fees from Bayer, Pfizer, Boehringer Ingelheim, Astra Zeneca, Servier, Merck Serono, Gedeon Richter, Actavis, Berlin Chemie; AG, ZK, SM: no conflicts of interest to declare; LjM: speaker fees from Bayer and Boehringer Ingelheim; RM: no conflicts of interest to declare; EB: speaker fees from Astra Zeneca, Berlin Chemie, Pfizer, Antibiotice Iasi, Gedeon Richter; GM: speaker fees from Pfizer and Boehringer Ingelheim; VP, ESD, SLP, HDj, DL, AB: no conflicts of interest to declare; SB: speaker fees from Bayer, Pfizer, Boehringer Ingelheim; GYHL: consultant fees from Bayer, Merck, Sanofi, BMS/Pfizer, Daiitchi-Sankyo, Biotronic, Medtronic, Portola and Boehringer Ingelheim and speaker fees from Bayer, BMS/Pfizer, Boehringer Ingelheim, Daiitchi-Sankyo, Medtronic.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Potpara, T., Dan, GA., Trendafilova, E. et al. Stroke prevention in atrial fibrillation and ‘real world’ adherence to guidelines in the Balkan Region: The BALKAN-AF Survey. Sci Rep 6, 20432 (2016). https://doi.org/10.1038/srep20432
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep20432
This article is cited by
-
Cost-effectiveness of a photopethysmographic procedure for screening for atrial fibrillation in 6 European countries
Health Economics Review (2022)
-
Non-adherence to Thromboprophylaxis Guidelines in Atrial Fibrillation: A Narrative Review of the Extent of and Factors in Guideline Non-adherence
American Journal of Cardiovascular Drugs (2021)
-
Decision-Making in Clinical Practice: Oral Anticoagulant Therapy in Patients with Non-valvular Atrial Fibrillation and a Single Additional Stroke Risk Factor
Advances in Therapy (2017)
-
The Patterns of Non-vitamin K Antagonist Oral Anticoagulants (NOACs) Use in Patients with Atrial Fibrillation in Seven Balkan Countries: a Report from the BALKAN-AF Survey
Advances in Therapy (2017)
-
Adherence to antithrombotic therapy guidelines improves mortality among elderly patients with atrial fibrillation: insights from the REPOSI study
Clinical Research in Cardiology (2016)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
